Download as pdf or txt
You might also like
- PM Schedule Interior Fit Out Works For DIB Baniyas Branch Abu Dhabi UAE PDFDocument5 pagesPM Schedule Interior Fit Out Works For DIB Baniyas Branch Abu Dhabi UAE PDFXozan100% (1)
- The 3D Printing Handbook - Technologies, Design and ApplicationsDocument347 pagesThe 3D Printing Handbook - Technologies, Design and ApplicationsJuan Bernardo Gallardo100% (7)
- Surgery OsceDocument69 pagesSurgery OsceRebecca BrandonNo ratings yet
- Apple Iphone XR (White, 64 GB) (Includes Earpods, Power Adapter)Document2 pagesApple Iphone XR (White, 64 GB) (Includes Earpods, Power Adapter)Gaurav Poddar100% (2)
- NG Tube IntubationDocument40 pagesNG Tube IntubationVed BratNo ratings yet
- Nasogastric Tube NGT 1215082454278959 8Document107 pagesNasogastric Tube NGT 1215082454278959 8Raquel M. MendozaNo ratings yet
- احمد كريمDocument12 pagesاحمد كريمMr. abbas fahim hamidNo ratings yet
- Nasogastric Intubation Bladder CatheterizationDocument18 pagesNasogastric Intubation Bladder Catheterizationmolaf17696No ratings yet
- NG Tube Lictures 2023Document22 pagesNG Tube Lictures 2023ALi NursingNo ratings yet
- Ryle's Tube (Nasogastric Tube)Document41 pagesRyle's Tube (Nasogastric Tube)Sandhya BasnetNo ratings yet
- Module 3 Nursing Skills Procedure On GI, Endo-Metab Concept (A)Document18 pagesModule 3 Nursing Skills Procedure On GI, Endo-Metab Concept (A)Nashebah A. BatuganNo ratings yet
- Nasogastric+Tube+Insertion+and+Removal 2Document24 pagesNasogastric+Tube+Insertion+and+Removal 2Anonymous 4OJslWE1No ratings yet
- NG Tube InsertionDocument37 pagesNG Tube InsertionSarah BirechNo ratings yet
- Administering An EnemaDocument13 pagesAdministering An EnemaNai DhavalNo ratings yet
- .archNG - Parenteral NutritionDocument77 pages.archNG - Parenteral NutritionBidhya GuptaNo ratings yet
- NGT:OGTDocument2 pagesNGT:OGTeloiza custodioNo ratings yet
- Nasogastric Tube InsertionDocument10 pagesNasogastric Tube InsertionPoh Thing LawNo ratings yet
- Nasogastric Tube InsertionDocument18 pagesNasogastric Tube InsertionSandya PallapotuNo ratings yet
- Providing Special CareDocument23 pagesProviding Special CareJan LagriaNo ratings yet
- NGT Insertion: Group 2 Guerrero, Gumatay, Lim, Lopez, Mallabo, Miñano, Nario, Olores, Paaño, Pajutan, Paz, PerezDocument19 pagesNGT Insertion: Group 2 Guerrero, Gumatay, Lim, Lopez, Mallabo, Miñano, Nario, Olores, Paaño, Pajutan, Paz, PerezHarlyn MagsinoNo ratings yet
- Nasogastric Tube: - Insertion - FeedingDocument61 pagesNasogastric Tube: - Insertion - FeedingJustine Cagatan75% (4)
- Insertion of A Nasogastric Tube - Examiner RoleplayDocument3 pagesInsertion of A Nasogastric Tube - Examiner Roleplaysanju ghimireNo ratings yet
- Gastric LavageDocument13 pagesGastric Lavagetibinj67No ratings yet
- Assisting in Nasogastric Tube Insertion 1 1Document14 pagesAssisting in Nasogastric Tube Insertion 1 1Princess Faniega SugatonNo ratings yet
- Urinary-Catheterization (1)Document31 pagesUrinary-Catheterization (1)hazel jamisNo ratings yet
- Assisting in Nasogastric Tube InsertionDocument11 pagesAssisting in Nasogastric Tube InsertionJan Federick BantayNo ratings yet
- PARACENTESISDocument15 pagesPARACENTESISSoonh ChannaNo ratings yet
- NG and Foley Cath M2 2009Document54 pagesNG and Foley Cath M2 2009aditi268100% (1)
- Lect 8 SUTUREDocument33 pagesLect 8 SUTUREAbdisamed AllaaleNo ratings yet
- Nasogastric TubeDocument25 pagesNasogastric Tubekayse abtidoonNo ratings yet
- NGT Feeding Discussion InotDocument2 pagesNGT Feeding Discussion InotRhenelyn Delos ReyesNo ratings yet
