Download as pdf or txt
You might also like
- Wicked Cheat Days: With Nick DompierreDocument14 pagesWicked Cheat Days: With Nick DompierreMinhao ZhouNo ratings yet
- Kakoullis 2019Document20 pagesKakoullis 2019Andi SusiloNo ratings yet
- New Therapeutic Developments against Shiga Toxin-Producing Escherichia coliDocument14 pagesNew Therapeutic Developments against Shiga Toxin-Producing Escherichia coliMiriam LeiNo ratings yet
- Fischer Sigel Et Al Microbial Pathogenesis Dic-2023Document11 pagesFischer Sigel Et Al Microbial Pathogenesis Dic-2023Karina Fischer SigelNo ratings yet
- Nejmra 2108739Document13 pagesNejmra 2108739Leo TorresNo ratings yet
- Development of Recombinant Lactococcus Lactis DispDocument21 pagesDevelopment of Recombinant Lactococcus Lactis DispGregorius HocevarNo ratings yet
- ART 662 Jenny Granados PDFDocument16 pagesART 662 Jenny Granados PDFdarcy florezNo ratings yet
- Fcimb 02 00090Document7 pagesFcimb 02 00090bonniNo ratings yet
- Cytokine Storm and Leukocyte Changes in Mild Versus SevereDocument25 pagesCytokine Storm and Leukocyte Changes in Mild Versus SevereRaffaharianggaraNo ratings yet
- Medical Microbiology & DiagnosisDocument4 pagesMedical Microbiology & DiagnosisdianaNo ratings yet
- Kuliah 2 Bahan Biologi (Mikroba) Penyebab Keracunan PanganDocument21 pagesKuliah 2 Bahan Biologi (Mikroba) Penyebab Keracunan PanganAchmad HilmyNo ratings yet
- Detection of Shiga Toxin-Producing Escherichia Coli in Ground Beef Using The GeneDisc Real-Time PCR SystemDocument6 pagesDetection of Shiga Toxin-Producing Escherichia Coli in Ground Beef Using The GeneDisc Real-Time PCR SystemACOPIO GUAMALNo ratings yet
- Nattokinase and Spike Protein DetoxDocument9 pagesNattokinase and Spike Protein DetoxBernardoSaviñonPadillaNo ratings yet
- Apoptosis STXDocument7 pagesApoptosis STXKarina Fischer SigelNo ratings yet
- COVID 19 DrugsDocument9 pagesCOVID 19 DrugsTausif AlamNo ratings yet
- Shigella Pathogenesis: Molecular and Computational Insights: ReviewDocument23 pagesShigella Pathogenesis: Molecular and Computational Insights: ReviewRifqi Fathul ArroisiNo ratings yet
- Molecules 29 00849 v2Document32 pagesMolecules 29 00849 v2yashwanth665544No ratings yet
- Campylobacter Jejuni Biofilms Up-Regulated in The Absence of The Stringent Response Utilize A Calcofluor White-Reactive PolysaccharideDocument11 pagesCampylobacter Jejuni Biofilms Up-Regulated in The Absence of The Stringent Response Utilize A Calcofluor White-Reactive PolysaccharideMichaelNo ratings yet
- Toxin Gene Expression by Shiga Toxin-Producing Escherichia coli the Role of Antibiotics and the Bacterial SOS ResponseDocument8 pagesToxin Gene Expression by Shiga Toxin-Producing Escherichia coli the Role of Antibiotics and the Bacterial SOS ResponseMiriam LeiNo ratings yet
- Pone 0100542Document14 pagesPone 0100542UisanimgggNo ratings yet
- Ijms 25 01414Document18 pagesIjms 25 01414alphafoldjesus710No ratings yet
- Phylogeny, Prevalence, and Shiga Toxin (STX) Production of Clinical JapanDocument9 pagesPhylogeny, Prevalence, and Shiga Toxin (STX) Production of Clinical Japancbrs.vetmedNo ratings yet
- Escherichia ColiDocument5 pagesEscherichia ColiAldin AhmetovićNo ratings yet
- Journal of Bacteriology-2008-Rasko-6881.full-compressedDocument13 pagesJournal of Bacteriology-2008-Rasko-6881.full-compressedchamarawmas95No ratings yet
- Fig. 1 Fig. 1: Correspondence Pathology (2019), 51 (4), JuneDocument3 pagesFig. 1 Fig. 1: Correspondence Pathology (2019), 51 (4), JuneDiego TulcanNo ratings yet
