Professional Documents
Culture Documents
1-s2.0-S0140673624009218-main
1-s2.0-S0140673624009218-main
Uploaded by
Vinícius NavesCopyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
1-s2.0-S0140673624009218-main
1-s2.0-S0140673624009218-main
Uploaded by
Vinícius NavesCopyright:
Available Formats
Articles
Tenecteplase versus standard of care for minor ischaemic
stroke with proven occlusion (TEMPO-2): a randomised,
open label, phase 3 superiority trial
Shelagh B Coutts, Sandeep Ankolekar, Ramana Appireddy, Juan F Arenillas, Zarina Assis, Peter Bailey, Philip A Barber, Rodrigo Bazan,
Brian H Buck, Ken S Butcher, Marie-Christine Camden, Bruce C V Campbell, Leanne K Casaubon, Luciana Catanese, Kausik Chatterjee,
Philip M C Choi, Brian Clarke, Dar Dowlatshahi, Julia Ferrari, Thalia S Field, Aravind Ganesh, Darshan Ghia, Mayank Goyal, Stefan Greisenegger,
Omid Halse, Mackenzie Horn, Gary Hunter, Oje Imoukhuede, Peter J Kelly, James Kennedy, Carol Kenney, Timothy J Kleinig, Kailash Krishnan,
Fabricio Lima, Jennifer L Mandzia, Martha Marko, Sheila O Martins, George Medvedev, Bijoy K Menon, Sachin M Mishra, Carlos Molina,
Aimen Moussaddy, Keith W Muir, Mark W Parsons, Andrew M W Penn, Arthur Pille, Octávio M Pontes-Neto, Christine Roffe, Joaquin Serena,
Robert Simister, Nishita Singh, Neil Spratt, Daniel Strbian, Carol H Tham, M Ivan Wiggam, David J Williams, Mark R Willmot, Teddy Wu,
Amy Y X Yu, George Zachariah, Atif Zafar, Charlotte Zerna, Michael D Hill, on behalf of the TEMPO-2 investigators*
Summary
Background Individuals with minor ischaemic stroke and intracranial occlusion are at increased risk of poor outcomes. Lancet 2024; 403: 2597–605
Intravenous thrombolysis with tenecteplase might improve outcomes in this population. We aimed to test the Published Online
superiority of intravenous tenecteplase over non-thrombolytic standard of care in patients with minor ischaemic May 17, 2024
stroke and intracranial occlusion or focal perfusion abnormality. https://doi.org/10.1016/
S0140-6736(24)00921-8
This online publication has been
Methods In this multicentre, prospective, parallel group, open label with blinded outcome assessment, randomised corrected. The corrected version
controlled trial, adult patients (aged ≥18 years) were included at 48 hospitals in Australia, Austria, Brazil, Canada, first appeared at thelancet.com
Finland, Ireland, New Zealand, Singapore, Spain, and the UK. Eligible patients with minor acute ischaemic stroke on June 13, 2024
(National Institutes of Health Stroke Scale score 0–5) and intracranial occlusion or focal perfusion abnormality were See Comment page 2566
enrolled within 12 h from stroke onset. Participants were randomly assigned (1:1), using a minimal sufficient balance *TEMPO-2 investigators are
algorithm to intravenous tenecteplase (0·25 mg/kg) or non-thrombolytic standard of care (control). Primary outcome listed in the appendix
was a return to baseline functioning on pre-morbid modified Rankin Scale score in the intention-to-treat (ITT) Department of Clinical
population (all patients randomly assigned to a treatment group and who did not withdraw consent to participate) Neurosciences
(Prof S B Coutts MD,
assessed at 90 days. Safety outcomes were reported in the ITT population and included symptomatic intracranial P A Barber MD,
haemorrhage and death. This trial is registered with ClinicalTrials.gov, NCT02398656, and is closed to accrual. A Ganesh MD, Prof M Goyal MD,
M Horn BSc, C Kenney RN,
Prof B K Menon MD,
Findings The trial was stopped early for futility. Between April 27, 2015, and Jan 19, 2024, 886 patients were enrolled;
C Zerna MD, Prof M D Hill MD),
369 (42%) were female and 517 (58%) were male. 454 (51%) were assigned to control and 432 (49%) to intravenous Department of Radiology
tenecteplase. The primary outcome occurred in 338 (75%) of 452 patients in the control group and 309 (72%) of 432 (Prof S B Coutts, Prof M Goyal,
in the tenecteplase group (risk ratio [RR] 0·96, 95% CI 0·88–1·04, p=0·29). More patients died in the tenecteplase Prof B K Menon, Prof M D Hill),
Department of Community
group (20 deaths [5%]) than in the control group (five deaths [1%]; adjusted hazard ratio 3·8; 95% CI 1·4–10·2,
Health Sciences (Prof S B Coutts,
p=0·0085). There were eight (2%) symptomatic intracranial haemorrhages in the tenecteplase group versus two (<1%) A Ganesh, Prof B K Menon,
in the control group (RR 4·2; 95% CI 0·9–19·7, p=0·059). Prof M D Hill), and Department
of Medicine (Prof M D Hill),
Hotchkiss Brain Institute
Interpretation There was no benefit and possible harm from treatment with intravenous tenecteplase. Patients with
(Prof S B Coutts, A Ganesh,
minor stroke and intracranial occlusion should not be routinely treated with intravenous thrombolysis. Prof M Goyal, Prof B K Menon,
Prof M D Hill), and the O’Brien
Funding Heart and Stroke Foundation of Canada, Canadian Institutes of Health Research, and the British Heart Institute for Public Health
(A Ganesh), Cumming School of
Foundation.
Medicine, University of
Calgary, Calgary, AB, Canada;
Copyright © 2024 Elsevier Ltd. All rights reserved, including those for text and data mining, AI training, and similar Department of Neurology,
technologies. King’s College Hospital London,
UK (S Ankolekar FRCP); Division
of Neurology, Department of
Introduction intracranial occlusion are a subpopulation at high risk Medicine, Queen’s University,
Up to 50% of patients with ischaemic stroke initially for early neurological deterioration,5,6 which most often Kingston, ON, Canada
present with minimal symptoms which are non- occurs within the first 24 h after presentation.5 This is (R Appireddy MD); Stroke
Program, Department of
disabling.1 Despite having low scores on the National true even if the deficits have resolved.7 Nevertheless, Neurology, Hospital Clínico
Institutes of Health Stroke Scale (NIHSS), typically minor deficits are a common reason for withholding Universitario, Valladolid, Spain
ranging from 0 to 5, a third of such patients are dead or thrombolysis,2 as many physicians have concerns (J F Arenillas PhD); Valladolid
disabled at 90-day follow-up if thrombolysis is withheld.2–4 regarding the potential harm from bleeding in the Health Research Institute,
Department of Medicine,
Patients with minor deficits and evidence of an absence of major deficits. Most stroke thrombolysis trials
www.thelancet.com Vol 403 June 15, 2024 2597
Articles
University of Valladolid,
Valladolid, Spain (J F Arenillas); Research in context
Department of Imaging,
Foothills Medical Centre, Evidence before this study Added value of this study
Calgary, AB, Canada Intravenous thrombolysis with both alteplase and tenecteplase This is the first phase 3 study to examine the efficacy of
(Z Assis MD); Alberta Children’s has been proven to improve clinical outcomes after ischaemic thrombolysis with tenecteplase in minor ischaemic stroke
Hospital, Calgary, AB, Canada
(Z Assis); Griffith University,
stroke. However, for patients with minor deficits, thrombolysis patients with intracranial occlusion within 12 h of onset. The trial
Gold Coast, QLD, Australia with either agent has not been shown to be superior to showed that patients do not benefit from treatment with
(P Bailey MD); Botucatu Medical antiplatelet agents. The subgroup of patients with intracranial tenecteplase and that there is potential harm. This large, well
School, São Paulo State occlusion and minor stroke have an elevated risk of early conducted trial had a pragmatic control reflecting clinical practice.
University, San Paulo, Brazil
deterioration and disability. We searched MEDLINE and PubMed
(Prof R Bazan MD); Division of Implications of all the available evidence
Neurology, Department of for randomised trials published in English between Jan 1, 2000,
Findings from our study suggest that minor ischaemic stroke
Medicine, University of and March 31, 2024, using the terms “stroke”, “tenecteplase”, and
Alberta, Edmonton, AB, patients with intracranial occlusion should not be treated with
“alteplase”, and “trial or study”. We could not identify any
Canada (B H Buck MD, intravenous thrombolysis with tenecteplase and that
phase 3 randomised trials comparing tenecteplase or alteplase
S M Mishra MD); School of antiplatelet therapy is sufficient.
Clinical Medicine, University of with antiplatelet agents in patients with minor stroke and
New South Wales, NSW, intracranial occlusion. Two phase 3 trials compared alteplase with
Australia (Prof K S Butcher PhD); antiplatelet agents in minor stroke, but none looked at the subset
CHU de Québec–Hôpital de
l’Enfant-Jésus, Quebec City, QC,
with intracranial occlusion and none looked at tenecteplase.
