Download as pdf or txt
You might also like
- ISO 11607-1 2019 Packaging For Terminally Sterilized MDDocument52 pagesISO 11607-1 2019 Packaging For Terminally Sterilized MD960213100% (1)
- Pediatric Obesity AlgorithmDocument14 pagesPediatric Obesity AlgorithmSyarifah Maharani HidayatNo ratings yet
- Evaluating Mid Upper Arm Circumference Z Score As A Determinant of Nutrition Status Stephens2018Document9 pagesEvaluating Mid Upper Arm Circumference Z Score As A Determinant of Nutrition Status Stephens2018Oscar Hernan Tellez SantosNo ratings yet
- An Obesity Risk Assessment Tool For Young Childr 2018 Journal of Nutrition EDocument13 pagesAn Obesity Risk Assessment Tool For Young Childr 2018 Journal of Nutrition EErik agustioNo ratings yet
- Early Obesity Prevention - A Randomized Trial ofDocument7 pagesEarly Obesity Prevention - A Randomized Trial ofClaudia Rodrigues DiasNo ratings yet
- Pediatric Obesityassessment Treatment and Prevention An Endocrin 2017Document49 pagesPediatric Obesityassessment Treatment and Prevention An Endocrin 2017Elena NicaNo ratings yet
- Evaluation of A Community-Based Weight Management Program ForDocument13 pagesEvaluation of A Community-Based Weight Management Program ForRaquel BoffNo ratings yet
- Characteristics of Children 2 To 5 Years of Age With Severe ObesityDocument10 pagesCharacteristics of Children 2 To 5 Years of Age With Severe ObesityIvan BurgosNo ratings yet
- Pediatric Obesity - Assessment, Treatment, and Prevention-An Endocrine Society Clinical Practice Guideline 2017Document49 pagesPediatric Obesity - Assessment, Treatment, and Prevention-An Endocrine Society Clinical Practice Guideline 2017Filipa FigueiredoNo ratings yet
- A.S.P.E.N. Clinical Guidelines Nutrition Support of Children With Human Immunodeficiency Virus InfectionDocument19 pagesA.S.P.E.N. Clinical Guidelines Nutrition Support of Children With Human Immunodeficiency Virus Infectionmededep273No ratings yet
- Fnut 11 1270048Document16 pagesFnut 11 1270048vivianelimaliveNo ratings yet
- Clinical Endocrinology - 2021 - Apperley - Childhood obesity A review of current and future management optionsDocument14 pagesClinical Endocrinology - 2021 - Apperley - Childhood obesity A review of current and future management optionsdoctoramassuh.endocrinopediaNo ratings yet
- STAMP (Kids)Document8 pagesSTAMP (Kids)Rika LedyNo ratings yet
- GLIM Criteria For The Diagnosis of Malnutrition A Consensus Report From The Global Clinical Nutrition CommunityDocument9 pagesGLIM Criteria For The Diagnosis of Malnutrition A Consensus Report From The Global Clinical Nutrition CommunityRomer Juanez AramayoNo ratings yet
- Randomized Controlled Trial of A Primary Care-Based Child Obesity Prevention Intervention On Infant Feeding PracticesDocument9 pagesRandomized Controlled Trial of A Primary Care-Based Child Obesity Prevention Intervention On Infant Feeding PracticesSardono WidinugrohoNo ratings yet
- Adc 96 11 1008Document6 pagesAdc 96 11 1008Sri Widia NingsihNo ratings yet
- Childhood Obesity-Knowledge, Attitudes, and Practices of European Pediatric Care Providers (Pediatrics2013)Document11 pagesChildhood Obesity-Knowledge, Attitudes, and Practices of European Pediatric Care Providers (Pediatrics2013)jose matosNo ratings yet
- An Intensive Family Intervention Clinic For Reducing Childhood ObesityDocument8 pagesAn Intensive Family Intervention Clinic For Reducing Childhood ObesityFarha AamirNo ratings yet
- Bouma 2016Document16 pagesBouma 2016Eugenia BocaNo ratings yet
