Download as pdf or txt
You might also like
- NCLFNP - Mr. Robert McClelland CaseDocument4 pagesNCLFNP - Mr. Robert McClelland CaseAiresh Lamao50% (2)
- Dimensions of Culture: Cross-Cultural Communications for Healthcare ProfessionalsFrom EverandDimensions of Culture: Cross-Cultural Communications for Healthcare ProfessionalsRating: 5 out of 5 stars5/5 (1)
- Physical Examination and Health Assessment 8th EditionDocument20 pagesPhysical Examination and Health Assessment 8th EditionDerek Scott Tripp100% (1)
- Charlie and LolaDocument22 pagesCharlie and LolaPeterHanley100% (1)
- Cultural and Global Issues Affecting CommunicationDocument40 pagesCultural and Global Issues Affecting CommunicationYanie Kyle MungcalNo ratings yet
- First Aid PsychiatryDocument156 pagesFirst Aid PsychiatryMae Matira AbeladorNo ratings yet
- Palliative Dr. WinemakerDocument32 pagesPalliative Dr. WinemakerEzhil Vendhan PalanisamyNo ratings yet
- SPIKES ProtocolDocument4 pagesSPIKES ProtocolKassem Gharaibeh100% (1)
- Chapter 15 - Health and Physical Assessment of The Adult ClientDocument65 pagesChapter 15 - Health and Physical Assessment of The Adult ClientKristian Jane de Jesus100% (1)
- Palliative Care BrochureDocument16 pagesPalliative Care BrochureHashim Ahmad100% (1)
- Approaches For Cross Cultural RelationshipsDocument3 pagesApproaches For Cross Cultural RelationshipsMădălina OanceaNo ratings yet
- Understanding Transcultural NursingDocument7 pagesUnderstanding Transcultural NursingVALENZUELA DELIESA E.100% (1)
- Ed, Pa, SDDocument11 pagesEd, Pa, SDgj21since2003No ratings yet
- Trans CulturalDocument6 pagesTrans CulturalAlyssa Santos JavierNo ratings yet
- Chinese Culture ClueDocument2 pagesChinese Culture ClueSr. RZNo ratings yet
- Hms CCC Primer2Document4 pagesHms CCC Primer2KNo ratings yet
- Cultural Sensitivit Y: A Guidebook For Physicians & Healthcare ProfessionalsDocument30 pagesCultural Sensitivit Y: A Guidebook For Physicians & Healthcare ProfessionalsneuronurseNo ratings yet
- Transcultural Nursing in West Florida: U.S. Bureau of Labor StatisticsDocument6 pagesTranscultural Nursing in West Florida: U.S. Bureau of Labor StatisticsChainna Justine CubaoNo ratings yet
- Doctor-Patient Relationship - Cultural Aspects and Other Issues - Adel Adly RaghebDocument10 pagesDoctor-Patient Relationship - Cultural Aspects and Other Issues - Adel Adly RaghebAdel Adly100% (1)
- The Tiniest Book on Diabetes: A Pocket-Sized Primer on Life with Diabetes.From EverandThe Tiniest Book on Diabetes: A Pocket-Sized Primer on Life with Diabetes.No ratings yet
- Rosa Alers Talavera - Spirituality and MedicineDocument4 pagesRosa Alers Talavera - Spirituality and MedicineRosa AlersNo ratings yet
- Difficult Patient and Dealing With Difficult PatientDocument22 pagesDifficult Patient and Dealing With Difficult Patientmhmtrgnn67No ratings yet
- Patient Communication PDFDocument16 pagesPatient Communication PDFraynanthaNo ratings yet
- COA Finals ReviewerDocument216 pagesCOA Finals ReviewerprincessdyrianeNo ratings yet
- Cult Comp CareDocument15 pagesCult Comp CareKharis Mochammad NurNo ratings yet
- 02章(30 89)物理治疗转诊筛查Document60 pages02章(30 89)物理治疗转诊筛查zhangpengNo ratings yet
- Issues of Maternal and Child Health NursingDocument31 pagesIssues of Maternal and Child Health NursingAnonymous XK9fWOhxNo ratings yet
- Communication Skills in Pharmacy Practice Communication Skills in Pharmacy PracticeDocument20 pagesCommunication Skills in Pharmacy Practice Communication Skills in Pharmacy PracticeyousernameNo ratings yet