Canada (Prof M-C Camden MD);
Department of Medicine and
Neurology, Melbourne Brain have excluded patients with minor stroke and thus high- non-inferior to alteplase,12,13 which has led to guideline
Centre at the Royal
quality data to guide thrombolytic treatment in these changes, with intravenous tenecteplase (0·25 mg/kg) now
Melbourne Hospital,
University of Melbourne, patients are scarce. recommended for use in ischaemic stroke within 4·5 h
Parkville, VIC, Australia An individual patient data meta-analysis of the subset of of symptom onset.14–16 The TIMELESS study17 included
(Prof B C V Campbell PhD); patients with minor stroke included in randomised trials patients with disabling stroke between 4·5 h and 24∙0 h from
University Health Network–
of thrombolysis with intravenous alteplase suggested that onset with potentially salvageable tissue defined by CT
Toronto Western Hospital
(L K Casaubon MD) and thrombolysis improved outcomes in these individuals perfusion imaging and randomly assigned patients to
Neurology, Department of (odds ratio [OR] 1·48, for good outcome [modified Rankin treatment with standard of care or intravenous
Medicine, Sunnybrook Health Scale, mRS score, 0–1] adjusted for age and time from tenecteplase. Although there was no observable difference
Sciences Centre (A Y X Yu MD),
onset; 95% CI 1·07−2·06).8 However, randomised trials in outcomes between groups in TIMELESS, there was no
University of Toronto, Toronto,
ON, Canada; McMaster examining thrombolysis exclusively in individuals with evidence of harm when tenecteplase was given in
University, Population Health minor stroke have not shown benefit over antiplatelet the 24 h time window. The TWIST study found similar
Research Institute, Hamilton, therapy. The PRISMS trial compared intravenous alteplase safety in patients with stroke on awakening.18 The
ON, Canada (L Catanese MD);
Countess of Chester Hospital
against aspirin monotherapy and showed no significant TEMPO-119 study, which was a phase 2 dose escalation
NHS Foundation Trust, Chester, difference in 90-day functional outcomes between groups safety study assessing the feasibility of using tenecteplase
UK (Prof K Chatterjee MD); and higher rates of symptomatic intracerebral in the treatment of minor stroke patients with intracranial
Department of Neuroscience, haemorrhage in the alteplase group.9 The ARAMIS non- occlusion, showed a low symptomatic intracranial
Box Hill Hospital, Eastern
Health, Melbourne, VIC,
inferiority trial (–4·5% non-inferiority margin) found that haemorrhage rate (4%) and high recanalisation rates at
Australia (P M C Choi MBChB); dual antiplatelet therapy was non-inferior to intravenous the 0·25 mg/kg dose. All of these studies12,17–19 have shown
Eastern Health Clinical School, alteplase for excellent functional outcome at 90 days with the safety of thrombolysis with tenecteplase in selected
Monash University, Melbourne, no significant difference in the risk of symptomatic patients within 4·5 h and after 4·5 h from stroke onset.
VIC, Australia (P M C Choi);
St George’s University
intracranial haemorrhage between groups.10 Both trials The TEMPO-2 trial was designed to show superiority of
Hospitals, London, UK used intravenous alteplase as the comparative thrombolytic intravenous tenecteplase (0·25 mg/kg) as compared with
(B Clarke MRCPI); Department agent and restricted enrolment to either 3∙0 or 4·5 h from non-thrombolytic standard of care in patients with minor
of Medicine, University of symptom onset. Both trials also tried to exclude patients stroke with intracranial occlusion or focal perfusion
Ottawa, Ottawa, ON, Canada
(Prof D Dowlatshahi MD);
who could be at elevated risk for disability within this low lesion presenting within 12 h from symptom onset, on
Ottawa Hospital Research NIHSS population by excluding patients scoring higher on 90-day functional outcomes assessed with mRS.
Institute, Ottawa Hospital, certain subcategories of the NIHSS. Neither study focused
Ottawa, ON, Canada specifically on the subpopulation with intracranial Methods
(Prof D Dowlatshahi);
Department of Neurology,
occlusion who seem to be at the highest risk for early Study design and participants
St John’s of God Hospital deterioration and disability.5,6 TEMPO-2 was an investigator-initiated, multicentre,
Vienna, Vienna, Austria Tenecteplase, a recombinant human tissue plasminogen prospective, randomised, open-label with blinded
(J Ferrari MD); Vancouver Stroke
activator similar to alteplase, has a longer half-life in part endpoint assessment (PROBE), parallel group, controlled
Program, Division of
Neurology (T S Field MD) and due to resistance to plasminogen activator inhibitor, it is trial, designed to test the superiority of intravenous
Royal Columbian Hospital more fibrin-specific, and results in less systemic depletion tenecteplase (0·25 mg/kg) over non-thrombolytic
(G Medvedev MD), University of of circulating fibrinogen as compared with alteplase.11 The standard of care in patients with minor ischaemic stroke
British Columbia, Vancouver,
AcT trial and others have shown that tenecteplase is deficits, defined as NIHSS 0–5, and intracranial occlusion
2598 www.thelancet.com Vol 403 June 15, 2024
Articles
or focal perfusion lesion within 12 h from onset of randomisation after which the minimal sufficient BC, Canada; Fiona Stanley
symptoms. The trial was conducted at 48 hospitals balance algorithm was activated. The standard Hospital, Murdoch, Western
Australia, University of
in Australia, Austria, Brazil, Canada, Finland, Ireland, distribution for randomisation was 50:50, but when an Western Australia, Perth, WA,
New Zealand, Singapore, Spain, and the UK. The imbalance was detected, the distribution was biased to Australia (D Ghia MD);
methods of this trial have been previously published,20 65:35 in the direction against the imbalance; thus, there Department of Neurology,
and the protocol and statistical analysis plan are available were no deterministic allocations. Randomisation was Medical University of Vienna,
Vienna, Austria
in the appendix. The trial was sponsored by the University dynamic and generated in the moment via a web-based (Prof S Greisenegger MD,
of Calgary, AB, Canada. Data management and system such that the sequence of allocation was fully M Marko MD); Imperial College
monitoring were conducted by the University of Calgary. masked. Treatment allocation was open-label. Healthcare Trust, London, UK
The trial was monitored by an independent data and (O Halse MBBS); University of
Saskatchewan, Saskatoon, SK,
safety monitoring committee (DSMC) that conducted two Procedures Canada (G Hunter MD); Red
planned unblinded interim safety analyses, one additional Patients randomly assigned to tenecteplase received Deer Regional Hospital Centre,
safety assessment and one planned interim analysis 0·25 mg/kg (maximum dose of 50 mg) as a single, Red Deer, AB, Canada
(DSMC members are listed in the appendix [p 2]). The intravenous bolus administered over 5–10 s immediately (O Imoukhuede MD); School of
Medicine University College
trial was regulated by Health Canada and elsewhere as after randomisation. Patients assigned to control were Dublin–Mater University
required in individual countries. The trial protocol was treated with non-thrombolytic treatment. Per protocol, at Hospital Dublin, Dublin, Ireland
approved by local ethics boards. All patients or their minimum all patients received single agent antiplatelet (Prof P J Kelly MD); Acute
Multidisciplinary Imaging and
representative provided written informed consent as therapy. Guideline-based care was recommended and
Interventional Centre, John
approved by local ethics boards. Patients were eligible if this was implemented by the local investigator who chose Radcliffe Hospital, Radcliffe
they were 18 years or older; were functionally independent which antithrombotic regimen should be used. Standard Department of Medicine,
before the stroke (baseline pre-stroke mRS 0–2); had a of care medications were given immediately after University of Oxford, Oxford,
UK (J Kennedy MSc);
minor stroke with NIHSS score of 0–5, presented within randomisation. Imaging was reviewed centrally at the
Department of Neurology,
12 h of last seen normal; had direct imaging evidence of University of Calgary core laboratory by a neuroradiologist Royal Adelaide Hospital,
an intracranial occlusion or indirect evidence of occlusion (ZA) blinded to clinical information and treatment Adelaide, SA, Australia
with a focal perfusion lesion relevant to the presenting assignment. Imaging was assessed to confirm that (Prof T J Kleinig MD);
Department of Medicine,
symptoms; and had no region of well evolved infarction patients met imaging entry criteria, recanalisation status
University of Adelaide,
concordant with the acute presenting syndrome and an was assessed on imaging done at 4–8 h from Adelaide, SA, Australia
Alberta Stroke Program Early CT score (ASPECTS)21 randomisation in patients with direct evidence of (Prof T J Kleinig); Queen’s
of 7 or greater. Perfusion imaging was not mandatory. occlusion, and follow-up imaging was assessed for any Medical Centre, Nottingham
University Hospitals NHS Trust,
Patients were not eligible if, in the judgement of the intracranial haemorrhage, classified using the Heidelberg