- Nasogastric Intubation: DR - Efman.E.U.Manawan Mkes.,Spb-KbdDocument32 pagesNasogastric Intubation: DR - Efman.E.U.Manawan Mkes.,Spb-KbdBilly PeterNo ratings yet
- Intro To Specialized Nursing ProceduresDocument156 pagesIntro To Specialized Nursing ProceduresJimmy MainaNo ratings yet
- Foley Catheter PlacementDocument16 pagesFoley Catheter PlacementAlana CaballeroNo ratings yet
- Inserting Nasogastric TubeDocument4 pagesInserting Nasogastric TubeLoveSheryNo ratings yet
- Abdominal Paracentesis PDFDocument12 pagesAbdominal Paracentesis PDFJosephine George JojoNo ratings yet
- Inserting An NG TubeDocument1 pageInserting An NG TubeKay BristolNo ratings yet
- Presentation 1Document21 pagesPresentation 1Rekha PariharNo ratings yet
- Att.C08B1zSInzwQMCKoLLjeNVmv9HIibrSU88sJ0xvvxqEDocument38 pagesAtt.C08B1zSInzwQMCKoLLjeNVmv9HIibrSU88sJ0xvvxqEJaymark BlancoNo ratings yet
- Objectives: at The End of The Discussion The Students Will Be Able ToDocument6 pagesObjectives: at The End of The Discussion The Students Will Be Able ToMichael Angelo SeñaNo ratings yet
- Nasogastric Tube InsertionDocument17 pagesNasogastric Tube InsertionMichael Jude MedallaNo ratings yet
- Nasogastric TubeDocument5 pagesNasogastric TubeangelaNo ratings yet
- Paracentesis: by A.B.Sani KKB Son KTDocument8 pagesParacentesis: by A.B.Sani KKB Son KTabdulNo ratings yet
- Final TracheostomyDocument6 pagesFinal TracheostomychandhomepcNo ratings yet
- NGTDocument36 pagesNGTAstrid Bernadette Ulina PurbaNo ratings yet
- Objectives: Intestinal Tube InsertionDocument28 pagesObjectives: Intestinal Tube Insertion2013SecBNo ratings yet
- Pancreatic PseudocystDocument16 pagesPancreatic PseudocystSpandan KadamNo ratings yet
- GI Diagnostic TestsDocument7 pagesGI Diagnostic TestspatzieNo ratings yet
- Common Neonatal Surgical Conditions: Intensive Care Nursery House Staff ManualDocument6 pagesCommon Neonatal Surgical Conditions: Intensive Care Nursery House Staff ManualSayf QisthiNo ratings yet
- Sigmoidoscopy: Presented by Kriti Adhikari Roll No: 17Document38 pagesSigmoidoscopy: Presented by Kriti Adhikari Roll No: 17sushma shresthaNo ratings yet
- Elderly Care 101-NGT and PEGDocument92 pagesElderly Care 101-NGT and PEGBecky GalanoNo ratings yet
- Nasogastric Tube (Assissting in Indertion, Feeding) .ProcedureDocument4 pagesNasogastric Tube (Assissting in Indertion, Feeding) .ProcedureJeonoh FloridaNo ratings yet
- Nutrition: Procedure GuidelinesDocument33 pagesNutrition: Procedure GuidelinesAhmad SobihNo ratings yet
- Ccu NotesDocument76 pagesCcu NotesAr PeeNo ratings yet
- Nasogastric Intubation: DR - Efman.E.U.Manawan Mkes.,Spb-KbdDocument32 pagesNasogastric Intubation: DR - Efman.E.U.Manawan Mkes.,Spb-KbdNur Ilmi SofiahNo ratings yet
- NGT PresentationDocument23 pagesNGT PresentationniyigokNo ratings yet
- Endoscopy, Barium MealDocument22 pagesEndoscopy, Barium Mealyudhisthir panthiNo ratings yet
- Nasogastric Tube Insertion: Nursing Guidelines and ConsiderationsDocument39 pagesNasogastric Tube Insertion: Nursing Guidelines and ConsiderationsTiger KneeNo ratings yet
- Nasogastric TubeDocument10 pagesNasogastric TubeJihad HassanNo ratings yet
- NGTDocument4 pagesNGTRuthie BangteganNo ratings yet
- Nasogastric Tube InsertionDocument3 pagesNasogastric Tube InsertionLorenza VillarinoNo ratings yet
- InstrumentsDocument56 pagesInstrumentsroshankc0001No ratings yet
- Atlas of Laparoscopic Gastrectomy for Gastric Cancer: High Resolution Image for New Surgical TechniqueFrom EverandAtlas of Laparoscopic Gastrectomy for Gastric Cancer: High Resolution Image for New Surgical TechniqueNo ratings yet