- A Randomized, Controlled Trial of Liraglutide For Adolescents With ObesityDocument12 pagesA Randomized, Controlled Trial of Liraglutide For Adolescents With ObesityJosé Luis ChavesNo ratings yet
- Guidelines For Nutritional Care of Preterm InfantsDocument7 pagesGuidelines For Nutritional Care of Preterm InfantsA. Berenice GarcíaNo ratings yet
- Routine Amoxicillin For Uncomplicated Severe Acute Malnutrition in ChildrenDocument10 pagesRoutine Amoxicillin For Uncomplicated Severe Acute Malnutrition in ChildrenMc'onethree BrownNo ratings yet
- Clinical Nutrition: ESPEN Endorsed RecommendationDocument9 pagesClinical Nutrition: ESPEN Endorsed RecommendationjavierNo ratings yet
- Educacion en Adultos Con DMT2Document1 pageEducacion en Adultos Con DMT2Rafael Enrique Castellar MartinezNo ratings yet
- GPC Pediatric Obesity Assessment Treatment 2017Document49 pagesGPC Pediatric Obesity Assessment Treatment 2017Laura GarzónNo ratings yet
- Do Practice Nurses Have The Knowledge To Provide Diabetes Self-Management Education?Document9 pagesDo Practice Nurses Have The Knowledge To Provide Diabetes Self-Management Education?Macarena MartínezNo ratings yet
- Dr. Piyush Ranjan, Department of Medicine, AIIMS, January (2019)Document21 pagesDr. Piyush Ranjan, Department of Medicine, AIIMS, January (2019)Sree LathaNo ratings yet
- Assestment ObesDocument49 pagesAssestment Obesstockholms 2020No ratings yet
- Sdarticle 142 PDFDocument1 pageSdarticle 142 PDFRio Michelle CorralesNo ratings yet
- Pediatric Metabolic and Bariatric Surgery - Evidence, Barriers, and Best PracticesDocument10 pagesPediatric Metabolic and Bariatric Surgery - Evidence, Barriers, and Best PracticesConsultorio Pediatria ShaioNo ratings yet
- Endoscopic Sleeve Gastroplasty As An Early Tool Against Obesity: A Multicenter International Study On An Overweight PopulationDocument6 pagesEndoscopic Sleeve Gastroplasty As An Early Tool Against Obesity: A Multicenter International Study On An Overweight PopulationduranaxelNo ratings yet
- Pediatric Obesity - Assessment, Treatment, and Prevention: An Endocrine Society Clinical Practice GuidelineDocument49 pagesPediatric Obesity - Assessment, Treatment, and Prevention: An Endocrine Society Clinical Practice GuidelineLiza ApseraNo ratings yet
- Woobaidal 2016Document19 pagesWoobaidal 2016Visa LaserNo ratings yet
- Comparison of Malnutrition and Malnutrition Screening Tools in Pediatric Oncology Patients A Cross-Sectional StudyDocument5 pagesComparison of Malnutrition and Malnutrition Screening Tools in Pediatric Oncology Patients A Cross-Sectional StudySebastian MarinNo ratings yet
- Office-Based Motivational Interviewing To Prevent Childhood ObesityDocument7 pagesOffice-Based Motivational Interviewing To Prevent Childhood ObesitynicloverNo ratings yet
- Classification and Management of Feeding Difficulties in Children HO11-004 - E - With - WMDocument2 pagesClassification and Management of Feeding Difficulties in Children HO11-004 - E - With - WMCarlos GonzalezNo ratings yet
- Childhood Eating Disorders British National Surveillance StudyDocument7 pagesChildhood Eating Disorders British National Surveillance StudygharrisanNo ratings yet
- Weight Management Across Preconception, Pregnancy, and Postpartum - A Systematic Review and Quality Appraisal of International Clinical Practice Guidelines.Document23 pagesWeight Management Across Preconception, Pregnancy, and Postpartum - A Systematic Review and Quality Appraisal of International Clinical Practice Guidelines.Carlos ParraNo ratings yet
