Download as pdf or txt
You might also like
- 06a - OHMS MyWay Info PresentationDocument49 pages06a - OHMS MyWay Info Presentationmanami11No ratings yet
- Evaluating Impact: Turning Promises Into Evidence: Community Based Health Insurance SchemeDocument10 pagesEvaluating Impact: Turning Promises Into Evidence: Community Based Health Insurance Schemeseid mohammedNo ratings yet
- Bermuda Health Council: Corporate PlanDocument14 pagesBermuda Health Council: Corporate PlanBernewsAdminNo ratings yet
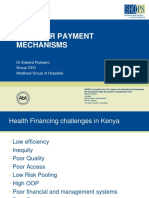
- Provider Payment MechanismsDocument20 pagesProvider Payment MechanismsCristhian LarrahondoNo ratings yet
- Healthcare WebinarDocument24 pagesHealthcare WebinarsureshtaureanNo ratings yet
- ZiffyHealth - Corporate Offerings - 19122019Document28 pagesZiffyHealth - Corporate Offerings - 19122019Pankaj ChoudhariNo ratings yet
- Evolving Health Care ModelDocument47 pagesEvolving Health Care Modelibson045001256No ratings yet
- Meningkatkan Mutu Pelayanan Dan Efisiensi Rumah Sakit - Jogja 8 Nov17Document24 pagesMeningkatkan Mutu Pelayanan Dan Efisiensi Rumah Sakit - Jogja 8 Nov17Aprilia ErmaNo ratings yet
- Artifiq Healthcare PPT - ModifiedDocument39 pagesArtifiq Healthcare PPT - Modifiedneh SinghNo ratings yet
- Stanley Lalta - Health FinancingDocument14 pagesStanley Lalta - Health FinancingPysadee PysadeeNo ratings yet
- Profil Perusahaan Cynergy Care IndonesiaDocument18 pagesProfil Perusahaan Cynergy Care IndonesiaRomeo Jaka RNo ratings yet
- Local Govt Infographic v9PGSDocument4 pagesLocal Govt Infographic v9PGSEd PraetorianNo ratings yet
- Shanz - Commed Le 2Document3 pagesShanz - Commed Le 2Petrina XuNo ratings yet
- Behavior Economics ClinicalDocument18 pagesBehavior Economics ClinicalEPNo ratings yet
- Quick Facts BrochureDocument6 pagesQuick Facts Brochurenifej15595No ratings yet
- Service Sector Management Health Care SectorDocument85 pagesService Sector Management Health Care SectorshuweNo ratings yet
- The Good PracticeDocument39 pagesThe Good PracticeD.WorkuNo ratings yet
- Competitive StragetyDocument23 pagesCompetitive StragetyBashudev BhandariNo ratings yet
- Procuement and Supply Management PDFDocument18 pagesProcuement and Supply Management PDFBhargavShridharNo ratings yet
- CBA - s17 - Class NotesDocument78 pagesCBA - s17 - Class NotesEric YoungNo ratings yet
- Case 2Document17 pagesCase 2Suraj KumarNo ratings yet
- k15 - Manajemen-Performa FPDocument37 pagesk15 - Manajemen-Performa FPYunandhika RizkiNo ratings yet
- Centric HealthDocument38 pagesCentric HealthJenny QuachNo ratings yet
- Nursing Administration II: Amelinda Saldua MagnoDocument12 pagesNursing Administration II: Amelinda Saldua MagnoJessica Ella Hernandez AgundayNo ratings yet
- Nursing InformaticsDocument18 pagesNursing InformaticsKeannu GervacioNo ratings yet
- Narrow Health Cares Quality PDFDocument8 pagesNarrow Health Cares Quality PDFakram75zaaraNo ratings yet
- India Healthcare Understanding Healthtech Opportunity 1702616723Document20 pagesIndia Healthcare Understanding Healthtech Opportunity 1702616723gaurav aroraNo ratings yet
- Case 2 Compress PDFDocument17 pagesCase 2 Compress PDFAbhinav KumarNo ratings yet
- My Private Health ReportDocument10 pagesMy Private Health ReportNamhar AnimasNo ratings yet
- Healthscore: The Credit Score For Your LifeDocument34 pagesHealthscore: The Credit Score For Your LifegabepolkNo ratings yet
- 1 - Introduction To Health Economics 2020Document24 pages1 - Introduction To Health Economics 2020Emy AL-AnaziNo ratings yet
- 2 From Volume To ValueDocument20 pages2 From Volume To ValueAR J LopezNo ratings yet
- Understanding Community HealthDocument35 pagesUnderstanding Community HealthNational Press FoundationNo ratings yet
