Download as docx, pdf, or txt
You might also like
- Skin Assessment FormDocument2 pagesSkin Assessment FormOng KarlNo ratings yet
- Settings, Processes, Methods and Tools in Counseling: Quarter 1 (Module 5)Document10 pagesSettings, Processes, Methods and Tools in Counseling: Quarter 1 (Module 5)Mark Anthony Garcia100% (1)
- Behavior TherapyDocument3 pagesBehavior TherapyScott Carter100% (1)
- Problem-Solving Group Therapy: A Group Leader's Guide for Developing and Implementing Group Treatment PlansFrom EverandProblem-Solving Group Therapy: A Group Leader's Guide for Developing and Implementing Group Treatment PlansRating: 4.5 out of 5 stars4.5/5 (2)
- Occupational TherapyDocument19 pagesOccupational TherapySwarnalata RKNo ratings yet
- Presentation On Therapeutic MilieuDocument48 pagesPresentation On Therapeutic MilieuShailja SharmaNo ratings yet
- A Model of Human Occupation ApproachDocument55 pagesA Model of Human Occupation Approachllloo100% (8)
- Evaluation of A Life Skills Group For Brain Injury Patients On An Acute Neurological Rehabilitation UnitDocument1 pageEvaluation of A Life Skills Group For Brain Injury Patients On An Acute Neurological Rehabilitation UnitJodiMBrownNo ratings yet
- Sowk 155 Unit TwoDocument32 pagesSowk 155 Unit TwoBLESS AKAKPONo ratings yet
- Occupational TherapyDocument6 pagesOccupational TherapyJayita Gayen DuttaNo ratings yet
- CH 9 Occupational Therapy FrameworkDocument2 pagesCH 9 Occupational Therapy Frameworkapi-299934163No ratings yet
- Forensic Psychiatry and Occupational TherapyDocument3 pagesForensic Psychiatry and Occupational TherapyVuyokazi Nosipho MajolaNo ratings yet
- Occupational TherapyDocument7 pagesOccupational TherapyIsha BhusalNo ratings yet
- Case ConceptualizationDocument16 pagesCase ConceptualizationmichaelxandrNo ratings yet
- My Sample LetterDocument16 pagesMy Sample Lettertjvt5sg7dyNo ratings yet
- Theories and Techniques of CounsellingDocument5 pagesTheories and Techniques of CounsellingAKANKSHA SUJIT CHANDODE PSYCHOLOGY-CLINICALNo ratings yet
- 3.nursing Process.Document42 pages3.nursing Process.Gilbert JohnNo ratings yet
- MPCE 13 EM 23-24Document23 pagesMPCE 13 EM 23-24Sandeep SingalNo ratings yet
- Community Health EducationDocument22 pagesCommunity Health EducationIs MaïlNo ratings yet
- مقدمة و متطلباتDocument9 pagesمقدمة و متطلباتseedhassan686No ratings yet
- Psikologi Konseling - BehavioristikDocument26 pagesPsikologi Konseling - BehavioristikDEVIANTY RHAMADHANINo ratings yet
- Cognitive-Behavioral TherapyDocument60 pagesCognitive-Behavioral TherapyVaneeza AliNo ratings yet
- Introduction To Psychological InterventionsDocument26 pagesIntroduction To Psychological InterventionsJay Mark Cabrera100% (1)
- Classical Psychotherapies Unit 3,4,5Document25 pagesClassical Psychotherapies Unit 3,4,5Anchal BoharaNo ratings yet
- Psy 453Document29 pagesPsy 453AdelinaNo ratings yet
- The Effect of Group Coaching On Brain ActivityDocument10 pagesThe Effect of Group Coaching On Brain ActivityNguyễn NhưNo ratings yet
- Role of Occupational Therapy in The Treatment of Mental DisordersDocument34 pagesRole of Occupational Therapy in The Treatment of Mental DisorderssamuelNo ratings yet
- Integrative and Multimodal Therapy by Sneha With WatermarkDocument10 pagesIntegrative and Multimodal Therapy by Sneha With WatermarkSnehakrishnanNo ratings yet
- Care Planning & Reflection PresentationDocument48 pagesCare Planning & Reflection PresentationBatool Al-Shabrakha100% (2)
- Ruchi Integration of ApproachesDocument19 pagesRuchi Integration of Approachesjaahoo00777No ratings yet
- Prioritized Problem ListDocument2 pagesPrioritized Problem ListJoeffric Nourence CayabanNo ratings yet
- Nursing Models and Care Planning CCDocument26 pagesNursing Models and Care Planning CCangelica1971No ratings yet