- J Jneb 2014 06 002Document6 pagesJ Jneb 2014 06 002Zhewen TangNo ratings yet
- AlimentaciónDocument23 pagesAlimentaciónMaro LisNo ratings yet
- Guidelines For The Management of Pregnant Women With Obesity: A Systematic ReviewDocument14 pagesGuidelines For The Management of Pregnant Women With Obesity: A Systematic ReviewMichael ThomasNo ratings yet
- Practiceguidelines: Received: 4 May 2017 Accepted: 22 May 2017 DOI: 10.1002/hed.24866Document7 pagesPracticeguidelines: Received: 4 May 2017 Accepted: 22 May 2017 DOI: 10.1002/hed.24866MdacNo ratings yet
- Intensive & Critical Care Nursing: Research ArticleDocument6 pagesIntensive & Critical Care Nursing: Research ArticleJaemin cuteNo ratings yet
- Age of Introduction of Complementary Feeding and OverweightDocument9 pagesAge of Introduction of Complementary Feeding and OverweightdavidNo ratings yet
- GROUP 6 TDH DR Case Presentation 1Document92 pagesGROUP 6 TDH DR Case Presentation 1Britz Ronquillo MintaNo ratings yet
- AAP Obesity Policy StatementDocument13 pagesAAP Obesity Policy StatementSonia HaNo ratings yet
- Aspen VihDocument19 pagesAspen VihEnzo Ubaque AhumadaNo ratings yet
- Early Childhood Obesity A Survey of Knowledge andDocument8 pagesEarly Childhood Obesity A Survey of Knowledge andshe.hoxhaNo ratings yet
- Life 11 00532Document15 pagesLife 11 00532grpadillaNo ratings yet
- Nutrition Screening AssesmentDocument11 pagesNutrition Screening AssesmentIrving EuanNo ratings yet
- Treatment of Pediatric ObesityDocument6 pagesTreatment of Pediatric Obesitymaxime wotolNo ratings yet
- A Randomized, Controlled Trial of Liraglutide For Adolescents With ObesityDocument12 pagesA Randomized, Controlled Trial of Liraglutide For Adolescents With ObesityWarun KumarNo ratings yet
- Nutrisi Pada Obesitas RemajaDocument15 pagesNutrisi Pada Obesitas RemajaDyah Annisa AnggrainiNo ratings yet
- E20151662 FullDocument11 pagesE20151662 FullMichael OlaleyeNo ratings yet
- CP Cholecystitis With Cholethiasis, Mild Dehydration CAPDocument181 pagesCP Cholecystitis With Cholethiasis, Mild Dehydration CAPArianna Jasmine MabungaNo ratings yet
- 06 Original 02Document7 pages06 Original 02normanahmad92No ratings yet
- Knowledge and Attitudes Towards Baby-Led-Weaning by Health Professionals and Parents A Cross-Sectional Study.Document7 pagesKnowledge and Attitudes Towards Baby-Led-Weaning by Health Professionals and Parents A Cross-Sectional Study.myjesa07No ratings yet
- Nutritional Assessment of Children With CHD CompareDocument9 pagesNutritional Assessment of Children With CHD CompareIntan Robi'ahNo ratings yet
- Breastfeeding Community Based Intervention EvalautionDocument8 pagesBreastfeeding Community Based Intervention EvalautionNERMEEN MOHAMEDALI HASSANNo ratings yet
- Barangay Putik (Report)Document26 pagesBarangay Putik (Report)Shareen AbdusalamNo ratings yet
- Equity in Healthcare: Journal of the Student National Medical Association (JSNMA), #22.1From EverandEquity in Healthcare: Journal of the Student National Medical Association (JSNMA), #22.1No ratings yet
- Analysis of SIRT1 Genetic Variants in Young Mexican Individuals. Relationships Wit Overweight and ObesityDocument12 pagesAnalysis of SIRT1 Genetic Variants in Young Mexican Individuals. Relationships Wit Overweight and Obesityluis sanchezNo ratings yet
- The High Prevalence of Overweight and Obesity in Mexican ChildrenDocument9 pagesThe High Prevalence of Overweight and Obesity in Mexican Childrenluis sanchezNo ratings yet