- Antimicrobial Resistance, Serologic and Molecular Characterization of E Coli Isolated From Calves With Severe or Fatal Enteritis in Bavaria, GermanyDocument16 pagesAntimicrobial Resistance, Serologic and Molecular Characterization of E Coli Isolated From Calves With Severe or Fatal Enteritis in Bavaria, GermanyHtet Lin OoNo ratings yet
- Bartholin's Abscess Caused by Hypermucoviscous Klebsiella PneumoniaeDocument3 pagesBartholin's Abscess Caused by Hypermucoviscous Klebsiella PneumoniaeRohmantuah_Tra_1826No ratings yet
- Jesus Patogenicidad PecesDocument12 pagesJesus Patogenicidad PecesCAMI ARMYNo ratings yet
- Edema Disease of Swine: A Review of The Pathogenesis: January 2019Document9 pagesEdema Disease of Swine: A Review of The Pathogenesis: January 2019Flaviu TabaranNo ratings yet
- Foodsafetyfscj 5 122Document29 pagesFoodsafetyfscj 5 122Medical Laboratory ChannelNo ratings yet
- Exosomes As NanocarriersDocument9 pagesExosomes As NanocarriersmariamaNo ratings yet
- Kvir 15 2301246Document17 pagesKvir 15 2301246Rodrigo AlvesNo ratings yet
- 09 J Immunol 2010 Silverman 5011 22 LeishmaniaDocument13 pages09 J Immunol 2010 Silverman 5011 22 LeishmanialilianapradaNo ratings yet
- Articulo 6 Ip-10okDocument11 pagesArticulo 6 Ip-10okoscarbio2009No ratings yet
- Streptococcus Pyogenes: Werner ReichardtDocument12 pagesStreptococcus Pyogenes: Werner ReichardtLissette Johana Salamanca MesaNo ratings yet
- Toxic Shock SyndromeDocument13 pagesToxic Shock SyndromeSrinivas PingaliNo ratings yet
- Molecules 28 06811Document35 pagesMolecules 28 06811Nejc KovačNo ratings yet
- 1 s2.0 S0300483X20301670 MainDocument12 pages1 s2.0 S0300483X20301670 MainAhmad SolihinNo ratings yet
- Jiad 230Document10 pagesJiad 230frehanyaqNo ratings yet
- Toxins: Different Types of Cell Death Induced by EnterotoxinsDocument19 pagesToxins: Different Types of Cell Death Induced by Enterotoxinsكريم بسيونيNo ratings yet
- 06 Toll StreptoDocument10 pages06 Toll StreptoFernanda Camargo NunesNo ratings yet
- Fangruida (Smith) Law-The Most Important Scientific Discoveries and Inventions (Boulder)Document7 pagesFangruida (Smith) Law-The Most Important Scientific Discoveries and Inventions (Boulder)weld AdonisNo ratings yet
- Quercetin Alleviates Acute Kidney Injury by Inhibiting FerroptosisDocument13 pagesQuercetin Alleviates Acute Kidney Injury by Inhibiting Ferroptosisdiego.battiatoNo ratings yet
- 1 2 BRDocument3 pages1 2 BRrahmani bagherNo ratings yet
- Advanced Science - 2021 - Liu - Cytokines FroDocument29 pagesAdvanced Science - 2021 - Liu - Cytokines FroDuy HoangNo ratings yet
- Animals 11 00642 v2Document24 pagesAnimals 11 00642 v2ThomasNo ratings yet
- Omega 3 Inflamación GripeDocument12 pagesOmega 3 Inflamación GripeCarlos MendozaNo ratings yet
- Pathogens 11 00151 v2Document14 pagesPathogens 11 00151 v2Mayang WulanNo ratings yet
- Cytoquine Storm and SepsisDocument12 pagesCytoquine Storm and SepsisEduardo ChanonaNo ratings yet
- Research Article: SOCS1 Mimetic Peptide Suppresses Chronic Intraocular Inflammatory Disease (Uveitis)Document33 pagesResearch Article: SOCS1 Mimetic Peptide Suppresses Chronic Intraocular Inflammatory Disease (Uveitis)Paulus SidhartaNo ratings yet
- Biology 11 01466Document21 pagesBiology 11 01466Robert StryjakNo ratings yet
- Gut Microbiota May Not Be Fully Restored in Recovered COVID-19 Patients After 3-Month RecoveryDocument9 pagesGut Microbiota May Not Be Fully Restored in Recovered COVID-19 Patients After 3-Month RecoveryEdgar VázquezNo ratings yet
- Review Sepsis CCM 2007Document9 pagesReview Sepsis CCM 2007Nicole MariaNo ratings yet