Nottingham, UK
physician and the patient, routine intravenous bleeding classification.25 (K Krishnan PhD); Hospital Geral
thrombolysis treatment was warranted. The main De Fortaleza, Fortaleza, Brazil
exclusion criteria were standard contraindications to Outcomes (F Lima MD); Department of
Clinical Neurological Sciences,
intravenous thrombolysis. Full inclusion and exclusion The primary outcome was assessed at 90 days by an Western University, London,
criteria are available in the study protocol. All patients investigator blinded to the treatment allocation. The ON, Canada (J L Mandzia MD);
were provided with standard stroke unit care, primary outcome was defined as return to baseline Hospital de Clínicas de Porto
investigations for stroke mechanism, and stroke neurological functioning as measured by the mRS, using Alegre (Prof S O Martins MD)
and Neurology Department
prevention care according to current guidelines. Patients a sliding dichotomy approach. A responder was defined (A Pille MD), Hospital Moinhos
with evidence of a vessel occlusion on baseline CT as follows: (1) if the pre-morbid mRS is 0–1, then mRS de Vento, Porto Alegre, Brazil;
angiogram underwent a follow-up CT angiogram of the 0–1 at 90 days is a responder (good outcome) or (2) if the Vall d’Hebron Stroke Center,
intracranial circulation at 4–8 h after randomisation in pre-morbid mRS is 2, then mRS 0–2 is a responder (good Hospital Vall d’Hebron,
Barcelona, Spain
both groups to determine early recanalisation status of outcome). All raters were trained and certified in the use (Prof C Molina MD); Montreal
the occluded artery. All patients underwent routine of the mRS. Neurological Institute, McGill
follow-up brain imaging at 24 h with either CT or MR. Baseline pre-morbid mRS was assessed using the University Health Centre,
structured mRS before randomisation.26 The 90-day mRS Montreal, QC, Canada
(A Moussaddy MD); School of
Randomisation and masking was rated using the structured mRS questionnaire.26 The Neuroscience and Psychology,
Patients were randomly assigned (1:1) to intravenous 90-day mRS was completed in person where possible and University of Glasgow,
tenecteplase versus non-thrombolytic standard of care by telephone otherwise. The structured questionnaire has Glasgow, UK
(control). Randomisation was completed by a computer- been shown to improve reliability in assessing the mRS (Prof K W Muir MD);
Department of Neurology,
generated minimisation algorithm, minimal sufficient both in person and by telephone.26 Secondary outcomes Liverpool Hospital, UNSW
balance randomisation, to ensure balance on key included the absence of disability, defined as return to South West Sydney, Sydney,
variables (age, sex assigned at birth, baseline NIHSS exact baseline mRS or better, functional independence NSW, Australia
(Prof M W Parsons PhD); Victoria
score, and time from symptom onset to randomisation).22 defined as 90-day mRS 0–2, comparison of the mean
General Hospital, Victoria, BC,
These are the key variables known to influence outcome 90-day mRS with linear regression using the mRS as a Canada (A M W Penn MD);
in minor stroke.6,23,24 This algorithm was developed continuous variable, percent function on Lawton Ribeirao Preto Medical School,
centrally and the details were not available to the treating Instrumental Activities of Daily Living Scale at 90 days,24 University of Sao Paulo,
Ribeirao Preto, Brazil
sites. The first 40 patients were assigned using simple NIHSS at day 5 or on day of hospital discharge (whichever
www.thelancet.com Vol 403 June 15, 2024 2599
Articles
(O M Pontes-Neto MD); Stroke is earlier), quality of life measured at 90 days on the subarachnoid, intraventricular, or subdural haemorrhage)
Research, Keele University, European Quality of Life score, five dimensions, five associated with clinical evidence of neurological
Stoke-on-Trent, UK
(Prof C Roffe MD); Stroke Unit,
levels (EQ-5D-5L),27 stroke progression and recurrent worsening, in which the haemorrhage was judged to be
Neurology Department, stroke,7 all-cause mortality, and proportion of patients the most important cause of the neurological worsening.
Hospital Trueta de Girona, receiving rescue endovascular thrombectomy for the Clinical worsening was defined by the NIHSS score
Fundació Institut index stroke and recanalisation at 4–8 h.28 Recanalisation worsening a minimum of 2 or more points different from
d’Investigació Biomèdica de
Girona Dr Josep Trueta, Girona,
was only assessed in patients with direct evidence of baseline. The Heidelberg bleeding classification25 was
Spain (J Serena MD); University occlusion seen on baseline CT angiogram. Stroke used for assessing intracranial haemorrhage on follow-up
College Hospitals London, progression was defined as a clear functional worsening imaging. Major extracranial haemorrhage was defined as
London, UK (R Simister MD); where the imaging and clinical symptomology supported life-threatening bleeding, resulting in haemodynamic
Rady Faculty of Health
Sciences, University of
a worsening of the presenting event rather than a distinct compromise or hypovolemic shock, requiring inotropic
Manitoba, Winnipeg, MB, new event.7 support or other means to maintain cardiac output,
Canada (N Singh MD); School of The main safety outcome was the proportion of patients requiring blood transfusion of more than 2 units of
Biomedical Sciences and with major bleeding within 48 h of randomisation. This packed red blood cells, or associated with a fall in
Pharmacy, University of
Newcastle, Newcastle, NSW,
included symptomatic intracranial haemorrhage alone as haemoglobin greater than or equal to 5 g/L, temporally
Australia (Prof N Spratt PhD); well as a composite of symptomatic intracranial related to the treatment.
Heart and Stroke Program, haemorrhage and major extracranial haemorrhage.
Hunter Medical Research
Symptomatic intracranial haemorrhage was defined as Statistical analysis
Institute, Newcastle, NSW,
new intracranial haemorrhage (intracerebral, The statistical analysis plan was finalised before database
lock (on April 10, 2024). Past literature showed an effect
size of 10% in the subset of minor stroke patients treated
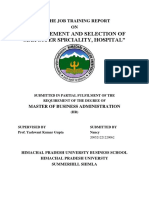
886 participants enrolled and with thrombolysis.8 Previous trials included in the meta-
randomly assigned analysis of individuals with minor stroke did not require
patients to have an intracranial occlusion. We expected
that the effect size of thrombolysis would be greater in a
432 assigned to tenecteplase 454 assigned to control population exclusively comprised of individuals with an
intracranial occlusion. We estimated the sample based
upon a predicted effective size of 9% absolute risk
2 withdrew consent reduction. In TEMPO-1,19 incidence of the primary
outcome (mRS score 0–1) at 90 days was 66% in the
432 included in intention-to-treat 452 included in intention-to-treat combined 0·1 mg/kg and 0·25 mg/kg tenecteplase-
population population treated groups. Based on this we estimated
60% good outcome in the control group and 69% in the
tenecteplase-treated group for a sample size of
7 excluded 8 excluded
1 patient crossed over to control 4 crossed over to thrombolysis and 614 patients in each group (1228 total). Adding 4% loss to
and was given aspirin plus were given intravenous alteplase follow-up and adjusting for a single interim analysis for
clopidogrel 3 had no occlusion detected
5 had no occlusion detected 1 randomised >12 h from onset efficacy gave a sample size estimate of 1274 patients
(1 of these was also a crossover) (637 in each treatment group).
1 had low ASPECTS
1 randomised >12 h from onset
An independent DSMC completed prespecified interim
safety analyses after 100 patients and 450 patients were
enrolled. There was a signal of excess deaths in the
425 received tenecteplase 444 received standard of care tenecteplase group at the second safety review and an
258 received aspirin plus clopidogrel
103 received aspirin additional safety analysis was completed after 650 patients
50 received clopidogrel were enrolled. There was one planned interim analysis
17 received heparin or low
molecular weight heparin
after 850 patients had completed follow-up. At this interim
10 received a DOAC analysis, the DSMC recommended stopping the trial.
4 received aspirin plus ticagleror Outcomes for patients that were lost to follow-up were
2 did not receive any treatment*
imputed as non-responders in the primary outcome but
no imputation was done for two patients who withdrew
2 lost to follow-up consent. For individual secondary outcomes on the
mRS scores, no missing data were imputed. We
imputed the worst possible score for the EQ-5D-5L,
425 included in per-protocol analysis 442 included in per-protocol analysis
Lawton Index, mRS, and NIHSS scores for patients who
were known to be deceased at 90 days. Missing values
Figure 1: Trial profile
on the NIHSS score at 5 days or discharge were imputed
Exclusions data can overlap. ASPECTS=Alberta Stroke Program Early CT score. DOAC=direct oral anticoagulant.
*Two patients were not given antiplatelet agents after randomisation as they had already taken antiplatelets at using the last score carried forward principle. Missing
home. imaging variables were not imputed.