- StrokeDocument17 pagesStrokeluis sanchezNo ratings yet
- Carbapenem-Resistant Acinetobacter Baumannii in Latin AmericaDocument21 pagesCarbapenem-Resistant Acinetobacter Baumannii in Latin Americaluis sanchezNo ratings yet
- Global Incidence, Prevalence, Years Lived With Disability YLDs, Disability-Adjusted Life-YearsDocument29 pagesGlobal Incidence, Prevalence, Years Lived With Disability YLDs, Disability-Adjusted Life-Yearsluis sanchezNo ratings yet
- Association Between Children's Caregivers Time Preferences and Childhood Overweight and Obesity in MexicoDocument20 pagesAssociation Between Children's Caregivers Time Preferences and Childhood Overweight and Obesity in Mexicoluis sanchezNo ratings yet
- Worldwide Trends in Underweight and Obesity From 1990 To 2022Document24 pagesWorldwide Trends in Underweight and Obesity From 1990 To 2022luis sanchezNo ratings yet
- Global, Regional, and National Age-Specific Progress Towards The 2020 MilestonesDocument28 pagesGlobal, Regional, and National Age-Specific Progress Towards The 2020 Milestonesluis sanchezNo ratings yet
- 2023 Focused Update ESC Guidelines For The DX and TX of A&CHFDocument13 pages2023 Focused Update ESC Guidelines For The DX and TX of A&CHFluis sanchezNo ratings yet
- Clinical and Treatment Profiles of Arterial Hypertension in Mexico During The COVID-19 PandemicDocument29 pagesClinical and Treatment Profiles of Arterial Hypertension in Mexico During The COVID-19 Pandemicluis sanchezNo ratings yet
- Here's What To Know About Cardiovascular-Kidney-Metabolic Syndrome, Newly Defined by The AHADocument2 pagesHere's What To Know About Cardiovascular-Kidney-Metabolic Syndrome, Newly Defined by The AHAluis sanchezNo ratings yet
- Chagas DiseaseDocument16 pagesChagas Diseaseluis sanchezNo ratings yet
- The Full Value of Immunisation Against Respiratory Syncytial Virus For Infants Younger Tha 1 YearDocument10 pagesThe Full Value of Immunisation Against Respiratory Syncytial Virus For Infants Younger Tha 1 Yearluis sanchezNo ratings yet
- Associations of Socioeconomic Status and Healthy Lifestyle With Incident Early-Onset and Late-Onset DementiaDocument10 pagesAssociations of Socioeconomic Status and Healthy Lifestyle With Incident Early-Onset and Late-Onset Dementialuis sanchezNo ratings yet
- Obesity - 2022 - Santini - Marked Weight Loss On Liraglutide 3 0 MG Real Life Experience of A Swiss Cohort With ObesityDocument9 pagesObesity - 2022 - Santini - Marked Weight Loss On Liraglutide 3 0 MG Real Life Experience of A Swiss Cohort With Obesityluis sanchezNo ratings yet
- The Cardiac Wound Healing Response To Myocardial InfarctionDocument19 pagesThe Cardiac Wound Healing Response To Myocardial Infarctionluis sanchezNo ratings yet
- Two-Year Follow-Up of The COVID-19 Pandemic in MexicoDocument14 pagesTwo-Year Follow-Up of The COVID-19 Pandemic in Mexicoluis sanchezNo ratings yet
- Efficacy of Liraglutide in Obesity in Children and Adolescents. Systematic Review and Meta-Analysis of Randomized Controlled Trials. 2023Document10 pagesEfficacy of Liraglutide in Obesity in Children and Adolescents. Systematic Review and Meta-Analysis of Randomized Controlled Trials. 2023luis sanchezNo ratings yet
- Case Study Bronchial Asthma-1Document13 pagesCase Study Bronchial Asthma-1Krishna Krishii AolNo ratings yet
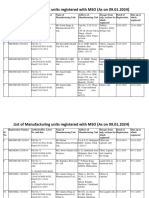