- Turbdstart Two™: WarningDocument1 pageTurbdstart Two™: Warningarness22No ratings yet
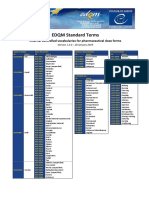
- Standard Terms Internal Vocabularies For Pharmaceutical Dose FormsDocument7 pagesStandard Terms Internal Vocabularies For Pharmaceutical Dose FormsJose De La Cruz De La ONo ratings yet
- Health and Family Life Education 1Document14 pagesHealth and Family Life Education 1JeanMichael Vincent100% (1)
- November 2019 (v3) QP - Paper 4 CIE Chemistry IGCSEDocument16 pagesNovember 2019 (v3) QP - Paper 4 CIE Chemistry IGCSEJeevith Soumya SuhasNo ratings yet
- Basic Accounting Principles ModuleDocument23 pagesBasic Accounting Principles ModulezendeexNo ratings yet
- Chapter 8 - Memory Storage Devices Question AnswersDocument4 pagesChapter 8 - Memory Storage Devices Question AnswersAditya MalhotraNo ratings yet
- Part 1: Application letters (Thư xin việc) : What to include in an application letterDocument9 pagesPart 1: Application letters (Thư xin việc) : What to include in an application letterKen BiNo ratings yet
- B. SC Nursing: Medical Surgical Nursing Unit V - Disorders of The Cardio Vascular SystemDocument31 pagesB. SC Nursing: Medical Surgical Nursing Unit V - Disorders of The Cardio Vascular SystemPoova Ragavan100% (1)
- Pulse OximetryDocument29 pagesPulse OximetryAnton ScheepersNo ratings yet
- Warhammer Skaven Paint GuideDocument2 pagesWarhammer Skaven Paint Guiderandom-userNo ratings yet
- Acts 13 New 2Document8 pagesActs 13 New 2fitsum tesfayeNo ratings yet
- Literary Appreciation SkillsDocument18 pagesLiterary Appreciation SkillsZaineid CaelumNo ratings yet
- Araña BJ 350 Ton 13 3-8Document60 pagesAraña BJ 350 Ton 13 3-8ceciliachableNo ratings yet
- Pengembangan Prosedur Dan Penataan Dinas JagaDocument11 pagesPengembangan Prosedur Dan Penataan Dinas JaganoviNo ratings yet
- Squatting Should Not Be Illegal. in Fact, It Should Be EncouragedDocument2 pagesSquatting Should Not Be Illegal. in Fact, It Should Be EncouragedNguyen Trong Phuc (FUG CT)No ratings yet
- Adjustment LetterDocument14 pagesAdjustment LetterQadr IftikharNo ratings yet
- Princess Maker 2 EndingsDocument11 pagesPrincess Maker 2 EndingspsnapplebeeNo ratings yet
- Definition of DemocracyDocument20 pagesDefinition of DemocracyAnonymous R1SgvNINo ratings yet
- I. Multiple Choice. Read and Analyze Each Question and Encircle The Letter of The Correct Physical EducationDocument3 pagesI. Multiple Choice. Read and Analyze Each Question and Encircle The Letter of The Correct Physical EducationMarck Jhon YalungNo ratings yet
- Neonatal Intubation: Past, Present, and Future: Practice GapsDocument9 pagesNeonatal Intubation: Past, Present, and Future: Practice GapskiloNo ratings yet
- b1 Speaking FashionDocument2 pagesb1 Speaking FashionIsaSánchezNo ratings yet
- Conflict Management, Team Coordination, and Performance Within Multicultural Temporary Projects: Evidence From The Construction IndustryDocument14 pagesConflict Management, Team Coordination, and Performance Within Multicultural Temporary Projects: Evidence From The Construction Industryjaveria khanNo ratings yet
- House of ConcreteDocument9 pagesHouse of ConcreteArkyadeep ChowdhuryNo ratings yet
- A Study in Satin I by TiggerDocument120 pagesA Study in Satin I by TiggerCereal69No ratings yet
- 1.socio Economic Determinants of HealthDocument64 pages1.socio Economic Determinants of HealthdenekeNo ratings yet
- Succession Cause 846 of 2011Document6 pagesSuccession Cause 846 of 2011kbaisa7No ratings yet
- SRS For Hotel Management SystemDocument16 pagesSRS For Hotel Management SystemAdarsh SinghNo ratings yet