2600 www.thelancet.com Vol 403 June 15, 2024
Articles
We analysed the primary outcome in the intention-to- Australia (Prof N Spratt);
treat (ITT) population, defined as all patients randomly Department of Neurology,
John Hunter Hospital,
assigned to a treatment group and who did not withdraw Newcastle, NSW, Australia
Control Tenecteplase
consent to participate. The primary outcome analysis was (n=452) (n=432) (Prof N Spratt); Department of
unadjusted. Secondary analysis included primary outcome Neurology, Helsinki University
Demographics Hospital and University
analysis adjusted for age, sex at birth, baseline NIHSS,
Age, years 72 (61–79) 72 (62–80) ofHelsinki, Helsinki, Finland
and time from symptom onset to randomisation and all (D Strbian MD); National
Sex at birth
secondary outcomes analysed unadjusted and adjusted for Neuroscience Institute,
Male 272 (60%) 244 (56%)
the same variables. These variables were chosen a priori Singapore (C H Tham MRCP);
Female 180 (40%) 188 (44%) Royal Victoria Hospital, Belfast,
because they are of prognostic or epidemiological
Race UK (M I Wiggam MD); RCSI
importance and because these variables were used in the University of Medicine and
White 382 (85%) 371 (86%)
randomised minimisation algorithm. We used generalised Health Sciences and Beaumont
linear modelling with a Poisson distribution and log link Asian 42 (9%) 40 (9%) Hospital, Dublin, Ireland
function in order to directly generate risk ratios. Robust Black 7 (2%) 6 (1%) (Prof D J Williams PhD);
First Nations 5 (1%) 4 (1%) University Hospitals
(Huber–Sandwich) standard error estimation was used. Birmingham NHS Trust,
We modelled death using survival analysis. A multivariable Pacific Islander 0 1 (<1%)
Birmingham, UK
model adjusting for age, sex at birth, onset-to- Other 16 (4%) 10 (2%) (M R Willmot MD); Department
Ethnicity of Neurology, Christchurch
randomisation time, and baseline NIHSS score was
Hospital, Christchurch,
developed using a Cox model. The proportional hazards Hispanic 9 (2%) 5 (1%)
New Zealand (T Wu PhD);
assumption was assessed graphically and statistically. Non-Hispanic 443 (98%) 427 (99%) Cambridge University
Using multiplicative interaction terms, we assessed for Medical history Hospitals NHS Trust,
Cambridge, UK
heterogeneity of treatment effect across the prespecified Hypertension 261 (58%) 265 (61%)
(G Zachariah MBBS); Unity
subgroups of sex (male vs female), timing of treatment Past smoking 176 (39%) 172 (40%) Health Toronto, St Michael’s
(≤4·5 h and >4·5 h from symptom onset), age Hyperlipidaemia 172 (38%) 180 (42%) Hospital, Toronto, ON, Canada
(≤80 and >80 years), how occlusion was identified (directly Diabetes 86 (19%) 82 (19%) (A Zafar MD); Städtisches
Klinikum Dresden, Dresden,
observed on CT angiography vs inferred from CT Past stroke 85 (19%) 72 (17%)
Germany (C Zerna)
perfusion or multiphase CT angiogram), occlusion Atrial fibrillation 78 (17%) 91 (21%)
Correspondence to:
location (large vessel occlusion [internal carotid artery or Ischaemic heart disease 73 (16%) 69 (16%) Prof Shelagh Coutts, Department
middle cerebral artery (MCA)-M1] vs medium vessel Congestive heart failure 18 (4%) 16 (4%) of Clinical Neurosciences,
occlusion [MCA-M2 or distal, anterior cerebral artery or Chronic renal failure 17 (4%) 22 (5%) University of Calgary, Calgary,
AB T2N 2T9, Canada
distal] vs vertebrobasilar [includes posterior cerebral Peripheral vascular disease 15 (3%) 13 (3%) scoutts@ucalgary.ca
artery]), recanalisation,28 and baseline NIHSS score before Past intracranial haemorrhage 1 (<1%) 3 (1%)
See Online for appendix
randomisation. Analyses were completed using STATA Clinical presentation
(version 18). The trial is registered at ClinicalTrials.gov, NIHSS score at baseline 2 (1–3) 2 (1–3)
NCT02398656, and is closed to accrual. Haemoglobin, g/L 141 (131–152) 140 (129–150)
Glucose, mM 6 (6–7) 6 (6–7)
Role of the funding source Creatinine, µM 84 (70–97) 82 (70–98)
The funders of the study had no role in study design, ASPECTS baseline 10 (9–10) 10 (9–10)
data collection, data analysis, data interpretation, or Onset to randomisation time, 273 (162–448) 286 (161–440)
writing of the report. min
Onset to hospital arrival time, 151 (72–337) 148 (76–332)
Results min
Between April 27, 2015, and Jan 19, 2024, 886 patients Onset to treatment time, min 311 (184–495) 293 (165–453)
were enrolled at 48 sites (appendix pp 8–10); Occlusion location at baseline
369 (42%) were female and 516 (58%) were male at Large vessel occlusion* 50 (11%) 53 (12%)
birth. The trial’s enrolment was ended by the Steering Medium vessel occlusion† 245 (54%) 235 (55%)
Committee after a planned interim analysis resulted in Vertebrobasilar circulation‡ 25 (6%) 20 (5%)
the DSMC recommending that the trial be halted for Focal perfusion lesion 127 (28%) 118 (27%)
futility. At the time of the interim analysis, the No occlusion detected 3 (1%) 5 (1%)
conditional power to show an effect favouring Data are n (%) or median (IQR). Race and ethnicity was self reported; ethnicity was
tenecteplase, assuming the outcomes rates remained binary with Hispanic or non-Hispanic being the options. ASPECTS=Alberta Stroke
the same for future patients as for currently observed, Program Early CT score. ITT=intention to treat. NIHSS=National Institutes of
Health Stroke Scale score. *Intracranial internal carotid artery, M1 segment of the
was less than 1%. Two (<1%) patients withdrew consent,
middle cerebral artery. †M2 segment of the middle cerebral artery or distal,
leaving 884 patients in the ITT population. Of A2 segment of the anterior cerebral artery or distal. ‡Intracranial vertebral artery,
886 patients, 432 (49%) were assigned to tenecteplase basilar artery or branches, posterior cerebral artery.
and 454 (51%) to control (figure 1). Four patients had
Table 1: Baseline characteristics (ITT population)
missing mRS outcomes at 90 days, two (<1%) patients
www.thelancet.com Vol 403 June 15, 2024 2601
Articles
were lost to follow-up, and two withdrew consent. for the control group. Recanalisation improved
There were no missing baseline data. outcomes (appendix p 17).
Baseline demographic and clinical characteristics of In safety analysis, more symptomatic intracranial
patients were similar between the tenecteplase group haemorrhages occurred in the tenecteplase group (eight
and the control group (table 1). The control medication [2%]) versus control (two [<1%], RR 4·2, 95% CI 0·9–19·6;
was given at a median of 17 min later than tenecteplase. table 3, appendix p 18). Four symptomatic intracranial
Median baseline NIHSS was 2 (IQR 1–3) overall haemorrhages occurred in the 0–4·5 h window and six in
(appendix p 11) and 149 (17%) of 884 participants reported the 4·5–12 h window (p=0·75). 34 patients received a dose
complete symptom resolution at the time of of tenecteplase greater than 25 mg, one of whom had a
randomisation. Median onset to randomisation was symptomatic intracranial haemorrhage. No extracranial
4·6 h (IQR 2∙7–7∙5). Most patients in the control group haemorrhages were temporally related to treatment. There
were treated with dual antiplatelet therapy with aspirin were 20 deaths in the tenecteplase group and five deaths in
and clopidogrel (259 [57%] of 452) or aspirin monotherapy the control group (adjusted hazard ratio 3·8; 95% CI
(106 [23%] of 452). The control population treatments are 1·4–10·2; table 2). Seven deaths (one in the control group
shown in the appendix (p 13). and six in the tenecteplase group) were related to a
After a median follow-up time of 92 days (IQR 85–99), symptomatic intracranial haemorrhage. Other than the
the primary outcome (mRS responder analysis) deaths after symptomatic intracranial haemorrhage, most
occurred in 338 (75%) of 452 patients in the control deaths occurred well after treatment and were not judged to
group and 309 (72%) of 432 in the tenecteplase group be biologically related to tenecteplase (appendix pp 15–16).
(risk ratio [RR] 0·96, 95% CI 0·88–1·04). Secondary In the subgroup analyses, female patients were more
outcomes are shown in table 2 and in the likely to do better with control than their male counterparts
appendix (pp 14, 15). More patients had an NIHSS of 0 in whom there was no treatment effect (pinteraction=0·04) and
in the tenecteplase group versus control (247 [57%] of patients older than 80 years were also more likely to do
432 vs 226 [50%] of 452, RR 1·16; 95% CI 1·02–1·31). In better with control as compared with younger patients in
the subset of patients who had direct evidence of whom there was no treatment effect (pinteraction=0·04). No
occlusion and underwent CT angiogram at 4–8 h heterogeneity of treatment effect was observed across any
(515 [58%] of 884), recanalisation rates overall were other subgroups (figure 2, appendix p 12).