- Chenodeoxycholic Acid-Amikacin Combination Enhances ERradication of StaphyDocument17 pagesChenodeoxycholic Acid-Amikacin Combination Enhances ERradication of StaphyAlex HernandezNo ratings yet
- Seminario 4 )Document17 pagesSeminario 4 )dr.tomasbarrazagNo ratings yet
- 01 Modulation by EnteralDocument5 pages01 Modulation by EnteralJavier VegaNo ratings yet
- Pediatric Pneumonia Death Caused by Community-Acquired Methicillin - Resistant Staphylococcus Aureus, JapanDocument3 pagesPediatric Pneumonia Death Caused by Community-Acquired Methicillin - Resistant Staphylococcus Aureus, JapanM ZumrodinNo ratings yet
- Immunoproteomic Approach To Elucidating The Pathogenesis of Cryptococcosis Caused by Cryptococcus GattiiDocument10 pagesImmunoproteomic Approach To Elucidating The Pathogenesis of Cryptococcosis Caused by Cryptococcus GattiiGabriella FreitasNo ratings yet
- Identification of A Staphylococcal Complement Inhibitor With Broad Host Specificity in Equid Staphylococcus Aureus StrainsDocument10 pagesIdentification of A Staphylococcal Complement Inhibitor With Broad Host Specificity in Equid Staphylococcus Aureus StrainsChlo14No ratings yet
- Binding of The Fap2 Protein of Fusobacterium Nucleatum To Human Inhibitory Receptor TIGIT Protects Tumors From Immune Cell Attack 2015 ImmunityDocument13 pagesBinding of The Fap2 Protein of Fusobacterium Nucleatum To Human Inhibitory Receptor TIGIT Protects Tumors From Immune Cell Attack 2015 ImmunityMatthew MacowanNo ratings yet
- The Biology of Fungi Impacting Human Health: A Tropical Asia-Pacific PerspectiveFrom EverandThe Biology of Fungi Impacting Human Health: A Tropical Asia-Pacific PerspectiveRating: 5 out of 5 stars5/5 (1)
- Multiplex PCR for rapid detection of genes encoding (1,2,8,9,25)Document2 pagesMultiplex PCR for rapid detection of genes encoding (1,2,8,9,25)Miriam LeiNo ratings yet
- Characterization of Clinical Isolates of Enterobacteriaceae from Italy by the BD Phoenix Extended-Spectrum -Lactamase Detection Method (TEM primer)Document6 pagesCharacterization of Clinical Isolates of Enterobacteriaceae from Italy by the BD Phoenix Extended-Spectrum -Lactamase Detection Method (TEM primer)Miriam LeiNo ratings yet
- Dutch patients, retail chicken meat and poultry share the same ESBLDocument8 pagesDutch patients, retail chicken meat and poultry share the same ESBLMiriam LeiNo ratings yet
- Occurrence of CTX-M-3, CTX-M-15, CTX-M-14, and CTX-M-9 Extended-Spectrum -Lactamases in Enterobacteriaceae Clinical Isolates in Korea ctx-1,2,9gDocument4 pagesOccurrence of CTX-M-3, CTX-M-15, CTX-M-14, and CTX-M-9 Extended-Spectrum -Lactamases in Enterobacteriaceae Clinical Isolates in Korea ctx-1,2,9gMiriam LeiNo ratings yet
- Optimization of the Hemolysis Assay 2024Document20 pagesOptimization of the Hemolysis Assay 2024Miriam LeiNo ratings yet
- Antimicrobial Peptides Methods and ProtocolsDocument431 pagesAntimicrobial Peptides Methods and ProtocolsMiriam LeiNo ratings yet
- Antibiotic Susceptibility and Molecular Characterization of Aeromonas Hydrophila From Grass CarpDocument6 pagesAntibiotic Susceptibility and Molecular Characterization of Aeromonas Hydrophila From Grass CarpMiriam LeiNo ratings yet
- Assessment of prevalence and changing epidemiology of extended-spectrum β-lactamase-producing Enterobacteriaceae fecal carriers using a chromogenic mediumDocument4 pagesAssessment of prevalence and changing epidemiology of extended-spectrum β-lactamase-producing Enterobacteriaceae fecal carriers using a chromogenic mediumMiriam LeiNo ratings yet