- Therapists Guide To Brief Cbtmanual-40-79Document40 pagesTherapists Guide To Brief Cbtmanual-40-79Kranthi ManthriNo ratings yet
- Healthy Dimension: A nurse's mind/body weight loss solutionFrom EverandHealthy Dimension: A nurse's mind/body weight loss solutionNo ratings yet
- 2020 CULTURAL INFLUENCES ACTIVITY TambogonDocument2 pages2020 CULTURAL INFLUENCES ACTIVITY TambogonLancerDimlaNo ratings yet
- Reading B2 Bedside Manner: Rapport Psychiatry Family Medicine Pathology RadiologyDocument3 pagesReading B2 Bedside Manner: Rapport Psychiatry Family Medicine Pathology RadiologyIoana BreazuNo ratings yet
- Breaking The Bad NewsDocument20 pagesBreaking The Bad NewsHandoyoNo ratings yet
- Communication Skills For Health Care WorkersDocument25 pagesCommunication Skills For Health Care WorkersnketjimotswalediNo ratings yet
- ElectiveDocument12 pagesElectiveMae Anne MahinayNo ratings yet
- Issues of Maternal and Child Health NursingDocument12 pagesIssues of Maternal and Child Health Nursingcitidotnet87% (31)
- ElectiveDocument35 pagesElectivedeeNo ratings yet
- Answer: Common ProblemsDocument12 pagesAnswer: Common ProblemsKhushnoodNo ratings yet
- Cultural Competence: January 25 2016Document3 pagesCultural Competence: January 25 2016api-301357653No ratings yet
- Care of Older Adult SasDocument29 pagesCare of Older Adult SasMaria Ogabang67% (3)
- 1.introduction To Behavioral SciencesDocument18 pages1.introduction To Behavioral SciencesFaisal Mehboob100% (1)
- Mood Board Essay 24'Document8 pagesMood Board Essay 24'emiliaNo ratings yet
- Dialysis - Teaching PlanDocument4 pagesDialysis - Teaching PlanantiolamNo ratings yet
- Geria - CT 7Document2 pagesGeria - CT 7Leighanne Clyve FerrerNo ratings yet
- Suggested Answers To Critical Thinking ExercisesDocument3 pagesSuggested Answers To Critical Thinking Exercisesracquela_3No ratings yet
- Ethical Issues in Palliative Care: 13 APHC, Surabaya-IndonesiaDocument52 pagesEthical Issues in Palliative Care: 13 APHC, Surabaya-IndonesiaBayu PermanaNo ratings yet
- B. P. Koirala Institute of Health Sciences College of Nursing Dharan, Sunsari, NepalDocument5 pagesB. P. Koirala Institute of Health Sciences College of Nursing Dharan, Sunsari, NepalBhagwati PandeyNo ratings yet
- YoungadultfactsDocument4 pagesYoungadultfactsJaved AnwarNo ratings yet
- PurnelLs Model of Cultural CompetenceDocument32 pagesPurnelLs Model of Cultural CompetenceBobby BwoyNo ratings yet
- 5 Steps: Medical Care Decision Making For Families and Guardians. July 2013Document2 pages5 Steps: Medical Care Decision Making For Families and Guardians. July 2013Dr Jerome MellorNo ratings yet
- Cultural Competence Importance in HealthcareDocument20 pagesCultural Competence Importance in Healthcaresaharconsulting100% (6)
- Breaking Bad NewsDocument4 pagesBreaking Bad NewsHussam KabakbjiNo ratings yet
- Case HistoryDocument22 pagesCase HistoryDeeksha RawatNo ratings yet
- Week 6 Review Challenge-SMEDocument4 pagesWeek 6 Review Challenge-SMEPylorikNo ratings yet
- Lec3 CA Communication SkillsDocument25 pagesLec3 CA Communication Skillsoha37229No ratings yet
- Talking With Your Older PatientDocument74 pagesTalking With Your Older PatientRanisa AmriNo ratings yet
- How Is Advance Care Planning Different From Advance Directives?Document109 pagesHow Is Advance Care Planning Different From Advance Directives?BGNo ratings yet
- BioethicsDocument110 pagesBioethicsvincent_tang_30No ratings yet
- Filipino Cultural CharacteristicsDocument21 pagesFilipino Cultural CharacteristicsArianne Jans MunarNo ratings yet
- How Is Low Health Literacy IdentifiedDocument2 pagesHow Is Low Health Literacy IdentifiedlefanNo ratings yet