higher in the tenecteplase-treated patients than in the
control group (122 [48%] of 256 vs 56 [22%] of 259, Discussion
p<0·0001; appendix p 13). For patients with large vessel Among patients with minor stroke symptoms
occlusion, recanalisation rates were 48% (22 of 46) in (NIHSS 0–5) and intracranial occlusion presenting
the tenecteplase group and 13% (five of 40; p=0·0005) within 12 h from symptom onset, we found no benefit for
Control (n=452) Tenecteplase Risk difference Unadjusted RR or HR Adjusted RR, RD, or
(n=432) (95% CI) (95% CI) HR (95% CI)*
Primary outcome
Responder 338 (75%) 309 (72%) –3·3% (–9·1 to 2·6) RR 0·96 (0·88 to 1·04) RR 0·96 (0·89 to 1·04)
Secondary outcome
mRS 0–1 at 90 days 321 (71%) 298 (69%) –2·4% (–8·4 to 3·7) RR 0·97 (0·89 to 1·05) RR 0·97 (0·90 to 1·06)
mRS 0–2 at 90 days 391 (87%) 352 (81%) –5·4% (–0·10 to –0·01) RR 0·94 (0·89 to 0·99) RR 0·94 (0·89 to 1·00)
NIHSS of 0 at 5 days or discharge 226 (50%) 247 (58%)† 7·8% (1·3 to 14·4) RR 1·16 (1·02 to 1·31) RR 1·15 (1·03 to 1·30)
mRS return to pre-morbid function 222 (49%) 212 (49%) 0 (–6·6 to 6·5) RR 1·00 (0·87 to 1·14) RR 1·00 (0·88 to 1·15)
Mean mRS score at 90 days 1·11 1·27 0·16 (–0·03 to 0·34) ∙∙ 0·13‡ (–0·05 to 0·31)
Median (IQR) mRS score at 90 days 1 (0–2) 1 (0–2) ∙∙ ∙∙ ∙∙
Lawton IADL percent functioning 90·8 86·4 –4·5 (–7∙9 to –1·1) ∙∙ RR –4·0 (–7·3 to –0·7)
score (n=850)
EQ-5D-5L index score (n=854; 0·84 0·81 –0·03 (–0·07 to –0·001) ∙∙ RR –0·03
range 0 to 1) (–0·06 to –0·001)
EQ-5D-5L VAS score (n=839; range 0 0·76 0·73 –3·4 (–6·3 to –0·5) ∙∙ RR –3·2 (–6·1 to –0·3)
to 100)
Death at 90 days 5 (1%) 20 (5%) ∙∙ HR 3·9 (1·4 to 10·4) HR 3·8 (1·4 to 10·2)
Data are n (%), unless otherwise indicated. EQ-5D-5L=European Quality of Life score, five dimensions, five levels. HR=hazard ratio. ITT=intention to treat. mRS=modified
Rankin Scale. NIHSS=National Institutes of Health Stroke Scale score. Lawton IADL=Lawton–Brody Instrumental Activities of Daily Living Scale index. RD=risk difference.
RR=risk ratio. VAS=visual analogue scale. *Adjusted for age, sex at birth, baseline NIHSS score, and onset to randomisation time; data violate the proportional odds
assumptions and so an ordinal shift analysis is not presented. †There were 427 participants with available data. ‡Adjusted difference of means.
Table 2: Outcomes (ITT population)
2602 www.thelancet.com Vol 403 June 15, 2024
Articles
the prevention of disability after treatment with
Control Tenecteplase p value
0·25 mg/kg of tenecteplase as compared with non- (n=452) (n=432)
thrombolytic standard of care. There was a small
Serious adverse event 80 (18%) 100 (23%) 0·045
increased risk of symptomatic haemorrhage in patients
Stroke progression 33 (7%) 35 (8%) 0·71
treated with tenecteplase and more deaths at 90 days in
Stroke recurrence 15 (3%) 16 (4%) 0·86
the tenecteplase group as compared with the control
Symptomatic intracranial haemorrhage 2 (<1%) 8 (2%) 0·059
group.
Death after symptomatic intracranial 1 (<1%) 6 (1%) 1
Over the past decade, endovascular thrombectomy has haemorrhage within 90 days
become the standard of care for stroke due to large vessel Any haemorrhage on follow-up imaging 40 (9%) 62 (14%) 0·02
occlusion. As a result, to define the angiographic
Rescue endovascular thrombectomy for 10 (2%) 15 (3%) 0·31
occlusions, CT angiography of the circle of Willis and index stroke
neck has become routinely used in addition to non- Death within 5 days 1 (<1%) 8 (2%) 0·018
contrast CT brain for all patients with suspected Death at 90 days 5 (1%) 20 (5%) 0·0018
ischaemic stroke, including those with milder deficits. Aspiration pneumonia 2 (<1%) 6 (1%) 0·17
With increased imaging, this approach has meant that Atrial fibrillation 3 (1%) 4 (1%) 0·72
many patients who present with relatively minor deficits Congestive heart failure 1 (<1%) 5 (1%) 0·12
are now identified to have evidence of an intracranial Seizure 3 (1%) 3 (1%) 1
occlusion. Based upon prior work, the fundamental Urinary tract infection 4 (1%) 2 (<1%) 0·69
premise of TEMPO-2 was that presence of an intracranial
ITT=intention to treat.
occlusion defines the minor stroke population with the
highest risk of poor outcome and that reperfusion in Table 3: Safety events (ITT population)
these patients would be beneficial.
Although there were significantly more patients with Risk ratio (95% CI) N pinteraction
early recanalisation and an NIHSS score of 0 at day 5 or
discharge after tenecteplase treatment, this did not Age (years) 0·04
translate into improved functional outcomes at 90 days. ≤80 1·01 (0·93–1·10) 676
High recanalisation rates are concordant with a recently >80 0·80 (0·64–0·99) 238
published meta-analysis that shows higher recanalisation Sex at birth 0·04
rates with tenecteplase compared with alteplase.29 All Female 0·87 (0·76–1·00) 368
other secondary outcomes did not show any benefit for Male 1·03 (0·94–1·13) 516
Onset to treatment (h) 0·102
tenecteplase. There was a signal of an increased rate of
≤4·5 0·91 (0·81–1·02) 432
symptomatic intracranial haemorrhage in the
>4·5 1·02 (0·92–1·15) 452
tenecteplase group, but at the relatively low absolute rate
Symptoms 0·71
of 2%, which is lower than the 3% rate seen in the Resolved 0·94 (0·82–1·08) 149
tenecteplase group of the AcT study. The PRISMS study9 Ongoing 0·97 (0·88–1·06) 735
found that there was a low but increased risk of Occlusion 0·39
symptomatic haemorrhage (3%) in minor stroke patients Large vessel occlusion* 0·98 (0·77–1·25) 103
treated with thrombolysis using intravenous alteplase. Medium vessel occlusion† 0·94 (0·84–1·05) 480
Like the PRISMS study, the low rate of harm from Vertebrobasilar occlusion‡ 0·86 (0·59–1·24) 45
symptomatic haemorrhage in TEMPO-2 was not Focal perfusion lesion 1·02 (0·89–1·17) 245
counteracted by a significant improvement in functional NIHSS score at baseline 0·07
outcomes at 90 days. The symptomatic haemorrhage rate 0 0·95 (0·83–1·09) 142
does not fully account for the absence of benefit at 1 1·13 (0·95–1·34) 206
2 1·03 (0·89–1·20) 199
90 days with tenecteplase. Similar to other trials17,18 we
3 0·77 (0·63–0·96) 155
allowed patients to be enrolled out to 12 h from symptom
4 0·93 (0·74–1·15) 122
onset. We did not see any increase in the symptomatic
5 0·70 (0·41–1·20) 60
intracranial haemorrhage rate in patients treated after
4·5 h versus before 4·5 h. The subgroup of patients 0·6 0·8 1·0 1·2
treated at 4·5–12∙0 h showed weak evidence of better
Favours control Favours tenecteplase
outcomes with thrombolysis as compared with those
treated before 4·5 h. This suggests that the 12 h window Figure 2: Forest plot of effect size by subgroup
for TEMPO-2 did not explain the absence of benefit seen Adjusted for sex at birth, age, time from onset and baseline NIHSS. NIHSS=National Institutes of Health Stroke
Scale. *Intracranial internal carotid and M1 segment of the middle cerebral artery. †M2 segment of the middle
from tenecteplase. cerebral artery or distal, A2 segment of the anterior cerebral artery or distal. ‡Including all branches of the posterior
Patients in the non-thrombolytic control group of the cerebral artery.