- Wastewater Surveillance of Pathogens Can Inform Public Health ResponsesDocument4 pagesWastewater Surveillance of Pathogens Can Inform Public Health ResponsesMiriam LeiNo ratings yet
- Antimicrobial Susceptibilities of Aeromonas Spp. Isolated From Environmental SourcesDocument7 pagesAntimicrobial Susceptibilities of Aeromonas Spp. Isolated From Environmental SourcesMiriam LeiNo ratings yet
- Combination Drugs: Innovation in PharmacotherapyDocument6 pagesCombination Drugs: Innovation in PharmacotherapyNational Pharmaceutical CouncilNo ratings yet
- Biotechnology: Principles and Processes - (DPP-01) : Lakshya (Neet)Document5 pagesBiotechnology: Principles and Processes - (DPP-01) : Lakshya (Neet)Ram MeharNo ratings yet
- Case Study PsychiaDocument6 pagesCase Study PsychiaJay Jay GwapoNo ratings yet
- Dr. Sheella-Renal Function TestDocument17 pagesDr. Sheella-Renal Function TestFanny BudimanNo ratings yet
- Land Surface Temp and Disease - PPTDocument28 pagesLand Surface Temp and Disease - PPTGOSPEL FACTORYNo ratings yet
- NHS Guideline For Treatment of Primary Insomnia 2019Document2 pagesNHS Guideline For Treatment of Primary Insomnia 2019Oscar ChauNo ratings yet
- Complete Health Insurance (Health Elite)Document19 pagesComplete Health Insurance (Health Elite)Sumit malikNo ratings yet
- Nishant Respiratory SecondDocument10 pagesNishant Respiratory SecondNishantNo ratings yet
- Pathology Laboratory IRCS Mehsana Taluka BranchDocument14 pagesPathology Laboratory IRCS Mehsana Taluka BranchVedant VyasNo ratings yet
- (Ophtha) Ocular Emergencies-Dr. Rebong (Parbs)Document6 pages(Ophtha) Ocular Emergencies-Dr. Rebong (Parbs)Patricia ManaliliNo ratings yet
- Dr. DolittleDocument45 pagesDr. DolittleTejashree Malpani-JahagirdarNo ratings yet
- Aqua - CELDocument2 pagesAqua - CELfajry_uhNo ratings yet
- English ProverbsDocument25 pagesEnglish ProverbsmukuldeshNo ratings yet
- Enteropathogenic Escherichia Coli - Written Report PDFDocument6 pagesEnteropathogenic Escherichia Coli - Written Report PDFuypaul97No ratings yet
- Disseminated Intravascular CoagulationDocument3 pagesDisseminated Intravascular CoagulationArlan Abragan100% (1)
- GHVDocument146 pagesGHVSantosh BhandariNo ratings yet
- Mas 2Document7 pagesMas 2Nofiya RuswantiNo ratings yet
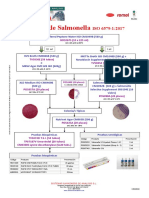
- Salmonella ISO 6579 2017Document1 pageSalmonella ISO 6579 2017Đăng Lưu100% (1)
- Qtern 84413Document19 pagesQtern 84413Manoj KaluvakotaNo ratings yet
- Transes Anaphy DigestionDocument7 pagesTranses Anaphy DigestionPia LouiseNo ratings yet
- Poster SpecCircs Anaphylaxis Treatment Algorithm ENG V20151001 HRES Site PDFDocument1 pagePoster SpecCircs Anaphylaxis Treatment Algorithm ENG V20151001 HRES Site PDFPetrarkina LauraNo ratings yet
- Benedek Theodora - Curs Cardiologie Interventionala FinalDocument102 pagesBenedek Theodora - Curs Cardiologie Interventionala FinalBianca IlieNo ratings yet
- Introduction To PharmacologyDocument50 pagesIntroduction To PharmacologyAbdishakour Hassa.100% (1)
- PostureDocument2 pagesPostureNader MorrisNo ratings yet
- GENERAL PHARMACOLOGY (Metabolism)Document37 pagesGENERAL PHARMACOLOGY (Metabolism)rexef82757No ratings yet
- Female Reproductive SystemDocument42 pagesFemale Reproductive SystemDoki NatsuNo ratings yet
- Changing: Your Partner ForDocument16 pagesChanging: Your Partner ForsunilNo ratings yet
- Epi FinalDocument481 pagesEpi FinalSana Savana Aman R100% (1)
- Nursing Care For Patient Undergoing TAHBSO For Ovarian GrowthDocument4 pagesNursing Care For Patient Undergoing TAHBSO For Ovarian GrowthAyaBasilio100% (2)