- 03 Psycheck Clinical TreatmentDocument147 pages03 Psycheck Clinical TreatmentJohnny TorresNo ratings yet
- Behavior TherapyDocument50 pagesBehavior TherapyRoberto VargasNo ratings yet
- BEHAVIOURAL THERAPYDocument7 pagesBEHAVIOURAL THERAPYsodumsuvidhaNo ratings yet
- Nursing Arts LO Module 4Document7 pagesNursing Arts LO Module 4AmberpersonNo ratings yet
- Theoretical ConsiderationsDocument36 pagesTheoretical Considerationsapi-290300066No ratings yet
- 12 Behavioristic Approach IUP Basic InterventionDocument18 pages12 Behavioristic Approach IUP Basic InterventionTSURAYA MUTIARALARASHATINo ratings yet
- (Magistral) Sohlberg (1) - Towards An Integrated Model of Cognitive Rehabilitation With A Focus On Functional OutcomeDocument66 pages(Magistral) Sohlberg (1) - Towards An Integrated Model of Cognitive Rehabilitation With A Focus On Functional OutcomeZAMIRANo ratings yet
- The Application of Assessment and Evaluation Procedure in Using Occupation Centered PracticeDocument55 pagesThe Application of Assessment and Evaluation Procedure in Using Occupation Centered PracticeAswathi100% (2)
- Basic CoachingDocument3 pagesBasic Coachingmiaedmonds554No ratings yet
- UNIT - 5 - Behavioural TherapyDocument42 pagesUNIT - 5 - Behavioural Therapygargchiya97No ratings yet
- Cognitive Behavioral TherapyDocument4 pagesCognitive Behavioral TherapyTyler06GwanOxNo ratings yet
- Behavior TherapyDocument4 pagesBehavior TherapyMarianne DalmacioNo ratings yet
- Counselling Approaches BehavourDocument28 pagesCounselling Approaches Behavourtinotenda mamberaNo ratings yet
- Cognitive Behavioral Approaches To GroupDocument37 pagesCognitive Behavioral Approaches To GroupJessica Rey TanNo ratings yet
- 2 - Roles of Community Health NursingDocument20 pages2 - Roles of Community Health Nursingraghad awwad100% (4)
- TFN - Module 7 Notes For StudentsDocument3 pagesTFN - Module 7 Notes For StudentsEileen Aquino MacapagalNo ratings yet
- Planning ReportDocument14 pagesPlanning ReportReylan GarciaNo ratings yet
- Application of Changew Theory in Nursing PracticeDocument4 pagesApplication of Changew Theory in Nursing PracticeAnjali NaudiyalNo ratings yet
- 1.professional ReasoningDocument23 pages1.professional ReasoningAswathiNo ratings yet
- 23-05-2018 011346916 - Intervention Modalities - Chapter 16Document26 pages23-05-2018 011346916 - Intervention Modalities - Chapter 16Bisan RatuishNo ratings yet
- 1healthcare TeamDocument37 pages1healthcare TeamNur Syahirah Mohamad RosliNo ratings yet
- Occupational TherapyDocument15 pagesOccupational Therapymanu sethi100% (1)
- Quiz 1 - Psychotherapeutic Stages-232744Document5 pagesQuiz 1 - Psychotherapeutic Stages-232744aqsa rehmanNo ratings yet
- Building Better Routines NDIS OT WebinarDocument34 pagesBuilding Better Routines NDIS OT WebinarjadegalNo ratings yet
- Assingment on Milieu TherapyDocument4 pagesAssingment on Milieu TherapySoraisham Kiranbala DeviNo ratings yet
- Peplau TheoryDocument9 pagesPeplau TheoryManish Tripathi100% (1)
- THERAPYYYDocument10 pagesTHERAPYYYERIKA MAE SIROYNo ratings yet
- Advanced Motivational Interviewing for Mental Health Clinicians: Integrating Neuroscience and Trauma-Informed Care with Real-World Case Studies and Practical ExercisesFrom EverandAdvanced Motivational Interviewing for Mental Health Clinicians: Integrating Neuroscience and Trauma-Informed Care with Real-World Case Studies and Practical ExercisesNo ratings yet
- A Concise Guide to Acceptance and Cognitive Therapy: ACT for BeginnersFrom EverandA Concise Guide to Acceptance and Cognitive Therapy: ACT for BeginnersNo ratings yet
- Peritoneal DialysisDocument16 pagesPeritoneal DialysisSoraisham Kiranbala DeviNo ratings yet
- Operation Theater TechniquesDocument34 pagesOperation Theater TechniquesSoraisham Kiranbala DeviNo ratings yet
- Cardio Pulmonary Resuscitation ProcedureDocument15 pagesCardio Pulmonary Resuscitation ProcedureSoraisham Kiranbala DeviNo ratings yet