TEMPO-2 study did better than expected. This might be
the result of chance, patient selection, greater penetrance
of dual antiplatelet therapy in the standard-of-care group,
www.thelancet.com Vol 403 June 15, 2024 2603
Articles
or better overall stroke care. The recanalisation rate in the data in a parallel registry, guideline-based practice is to
control group was 22% overall in the study and in large offer thrombolysis to patients who have disabling
vessel occlusion it was 13% in the non-thrombolytic symptoms in the judgement of the treating physician and
control group, highlighting that antiplatelet treatment is patient, and therefore we predict, but do not have data to
still an active treatment. Despite the reported high support, that a majority of patients in the TEMPO-2 trial
recanalisation rates in the tenecteplase group (48%), there did not have disabling symptoms at the time of consent to
was no change in the rate of stroke progression between the study. Because of the long duration of the study, there
groups, with an 8% rate of progression seen overall in the is the potential for selection bias in study inclusion and the
study. We know from previous work that patients with possibility that secular changes in care affected outcomes.
minor stroke and with intracranial occlusion are at risk of In summary, we did not find any evidence of benefit in
both progression and disability.23 It could be that medical treating minor stroke patients with intracranial occlusion
care (eg, intravenous fluids and antiplatelet therapy) in with tenecteplase as compared with non-thrombolytic
this patient population reduced the rate of stroke control.
progression in both groups. A rate of recanalisation of Contributors
48% might simply not be high enough to influence stroke SBC and MDH prepared the first draft of the report. SBC, CK, and MDH
progression and outcomes. Most of these patients are conceptualised the study design. SBC and MDH wrote the statistical
analysis plan. MDH was the lead statistician with SBC, and CK providing
likely to have excellent collaterals and therefore good additional data management and statistical support, and all had access to
supportive care may have improved outcomes in both all the data. SBC, CK, NSi, and MDH had access to and verified the
groups. It is also possible that the neurological deficit is underlying study data. MH led the imaging core laboratory with ZA, MG,
so minimal that vessel recanalisation cannot make SBC, and BKM providing support. SBC and MDH participated in data
analysis and interpretation. All authors participated in patient enrolment,
patients detectably much better using the outcome trial execution and management, and critically reviewed the report and
assessments we currently use. Consistent with the low approved the final version before submission. All authors had full access
rate of stroke progression, rescue endovascular to all the data in the study and had final responsibility for the decision to
thrombectomy rates were low in both treatment groups submit for publication.
in the study. Studies examining the use of endovascular Declaration of interests
thrombectomy in the subset of patients with minor stroke SBC received grant funding from the Canadian Institutes of Health
Research (CIHR), Heart and Stroke Foundation of Canada (HSFC), and
and large vessel occlusion in trials such as the ENDOLOW the British Heart Foundation (BHF) to complete the TEMPO-2 study.
trial (NCT04167527) are ongoing. Boehringer Ingelheim provided off-the-shelf study drug (tenecteplase) for
Overall mortality was low with 25 (3%) deaths but the study. JFA has received public research grants from the Spanish
mortality was higher in the tenecteplase group. Most of Ministry of Science, the regional health department, the European
Commission, and a private research grant from AstraZeneca. He has
these deaths occurred late and were not temporally received consultant or speaker fees from Pfizer-BMS, Medtronic, and
related to study drug, with seven of 25 deaths associated Amgen, and travel support from Daiichi-Sankyo. KSB reports speaker
with a symptomatic intracranial haemorrhage (six in the fees from Boehringer Ingelheim and AstraZeneca. LC has received
consulting or speakers fees from Roche. JF reports speaker fees from
tenecteplase group and one in the control group). The
AstraZeneca, Bayer, BMS, Boehringer Ingelheim, Pfizer, Sankyo, and
rates of stroke progression, stroke recurrence, and rescue Daiichi. AG reports a grant from Microvention; speaker fees from
endovascular thrombectomy were similar between Alexion, Biogen, and Servier Canada; and stock options for SnapDx and
groups. The increase in late deaths is unexplained and Collavidence. DG reports honoraria from Boehringer Ingelheim, Ipsen,
and Eisai. MG reports grant funding from Medtronic and Cerenovus and
has not been seen in previous studies. Because of the low
consulting fees from Mentice, CSL Behring, MicroVention, and
absolute numbers, this could be a chance finding. Medtronic. TSF participated in an advisory board for Roche. FL reports
Strengths of this study were that it was a large, well speaker fees and travel support from Boehringer Ingelheim. BKM has
conducted, investigator-initiated, international, multi been paid honoraria from Boehringer Ingelheim and Roche. MM has
received honoraria from Boehringer Ingelheim for participation at an
centre, randomised trial with near complete follow-up.
advisory board on the approval of tenecteplase for treatment of acute
Limitations were that the study took nearly 9 years to ischaemic stroke. SOM has received speaker fees from Boehringer,
complete due to external factors including a global Medtronic, Penumbra, Bayer, Pfizer, Novartis, Novo Nordisk, Servier, and
pandemic and drug supply issues. Although patients were Daiichi Sankyo. KWM reports grant funding from the BHF, and the
Stroke Association; consultancy fees from Boehringer Ingelheim,
eligible to be enrolled on the basis of a focal perfusion Biogen, IschaemaView; lecture fees from Boehringer Ingelheim,
lesion on CT imaging, reflecting real-world practice, it is IschaemaView, and Brainomix; and non-financial support (drug supply
possible that these lesions are qualitatively different from for ATTEST-2 trial) from Boehringer Ingelheim. MWP is on Boehringer
those with an observable arterial occlusion. However, we Ingelheim Advisory Board for Metalyse in stroke. AP received speaker
fees from Boehringer Ingelheim and travel support from AstraZeneca for
did not see any treatment interaction based on overt attending a meeting. OMP-N has received speaker fees from Boehringer
evidence of an occlusion versus a focal perfusion lesion, Ingelheim and AstraZeneca. RS is part funded by the UCLH Biomedical
suggesting that this was not the reason for the absence of Research Centre. DS reports an unrestricted educational grant from
benefit with tenecteplase. Patients in the non-thrombolytic Boehringer Ingelheim. MIW reports sponsorship or financial assistance
to support attendance at scientific meetings from Boehringer Ingelheim,
control group principally received antiplatelet therapy, but Bristol Myers Squibb, Daiichi Sankyo UK, and Bayer; honoraria for
treatment was not one single comparator. This pragmatic lectures given at education meetings from Boehringer Ingelheim, Bristol
choice reflects clinical practice and might make the trial Myers Squibb, and AstraZeneca; and payment for participation in
results more generalisable. Although we did not collect advisory panels from Boehringer Ingelheim and Daiichi Sankyo UK.
2604 www.thelancet.com Vol 403 June 15, 2024
Articles
DJW is the Co-principal Investigator for Health Research Board of 13 Wang Y, Li S, Pan Y, et al. Tenecteplase versus alteplase in acute
Ireland, Award–Improving Pathways for Acute Stroke and Rehabilitation. ischaemic cerebrovascular events (TRACE-2): a phase 3,
AYXY reports salary support from the HSFC. MDH reports grant multicentre, open-label, randomised controlled, non-inferiority
funding from CIHR, HSFC, Alberta Innovates, and study drug from trial. Lancet 2023; 401: 645–54.
Boehringer Ingelheim; grants from NoNo and Medtronic; consulting fees 14 Alamowitch S, Turc G, Palaiodimou L, et al. European Stroke
from Sun Pharma Brainsgate; and a DSMB member role on many stroke Organisation (ESO) expedited recommendation on tenecteplase for
clinical trials. acute ischaemic stroke. Eur Stroke J 2023; 8: 8–54.
15 Heran M, Lindsay P, Gubitz G, et al. Canadian stroke best practice
Data sharing recommendations: acute stroke management, 7th edition practice
Data collected for the study, including de-identified individual guidelines update, 2022. Can J Neurol Sci 2024; 51: 1–31.
participant data and a data dictionary defining each field in the set, can 16 Stroke Foundation. Australian and New Zealand living clinical
be made available to others on reasonable request and after signing guidelines for stroke management. Chapter 3 of 8: acute medical
appropriate data sharing agreements. Please send data access requests to and surgical management. 2023. https://files.magicapp.org/
scoutts@ucalgary.ca. Such requests must be approved by all the guideline/c1775.579.6513-49cb-b3df-7aab7780837e/published_
respective ethics boards and appropriate data custodians. guideline_7233-10_7.pdf.
17 Albers GW, Jumaa M, Purdon B, et al. Tenecteplase for stroke at
Acknowledgments 4·5 to 24 hours with perfusion-imaging selection. N Engl J Med
This trial was funded by grants from the HSFC, CIHR, and the BHF. 2024; 390: 701–11.
Intravenous tenecteplase was standard off-the-shelf drug and was paid 18 Roaldsen MB, Eltoft A, Wilsgaard T, et al. Safety and efficacy of
for by Boehringer Ingelheim, who had no role in the trial design or tenecteplase in patients with wake-up stroke assessed by non-
conduct, data analysis, or manuscript preparation. contrast CT (TWIST): a multicentre, open-label, randomised
controlled trial. Lancet Neurol 2023; 22: 117–26.
References
1 Reeves M, Khoury J, Alwell K, et al. Distribution of National 19 Coutts SB, Dubuc V, Mandzia J, et al. Tenecteplase-tissue-type
Institutes of Health stroke scale in the Cincinnati/northern plasminogen activator evaluation for minor ischemic stroke with
Kentucky stroke study. Stroke 2013; 44: 3211–13. proven occlusion. Stroke 2015; 46: 769–74.
2 Smith EE, Fonarow GC, Reeves MJ, et al. Outcomes in mild or 20 Singh N, Kenney C, Butcher KS, et al. A randomized controlled trial
rapidly improving stroke not treated with intravenous recombinant of tenecteplase versus standard of care for minor ischemic stroke
tissue-type plasminogen activator: findings from Get With The with proven occlusion (TEMPO-2): rational and design of a
Guidelines–Stroke. Stroke 2011; 42: 3110–15. multicenter, randomized open-label clinical trial. Int J Stroke 2024;
published online April 27. https://doi.org/10.1177/17474930241253702.