- Prioritization in Health CareDocument35 pagesPrioritization in Health CareArin BasuNo ratings yet
- Top 10 Health Care Innovations:: Achieving More For LessDocument15 pagesTop 10 Health Care Innovations:: Achieving More For LessMohd TauqeerNo ratings yet
- Reference-"Low Vision Assessment" - by Jane Mcnaughton, Jane Mcnaughton (Mcoptom.)Document10 pagesReference-"Low Vision Assessment" - by Jane Mcnaughton, Jane Mcnaughton (Mcoptom.)Ahil PrasanthNo ratings yet
- Servicom Presentation For Capacity BuildingDocument44 pagesServicom Presentation For Capacity BuildingMargaret DigitemieNo ratings yet
- Health Care SystemDocument3 pagesHealth Care SystemAnwarNo ratings yet
- Vermont Report Recommends Single Payer System - Presentation To The State LegislatureDocument33 pagesVermont Report Recommends Single Payer System - Presentation To The State LegislatureRich ElmoreNo ratings yet
- Healthcare Information Technology-Some Thoughts On Future TrendsDocument21 pagesHealthcare Information Technology-Some Thoughts On Future TrendsalaharigovindaNo ratings yet
- BeFit - BenefitDocument1 pageBeFit - BenefitR.c singhNo ratings yet
- Leadership and Innovation-High Quality Nursing CareDocument36 pagesLeadership and Innovation-High Quality Nursing Caresubinj_3No ratings yet
- Aravind Eye Care Systems: Providing Total Eye Care To The Rural PopulationDocument13 pagesAravind Eye Care Systems: Providing Total Eye Care To The Rural PopulationAvik BorahNo ratings yet
- Session 1 - HSMDocument32 pagesSession 1 - HSMlaxman kavitkarNo ratings yet
- HFI Intro2023-24Document50 pagesHFI Intro2023-24saurabh chaturvediNo ratings yet
- 2010 Global Survey of Health Care Consumers: Behaviors, Attitudes and Unmet NeedsDocument24 pages2010 Global Survey of Health Care Consumers: Behaviors, Attitudes and Unmet Needsapi-26178438No ratings yet
- Do Wellness Programs Work - Chapman 2007Document22 pagesDo Wellness Programs Work - Chapman 2007kedar2013No ratings yet
- Meri Health Seed (Autosaved) 1Document15 pagesMeri Health Seed (Autosaved) 1Meri HealthNo ratings yet
- Six Sigma and Its Application To HealthcareDocument20 pagesSix Sigma and Its Application To HealthcareAkash Bhagat100% (1)
- Implementing An Effective Employee Wellness ProgramDocument38 pagesImplementing An Effective Employee Wellness ProgramAndrew Hinkebein100% (1)
- NH - Cardiac Care of The PoorDocument11 pagesNH - Cardiac Care of The PoorJordan ScottNo ratings yet
- BestDocument7 pagesBestanuragluminarNo ratings yet
- Leadership Exam 2Document14 pagesLeadership Exam 2Zinou HarcheNo ratings yet
- Prepared by Deva Malar Vengrasalam (Zp03320) Mogana Rawan (Zp03316) Lynn Al Jarrah (Zp03436) Parimala Chandran (Zp03476)Document17 pagesPrepared by Deva Malar Vengrasalam (Zp03320) Mogana Rawan (Zp03316) Lynn Al Jarrah (Zp03436) Parimala Chandran (Zp03476)Mogana RawanNo ratings yet
- Quantum Health Results That Matter PDFDocument2 pagesQuantum Health Results That Matter PDFkbrinaldiNo ratings yet
- Health Care System Performance: By: Masheal Alsouhih Amjad Almutairi Supervised By: DR - Hanan AlgorashiDocument49 pagesHealth Care System Performance: By: Masheal Alsouhih Amjad Almutairi Supervised By: DR - Hanan AlgorashiAmjad100% (1)
- Strategic PurchasingDocument20 pagesStrategic PurchasingElmar D UmipigNo ratings yet
- Quality in Healthcare and Need For AccreditationDocument20 pagesQuality in Healthcare and Need For AccreditationVidyasagar SeerapuNo ratings yet
- Muslim Prayer-A New Form of Physical Activity: A Narrative ReviewDocument8 pagesMuslim Prayer-A New Form of Physical Activity: A Narrative ReviewMuhammad jamilNo ratings yet
- Lord of Shadows - Cassandra Clare 2Document676 pagesLord of Shadows - Cassandra Clare 2Joy AusiNo ratings yet