- MSO Latest - Manufacturing - Unit - 12Document46 pagesMSO Latest - Manufacturing - Unit - 12sunshine7883No ratings yet
- HOSPITRAUMA Medtronic CrescentTitanioDocument4 pagesHOSPITRAUMA Medtronic CrescentTitanioliuyonglogNo ratings yet
- MCQ Dental.Document5 pagesMCQ Dental.anuj sharmaNo ratings yet
- 4008 S Haemodialysis Device Instructions For UseDocument354 pages4008 S Haemodialysis Device Instructions For UseHau NghiemdinhNo ratings yet
- Farmington High School Covid19 ClosureDocument1 pageFarmington High School Covid19 ClosureAlyssa RobertsNo ratings yet
- Prevalence of Statin Intolerance: A Meta-AnalysisDocument16 pagesPrevalence of Statin Intolerance: A Meta-Analysisalejandro montesNo ratings yet
- Health LawDocument9 pagesHealth LawayishaNo ratings yet
- Format RKO Dan RKBMHP 2024.xlsx KEMUSUDocument40 pagesFormat RKO Dan RKBMHP 2024.xlsx KEMUSUWatik Nurul FaizahNo ratings yet
- Table For Cestodes and TrematodesDocument5 pagesTable For Cestodes and TrematodesMafie Barreiro100% (4)
- A Self-Fulfilling Prophecy: Systemic Collapse and Pandemic Simulation - The Philosophical SalonDocument14 pagesA Self-Fulfilling Prophecy: Systemic Collapse and Pandemic Simulation - The Philosophical Salonssp consultNo ratings yet
- Jurnal Teknik MenyusuiDocument9 pagesJurnal Teknik Menyusuifitriyani sekar sariNo ratings yet
- g40 - Đề Tham Khảo + Đáp Án - Oanh LeDocument4 pagesg40 - Đề Tham Khảo + Đáp Án - Oanh LetramNo ratings yet
- TWINKLERSDocument13 pagesTWINKLERSshien.intilaNo ratings yet
- CA 1 2022 - Week 10 (Module - Periop) (SINLAG)Document36 pagesCA 1 2022 - Week 10 (Module - Periop) (SINLAG)xtnreyesNo ratings yet
- MSDS Castrol Alphasyn HTX 1000 PDFDocument9 pagesMSDS Castrol Alphasyn HTX 1000 PDFzaidan hadiNo ratings yet
- Patient History-BALLON, KARLO C.Document5 pagesPatient History-BALLON, KARLO C.Melinda Cariño BallonNo ratings yet
- CARTER EP 100 - 084134 - APMO - English - 20230118Document12 pagesCARTER EP 100 - 084134 - APMO - English - 20230118JohnCarterNo ratings yet
- Guidelines For The Safety Assessment A Cosmetic ProductDocument25 pagesGuidelines For The Safety Assessment A Cosmetic ProductJoséNo ratings yet
- Haynes ResumeDocument1 pageHaynes Resumeapi-443388627No ratings yet
- Referat EndometriosisDocument18 pagesReferat EndometriosisAuliaNo ratings yet
- Payslip Payslip Employee Name: Employee Name: Deparment DeparmentDocument22 pagesPayslip Payslip Employee Name: Employee Name: Deparment DeparmentSharlin OrolaNo ratings yet
- A Case of Pica Treated With HomoeopathyDocument20 pagesA Case of Pica Treated With HomoeopathySandip VaghelaNo ratings yet
- (Book Snapshots) Chapter 7 - Birth, Introduction, Summary, Difficult Words and Q & ADocument10 pages(Book Snapshots) Chapter 7 - Birth, Introduction, Summary, Difficult Words and Q & AAMAN KUMARNo ratings yet
- Jurnal Internasional MicrobiologiDocument13 pagesJurnal Internasional MicrobiologiBrillian AlfiNo ratings yet
- Gaa 2024 - DohDocument31 pagesGaa 2024 - DohCris Ann BusilanNo ratings yet
- Chris Enss - Wicked Women - Notorious, Mischievous, and Wayward Ladies From The Old West (2015, TwoDot)Document225 pagesChris Enss - Wicked Women - Notorious, Mischievous, and Wayward Ladies From The Old West (2015, TwoDot)Ad MinaNo ratings yet
- Lesson 2 Importance of Quantitative Research Across Different FieldsDocument20 pagesLesson 2 Importance of Quantitative Research Across Different Fieldsjestoni manipolNo ratings yet
- Anatomy and PhysiologyDocument4 pagesAnatomy and PhysiologyCris Joe Rollorata DumagalNo ratings yet