3 Barber PA, Zhang J, Demchuk AM, Hill MD, Buchan AM. Why are
stroke patients excluded from TPA therapy? An analysis of patient 21 Barber PA, Demchuk AM, Zhang J, Buchan AM. Validity and
eligibility. Neurology 2001; 56: 1015–20. reliability of a quantitative computed tomography score in
predicting outcome of hyperacute stroke before thrombolytic
4 Nedeltchev K, Schwegler B, Haefeli T, et al. Outcome of stroke with
therapy. ASPECTS Study Group. Alberta Stroke Programme Early
mild or rapidly improving symptoms. Stroke 2007; 38: 2531–35.
CT Score. Lancet 2000; 355: 1670–74.
5 Coutts SB, Modi J, Patel SK, Demchuk AM, Goyal M, Hill MD.
22 Zhao W, Hill MD, Palesch Y. Minimal sufficient balance-a new
CT/CT angiography and MRI findings predict recurrent stroke after
strategy to balance baseline covariates and preserve randomness of
transient ischemic attack and minor stroke: results of the
treatment allocation. Stat Methods Med Res 2015; 24: 989–1002.
prospective CATCH study. Stroke 2012; 43: 1013–17.
23 Coutts SB, Modi J, Patel SK, et al. What causes disability after
6 Kim JT, Park MS, Chang J, Lee JS, Choi KH, Cho KH. Proximal
transient ischemic attack and minor stroke? Results from the CT
arterial occlusion in acute ischemic stroke with low NIHSS scores
and MRI in the triage of TIA and minor cerebrovascular events to
should not be considered as mild stroke. PLoS One 2013; 8: e70996.
identify high risk patients (CATCH) Study. Stroke 2012;
7 Horton M, Modi J, Patel SK, et al. Refinement of imaging predictors 43: 3018–22.
of recurrent events following transient ischemic attack and minor
24 Sato S, Uehara T, Ohara T, Suzuki R, Toyoda K, Minematsu K.
stroke. PLoS One 2013; 8: e65752.
Factors associated with unfavorable outcome in minor ischemic
8 Emberson J, Lees KR, Lyden P, et al. Effect of treatment delay, age, stroke. Neurology 2014; 83: 174–81.
and stroke severity on the effects of intravenous thrombolysis with
25 von Kummer R, Broderick JP, Campbell BC, et al. The Heidelberg
alteplase for acute ischaemic stroke: a meta-analysis of individual
bleeding classification: classification of bleeding events after
patient data from randomised trials. Lancet 2014; 384: 1929–35.
ischemic stroke and reperfusion therapy. Stroke 2015; 46: 2981–86.
9 Khatri P, Kleindorfer DO, Devlin T, et al. Effect of alteplase vs
26 Bruno A, Akinwuntan AE, Lin C, et al. Simplified modified Rankin
aspirin on functional outcome for patients with acute ischemic
Scale questionnaire: reproducibility over the telephone and
stroke and minor nondisabling neurologic deficits: the PRISMS
validation with quality of life. Stroke 2011; 42: 2276–79.
randomized clinical trial. JAMA 2018; 320: 156–66.
27 Dorman PJ, Waddell F, Slattery J, Dennis M, Sandercock P. Is the
10 Chen HS, Cui Y, Zhou ZH, et al. Dual antiplatelet therapy vs
EuroQol a valid measure of health-related quality of life after
alteplase for patients with minor nondisabling acute ischemic stroke:
stroke? Stroke 1997; 28: 1876–82.
the ARAMIS randomized clinical trial. JAMA 2023; 329: 2135–44.
28 Menon BK, Al-Ajlan FS, Najm M, et al. Association of clinical,
11 Singh N, Menon BK, Dmytriw AA, Regenhardt RW, Hirsch JA,
imaging, and thrombus characteristics with recanalization of visible
Ganesh A. Replacing alteplase with tenecteplase: is the time ripe?
intracranial occlusion in patients with acute ischemic stroke. JAMA
J Stroke 2023; 25: 72–80.
2018; 320: 1017–26.
12 Menon BK, Buck BH, Singh N, et al. Intravenous tenecteplase
29 Katsanos AH, Safouris A, Sarraj A, et al. Intravenous thrombolysis
compared with alteplase for acute ischaemic stroke in Canada
with tenecteplase in patients with large vessel occlusions:
(AcT): a pragmatic, multicentre, open-label, registry-linked,
systematic review and meta-analysis. Stroke 2021; 52: 308–12.
randomised, controlled, non-inferiority trial. Lancet 2022;
400: 161–69.
www.thelancet.com Vol 403 June 15, 2024 2605
You might also like
- MR Clean Late LancetDocument10 pagesMR Clean Late LancetLetícia JanuziNo ratings yet
- Clinical-Psychomotor SkillsDocument415 pagesClinical-Psychomotor SkillsKimG1991100% (2)
- Quick Guide To Cardiopulmonary Care 4th EditionDocument185 pagesQuick Guide To Cardiopulmonary Care 4th EditionLorenzo Romero AlbarranNo ratings yet
- 2024 NATO ACF Cardio_Haem_Paeds Dataset R2Document9 pages2024 NATO ACF Cardio_Haem_Paeds Dataset R2barbaraNo ratings yet
- Intravenous Tenecteplase Compared With Alteplase For Acute IschaemicDocument9 pagesIntravenous Tenecteplase Compared With Alteplase For Acute IschaemicVictoria JacoboNo ratings yet
- 7.17Document10 pages7.17Lê Đình NhiênNo ratings yet
- Tenecteplasa Vs AlteplasaDocument9 pagesTenecteplasa Vs AlteplasaJefferson Duque MartinezNo ratings yet
- Flaherty 2016Document6 pagesFlaherty 2016Diornald MogiNo ratings yet
- Lancet ArticolDocument10 pagesLancet ArticolStefan TehanciucNo ratings yet
- Eficacia de La Telemedicina en El Manejo de La Insuficiencia CardíacaDocument11 pagesEficacia de La Telemedicina en El Manejo de La Insuficiencia CardíacaSMIBA MedicinaNo ratings yet
- Ficha 4Document12 pagesFicha 4mariaNo ratings yet
- Hanley 2017Document9 pagesHanley 2017sjulurisNo ratings yet
- Kim 2015Document9 pagesKim 2015Ke XuNo ratings yet
- Manage TrialDocument10 pagesManage Trialgareth.goldNo ratings yet
- Pacific StrokeDocument11 pagesPacific StrokemrabhilekhNo ratings yet
- Clinical Course of Untreated Cerebral Cavernous MalformationsDocument8 pagesClinical Course of Untreated Cerebral Cavernous MalformationsMalaspulgasNo ratings yet
- Elective Versus Therapeutic Neck Dissection in Node-Negative Oral Cancer PDFDocument9 pagesElective Versus Therapeutic Neck Dissection in Node-Negative Oral Cancer PDFluxmansrikanthaNo ratings yet
- Craniectomia DescompresivaDocument51 pagesCraniectomia DescompresivaVlady78No ratings yet
- CD DX, LancetDocument29 pagesCD DX, Lancetimran karimNo ratings yet
- Pi Is 0140673623008061Document14 pagesPi Is 0140673623008061Edward ElBuenoNo ratings yet
- Me Hanna 2016Document11 pagesMe Hanna 2016eswarNo ratings yet
- MISTIEDocument10 pagesMISTIEsjulurisNo ratings yet
- Classifi Cation of Treatment-Related Mortality in Children WithDocument7 pagesClassifi Cation of Treatment-Related Mortality in Children WithIgnatia Rosalia KiranaNo ratings yet
- 8 28 PDFDocument8 pages8 28 PDFfirmansyahddsNo ratings yet
- Articles: BackgroundDocument8 pagesArticles: BackgroundfirmansyahddsNo ratings yet
- Tugas RCT SenaDocument10 pagesTugas RCT SenaArfad El HabibieNo ratings yet
- Seminario 4 PDFDocument12 pagesSeminario 4 PDFCarolina DiazNo ratings yet
- Invasive Versus Non-Invasive Management of Older Patients With non-ST Elevation Myocardial Infarction (SENIOR-NSTEMI) : A Cohort Study Based On Routine Clinical DataDocument12 pagesInvasive Versus Non-Invasive Management of Older Patients With non-ST Elevation Myocardial Infarction (SENIOR-NSTEMI) : A Cohort Study Based On Routine Clinical DatasavitageraNo ratings yet
- Ooi 160066Document6 pagesOoi 160066bjro1986No ratings yet
- Study After 80Document9 pagesStudy After 80Oscar Leonardo Torra BarajasNo ratings yet
- Articles: BackgroundDocument8 pagesArticles: BackgroundrodribeatsNo ratings yet
- Off MedDocument8 pagesOff MedShimily LiangNo ratings yet
- PIIS2213858721002357Document29 pagesPIIS2213858721002357Bladimir CentenoNo ratings yet
- Articles: BackgroundDocument11 pagesArticles: BackgroundricardojosesotofontalvoNo ratings yet