- Procedure For Adverse Event Reporting-AOC1Document6 pagesProcedure For Adverse Event Reporting-AOC1Mohamed EzzatNo ratings yet
- IMS Internal Audit Checklist: Clause Title Sub Clauses Sub Title Clause NumberDocument64 pagesIMS Internal Audit Checklist: Clause Title Sub Clauses Sub Title Clause Numberfadi713No ratings yet
- Dentistry For General Medicine: - Part 2 - Dental SurgeryDocument52 pagesDentistry For General Medicine: - Part 2 - Dental SurgeryDimitrios PapadopoulosNo ratings yet
- Job Safety Analysis and PPEDocument3 pagesJob Safety Analysis and PPEMazen ZarqanNo ratings yet
- ZLY 203 Pesticide Mode of ActionDocument18 pagesZLY 203 Pesticide Mode of ActionAdeoyeNo ratings yet
- 2020-08-22 New Scientist International Edition PDFDocument62 pages2020-08-22 New Scientist International Edition PDFrsanchez-No ratings yet
- Doctors LetterDocument34 pagesDoctors LetterOFC accountNo ratings yet
- Case Study 4Document2 pagesCase Study 4Dwaine TolentinoNo ratings yet
- Master Your Emotions Sedona MethodDocument156 pagesMaster Your Emotions Sedona MethodMurselica100% (11)
- Writing An Analytical EssayDocument4 pagesWriting An Analytical Essayafhbgrgbi100% (2)
- Picture Analysis What Can You Do To Help These People Around You?Document5 pagesPicture Analysis What Can You Do To Help These People Around You?Zhane LabradorNo ratings yet
- Qualitative and Quantitative Research Literature ReviewDocument8 pagesQualitative and Quantitative Research Literature Reviewc5haeg0nNo ratings yet
- Doctor ExhibitDocument110 pagesDoctor ExhibitKFORNo ratings yet
- Microbiology & Parasitology (Collection, Handling, and Storage of Laboratory Specimen - A Nursing Perspective)Document65 pagesMicrobiology & Parasitology (Collection, Handling, and Storage of Laboratory Specimen - A Nursing Perspective)Kyle ChuaNo ratings yet
- Eyewitness Testimony.Document6 pagesEyewitness Testimony.anorus97No ratings yet
- Untitled NotebookDocument3 pagesUntitled NotebookMuhammad Abelsea OktanzaNo ratings yet
- Digital X Ray For Smart Diagnostic System in EmergencyDocument23 pagesDigital X Ray For Smart Diagnostic System in EmergencynaamiiNo ratings yet
- Dissertation: Dr.M.Arunkumar. 1st Year Postgraduate Department of Community Medicine, SRMC & RiDocument27 pagesDissertation: Dr.M.Arunkumar. 1st Year Postgraduate Department of Community Medicine, SRMC & Rirajforever17No ratings yet
- Health Technology Assessment (HTA) GuidelineDocument163 pagesHealth Technology Assessment (HTA) Guidelinebella friscaamaliaNo ratings yet
- Cardiovascular Safety of Naltrexone and Bupropion Therapy Systematic Review and Meta-AnalysesDocument9 pagesCardiovascular Safety of Naltrexone and Bupropion Therapy Systematic Review and Meta-AnalysesPlinio ReisNo ratings yet
- Un ScriptDocument2 pagesUn ScriptPeterClomaJr.No ratings yet
- National Assessment and Certification Arrangements: ReferencesDocument25 pagesNational Assessment and Certification Arrangements: ReferencesCharlton Benedict Bernabe100% (1)
- Eating All Together: 28 September - 4 October 2022 Vicchio, ItalyDocument18 pagesEating All Together: 28 September - 4 October 2022 Vicchio, ItalyLeraNo ratings yet
- Revise-Spiritual Orientation. Issh 2023 PPT TemplateDocument13 pagesRevise-Spiritual Orientation. Issh 2023 PPT TemplateHarold Auditor GaringNo ratings yet
- Ylang Ylang Essential OilDocument3 pagesYlang Ylang Essential OilBradfield & Durham InternationalNo ratings yet
- Stablcal Msds 2.16.10Document59 pagesStablcal Msds 2.16.10Cristian VegaNo ratings yet
- The Dangers of Smoking in The MorningDocument3 pagesThe Dangers of Smoking in The MorningAuw SinNo ratings yet
- مشيناها خطى محمد فتحي عبد العال نسخة منقحة ومراجعة ومزيدة حتى نهاية 2024Document25 pagesمشيناها خطى محمد فتحي عبد العال نسخة منقحة ومراجعة ومزيدة حتى نهاية 2024mohamed fathi abdel aalNo ratings yet