- WEEK16CulturalCharacteristic PDFDocument21 pagesWEEK16CulturalCharacteristic PDFKim ChiNo ratings yet
- Spectrum TRD3 Tests Unit-8 1-OptDocument4 pagesSpectrum TRD3 Tests Unit-8 1-OptUrsula Anita Oyola AncajimaNo ratings yet
- Comparatives ReflectionDocument4 pagesComparatives Reflectionapi-490600514No ratings yet
- امتحانات الدمج انجليزى بالإجابات (word) للمرحلة الإبتدائية والإعدادية الترم الأول 2023 اهداء توجيه حلوان موقع دروس تعليمية اونم لاينDocument17 pagesامتحانات الدمج انجليزى بالإجابات (word) للمرحلة الإبتدائية والإعدادية الترم الأول 2023 اهداء توجيه حلوان موقع دروس تعليمية اونم لاينHassan AtefNo ratings yet
- Review of Verb Tenses 2º BachilleratoDocument5 pagesReview of Verb Tenses 2º BachilleratoLucía Martínez VivesNo ratings yet
- Turkish Grammar 1Document15 pagesTurkish Grammar 1BPN TanjungbalaiNo ratings yet
- 4 Schools of Singing. (Italian, German, French, and British)Document4 pages4 Schools of Singing. (Italian, German, French, and British)Rosette Mallari ValenciaNo ratings yet
- 4 Models 4upDocument4 pages4 Models 4upCHANDRA BHUSHANNo ratings yet
- Linguistic Reorganization ArticleDocument23 pagesLinguistic Reorganization ArticleRemin KabakNo ratings yet
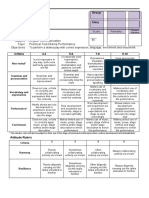
- Subject: English Communication Topic: Practical Test Drama Performance ObjectivesDocument1 pageSubject: English Communication Topic: Practical Test Drama Performance Objectivesanissa paneNo ratings yet
- Transkip NilaiDocument1 pageTranskip NilaiJihan Meta Ardhana100% (1)
- Mid Test Paper (19-04-2021)Document2 pagesMid Test Paper (19-04-2021)Darma ManurungNo ratings yet
- Teaching Vocabulary To Primary and Secondary SchoolDocument2 pagesTeaching Vocabulary To Primary and Secondary SchoolClara CurcaNo ratings yet
- Regular and Irregular VerbsDocument5 pagesRegular and Irregular VerbsDavid ChicaNo ratings yet
- Application Kit: Manitoba Provincial Nominee Program For BusinessDocument51 pagesApplication Kit: Manitoba Provincial Nominee Program For BusinessMichael JohnsNo ratings yet
- Turkish Language Guide ScriptDocument6 pagesTurkish Language Guide ScripthishamsNo ratings yet
- The Teacher-Student Communication Pattern: A Need To Follow?Document7 pagesThe Teacher-Student Communication Pattern: A Need To Follow?Alexandra RenteaNo ratings yet
- Gic2 U2Document30 pagesGic2 U2Мазун Дарина ОлександрівнаNo ratings yet
- Irregular VerbsDocument2 pagesIrregular VerbsmnavherNo ratings yet
- Test Answer Key: UnitsDocument1 pageTest Answer Key: UnitsJUAN DAVID ANDRES CAÑON MARTINEZ50% (2)
- Who, Which, Whom, What, Whose, ThatDocument4 pagesWho, Which, Whom, What, Whose, ThatYFXIINo ratings yet
- Quarter 1 Week 1 English 4Document52 pagesQuarter 1 Week 1 English 4San Vicente ESNo ratings yet
- Sekolah Kebangsaan Pekan Keningau Rancangan Pengajaran HarianDocument2 pagesSekolah Kebangsaan Pekan Keningau Rancangan Pengajaran HarianmazlanpostNo ratings yet
- English: Quarter 1-Module 1Document42 pagesEnglish: Quarter 1-Module 1Princis CianoNo ratings yet
- Creating An ArcGIS Engine Application With C-Sharp and OpenGLDocument11 pagesCreating An ArcGIS Engine Application With C-Sharp and OpenGLNut MaNo ratings yet
- - نموذج استرشادي محادثة واستماع الفرقة الرابعة تعليم أساسي-د. وجدان خليفةDocument4 pages- نموذج استرشادي محادثة واستماع الفرقة الرابعة تعليم أساسي-د. وجدان خليفةAhmed AmerNo ratings yet
- Sopa de LetrasDocument2 pagesSopa de LetrasNelly VincesNo ratings yet
- Fonetica y Fonologia 2Document17 pagesFonetica y Fonologia 2Tammy ParraNo ratings yet
- Y8 Essay StructureDocument1 pageY8 Essay Structureapi-383471557No ratings yet