- C19 Useless AntiviralDocument13 pagesC19 Useless Antiviral2jbkrf5bkcNo ratings yet
- Davis 2008Document11 pagesDavis 2008Suchada SangpetchNo ratings yet
- Jamaneurology Jiang 2018 Oi 180048Document9 pagesJamaneurology Jiang 2018 Oi 180048jonas lopetNo ratings yet
- Acute Stroke With Large Ischemic Core TreatedDocument8 pagesAcute Stroke With Large Ischemic Core Treatedjasonongsp1992No ratings yet
- Brain Cancer Progression A Retrospective.7Document9 pagesBrain Cancer Progression A Retrospective.7Hamzeh AlsalhiNo ratings yet
- Oxford CovidDocument13 pagesOxford Covid1954zapaNo ratings yet
- Destiny IIDocument10 pagesDestiny IIÍtala MotaNo ratings yet
- PONCHO TrialDocument8 pagesPONCHO Trialrahul krishnanNo ratings yet
- Arbel 2018Document29 pagesArbel 2018Sam ExlerNo ratings yet
- ATTENTION TrialDocument12 pagesATTENTION TrialmrabhilekhNo ratings yet
- Impact of Antiplatelet Therapy During Endovascular Therapy For Tandem OcclusionsDocument8 pagesImpact of Antiplatelet Therapy During Endovascular Therapy For Tandem Occlusionsrifki irsyadNo ratings yet
- 2020 Terri Glioma PRODocument7 pages2020 Terri Glioma PRORimpa Basu AchariNo ratings yet
- Articles: BackgroundDocument15 pagesArticles: Backgroundvinadata01No ratings yet
- Balanced Crystalloids Versus Saline For Critically Ill Patients (BEST-Living)Document10 pagesBalanced Crystalloids Versus Saline For Critically Ill Patients (BEST-Living)vali.levo7No ratings yet
- Steroid Vs Splint in CtsDocument11 pagesSteroid Vs Splint in CtsDiayanti TentiNo ratings yet
- Articles: BackgroundDocument10 pagesArticles: BackgroundPedro BarlettaNo ratings yet
- Articulo Suplementos en Pacientes Contacto TBDocument16 pagesArticulo Suplementos en Pacientes Contacto TBstephanie bojorquezNo ratings yet
- Characteristics of Chinese Herbal Medicine Usage and Its Effect On Survival ofDocument9 pagesCharacteristics of Chinese Herbal Medicine Usage and Its Effect On Survival ofu106023406No ratings yet
- Milrinone As Compared With Dobutamine in The Treatment of Cardiogenic ShockDocument10 pagesMilrinone As Compared With Dobutamine in The Treatment of Cardiogenic ShockCarlos Alberto Holguin PalaciosNo ratings yet
- Treatment of Benign Tracheal Stenosis Using Endoluminal Spray CryotherapyDocument6 pagesTreatment of Benign Tracheal Stenosis Using Endoluminal Spray CryotherapyVania Dwi AndhaniNo ratings yet
- PIIS2213260023004186Document11 pagesPIIS2213260023004186teresa mendozaNo ratings yet
- Tred HFDocument13 pagesTred HFhairos.izhaNo ratings yet
- Treatment For Benign Thyroid Nodules With A CombinDocument7 pagesTreatment For Benign Thyroid Nodules With A CombindarthjesussithNo ratings yet
- New England Journal Medicine: The ofDocument10 pagesNew England Journal Medicine: The ofNatalia ArizaNo ratings yet
- Hemicolectomy Versus Appendectomy For Patients With Appendiceal Neuroendocrine Tumours 1-2 CM in Size, A Retrospective, Europe-Wide, Pooled Cohort Study.2023.Document8 pagesHemicolectomy Versus Appendectomy For Patients With Appendiceal Neuroendocrine Tumours 1-2 CM in Size, A Retrospective, Europe-Wide, Pooled Cohort Study.2023.Cirugía General HGRNo ratings yet
- Medicine: Spontaneous Rupture of Solid Pseudopapillary Tumor of PancreasDocument8 pagesMedicine: Spontaneous Rupture of Solid Pseudopapillary Tumor of PancreasPatricia BezneaNo ratings yet
- 2003-Academic Emergency MedicineDocument154 pages2003-Academic Emergency MedicinealiceNo ratings yet
- Innovations in Modern Endocrine SurgeryFrom EverandInnovations in Modern Endocrine SurgeryMichael C. SingerNo ratings yet
- 2021 WEST _ 15500594211008285Document5 pages2021 WEST _ 15500594211008285Vinícius NavesNo ratings yet
- Dehaven on 2021Document8 pagesDehaven on 2021Vinícius NavesNo ratings yet
- s00415-023-11797-wDocument11 pagess00415-023-11797-wVinícius NavesNo ratings yet
- Materials Chemistry B: Journal ofDocument15 pagesMaterials Chemistry B: Journal ofVinícius NavesNo ratings yet
- Gastric Function TestsDocument15 pagesGastric Function TestsMustafa KhandgawiNo ratings yet
- NPCC NewDocument5 pagesNPCC Newyayathee rajuNo ratings yet
- Hubungan Kadar Interleukin 6 Dan Interleukin 10 Serum Pada Pasien Cedera Otak Berat Akibat TraumaDocument9 pagesHubungan Kadar Interleukin 6 Dan Interleukin 10 Serum Pada Pasien Cedera Otak Berat Akibat TraumaanggiNo ratings yet
- Etiology: 1. Compare Lobar Pneumonia With Lobular Pneumonia On The ListDocument3 pagesEtiology: 1. Compare Lobar Pneumonia With Lobular Pneumonia On The Listselam kalayuNo ratings yet
- Improved β-cell Function and Prolonged Remission of Diabetes Type 1 by GLP-1 Agonist Treatment in Newly Diagnosed AdolescencesDocument4 pagesImproved β-cell Function and Prolonged Remission of Diabetes Type 1 by GLP-1 Agonist Treatment in Newly Diagnosed Adolescencesscience world publishingNo ratings yet
- Long Case OrthopaedicDocument24 pagesLong Case OrthopaedicSyimah UmarNo ratings yet
- Ayurvedic Management of SciaticaDocument7 pagesAyurvedic Management of SciaticaSummit GautamNo ratings yet
- 10 Golden Rules in MedicationDocument2 pages10 Golden Rules in MedicationYha Nha Rhu100% (1)
- Balio Ox-580 Brochure enDocument4 pagesBalio Ox-580 Brochure enMo AlyNo ratings yet
- GASTRECTOMYDocument3 pagesGASTRECTOMYMaria Ydela MeradoresNo ratings yet
- Anesthesia-Assisted Vs Buprenorphine - or Clonidine-Assisted Heroin Detoxification and Naltrexone InductionDocument11 pagesAnesthesia-Assisted Vs Buprenorphine - or Clonidine-Assisted Heroin Detoxification and Naltrexone InductionAndy PurnomoNo ratings yet
- Handbook of Pediatric Surgery 2010Document454 pagesHandbook of Pediatric Surgery 2010Clau Jorquera Castillo100% (1)
- Telemanas ProspectusDocument29 pagesTelemanas ProspectusMehbub Hasan ChoudhuryNo ratings yet
- Morning Report: Dr. Dikara WS Maulidy, SP - PDDocument24 pagesMorning Report: Dr. Dikara WS Maulidy, SP - PDBethari Abi SafitriNo ratings yet
- Association Food Allergy Dried Fish Complex Regional Pain SyndromeDocument5 pagesAssociation Food Allergy Dried Fish Complex Regional Pain SyndromeSSR-IIJLS JournalNo ratings yet
- DR. B R Ambedkar Medical Aid SchemeDocument7 pagesDR. B R Ambedkar Medical Aid Schemevineet shendeNo ratings yet
- Dexamethasone (RX) : Dosing & UsesDocument4 pagesDexamethasone (RX) : Dosing & UsesFauzi GanihNo ratings yet
- Clostridium - Botulinum.Document26 pagesClostridium - Botulinum.tummalapalli venkateswara rao100% (1)
- NancyDocument67 pagesNancyNaina BakshiNo ratings yet
- Mcgraw-Hill Companies, IncDocument2 pagesMcgraw-Hill Companies, IncLu LubNaNo ratings yet
- US5877298Document18 pagesUS5877298Venura VishwaNo ratings yet
- 2nd Ed Critical Care Pharmacy Handbook Revised 19th Jan 2021 Final 5.5.21Document186 pages2nd Ed Critical Care Pharmacy Handbook Revised 19th Jan 2021 Final 5.5.21SAUMOJIT MAJUMDERNo ratings yet
- Ceftazidime+Avibactum-2gm +0.5gm InjectionDocument10 pagesCeftazidime+Avibactum-2gm +0.5gm InjectionMd. Abdur RahmanNo ratings yet
- Poc ScoliosisDocument20 pagesPoc ScoliosisSugar Capule - ManuelNo ratings yet
- Breast Cancer Atlas of Clinical OncologyDocument300 pagesBreast Cancer Atlas of Clinical OncologyQueenIchma ChualunaeonelophNo ratings yet
- Scientific Programme BookletDocument44 pagesScientific Programme BookletPreetam PatnalaNo ratings yet
- The Interaction of Herbs and DrugsDocument17 pagesThe Interaction of Herbs and DrugsCarleta StanNo ratings yet
- SepsisDocument8 pagesSepsisLEONELA VALDES CABELLONo ratings yet