- Physical ExaminationDocument137 pagesPhysical ExaminationSoraisham Kiranbala DeviNo ratings yet
- Biology TmaDocument7 pagesBiology TmaMISS RASHMINo ratings yet
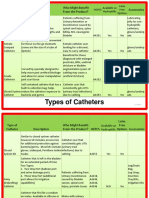
- Types of CathetersDocument2 pagesTypes of CathetersLorie Fadol100% (1)
- Journal of Nutrition College,: Sensitivity C-Reactive Protein (HS-CRP) Pada RemajaDocument6 pagesJournal of Nutrition College,: Sensitivity C-Reactive Protein (HS-CRP) Pada RemajaDevi OktariaNo ratings yet
- Obsgin - Gynecologic OncologyDocument8 pagesObsgin - Gynecologic OncologyARDHANo ratings yet
- Myofunctional TherapyDocument19 pagesMyofunctional Therapy許越隆No ratings yet
- Arthroscopic Shoulder Anterior Stabilisation Rehabilitation Protocol by TENDAYI MUTSOPOTSI MSc. ORTHO-MEDDocument8 pagesArthroscopic Shoulder Anterior Stabilisation Rehabilitation Protocol by TENDAYI MUTSOPOTSI MSc. ORTHO-MEDPhysiotherapy Care SpecialistsNo ratings yet
- RopDocument364 pagesRopIeie MawonNo ratings yet
- Presenter 1: Psychological Causes of Drug AddictionDocument4 pagesPresenter 1: Psychological Causes of Drug AddictionJeremiah AimitonNo ratings yet
- Sympathetic GanglionectomyDocument8 pagesSympathetic GanglionectomyCeaGarsakyNo ratings yet
- Endo PerioDocument41 pagesEndo Periovishrutha purushothamNo ratings yet
- Fractional CO2 Laser Treatment For StretchmarksDocument6 pagesFractional CO2 Laser Treatment For StretchmarksShinagawaPh Main100% (1)
- Amoxgentin - Amoxycillin & Potassium Clavulanate Injection - Export 600mg I.V - InFODocument1 pageAmoxgentin - Amoxycillin & Potassium Clavulanate Injection - Export 600mg I.V - InFOAnonymous BVD7IKfNo ratings yet
- What Is Anemia?: Anemia Blood Cells Hemoglobin Blood Cells Symptoms of Anemia FatigueDocument5 pagesWhat Is Anemia?: Anemia Blood Cells Hemoglobin Blood Cells Symptoms of Anemia FatigueLIPTANo ratings yet
- Extensor Tendon Fingers Norwich Guideline 2018Document2 pagesExtensor Tendon Fingers Norwich Guideline 2018Ariana Iorga100% (1)
- IT 9 - Hematology Malignancy - NDDocument93 pagesIT 9 - Hematology Malignancy - NDDesi MawarniNo ratings yet
- PharmacologyDocument1 pagePharmacologyایم ناولسٹNo ratings yet
- Daftar PustakaDocument4 pagesDaftar PustakaSantalia SeramNo ratings yet
- Drinking Water and Losing WeightDocument3 pagesDrinking Water and Losing WeightMathana SuriaNo ratings yet
- Consent For Circumcision: Minor Problems Are Short-TermDocument4 pagesConsent For Circumcision: Minor Problems Are Short-Termabrnrd56No ratings yet
- Roles of A NurseDocument6 pagesRoles of A NurseHex Jeif EchavezNo ratings yet
- Diabetes Awarenessin KG KapokDocument4 pagesDiabetes Awarenessin KG Kapokempus CatNo ratings yet
- DR Mustika Mahbubi SPJP FIHA-How To Treat Acute Coronary Sydrome (STEMI Patient) in Pre and Post HospitalDocument59 pagesDR Mustika Mahbubi SPJP FIHA-How To Treat Acute Coronary Sydrome (STEMI Patient) in Pre and Post HospitalHiszom AsyhariNo ratings yet
- Group Collaborative Activity TaskonomyDocument2 pagesGroup Collaborative Activity TaskonomyTweeky SaureNo ratings yet
- Breast ScreeningDocument75 pagesBreast ScreeningNikko Herrero CabrestanteNo ratings yet
- Screenshot 2023-05-20 at 8.20.47 AMDocument47 pagesScreenshot 2023-05-20 at 8.20.47 AMSrinidhi DrNo ratings yet
- 4.4 Which Swab Specimen For Which TestDocument2 pages4.4 Which Swab Specimen For Which TestVishaw Dev JoshiNo ratings yet
- Clinical Service ManagementDocument5 pagesClinical Service ManagementdharatriNo ratings yet
- 30 - Toronto Notes 2011 - Common Unit Conversions - Commonly Measured Laboratory Values - Abbreviations - IndexDocument28 pages30 - Toronto Notes 2011 - Common Unit Conversions - Commonly Measured Laboratory Values - Abbreviations - IndexRazrin RazakNo ratings yet
- ORSDocument2 pagesORSdraw with usNo ratings yet