Download as pdf or txt
You might also like
- KJMS Vol. 13 No.2 May-Aug 2020 Final BookDocument185 pagesKJMS Vol. 13 No.2 May-Aug 2020 Final Bookhimayatullah100% (1)
- Transfusion in Emergency Room by DR Prannoy George, Department of Emergency Medicine, Amrita Institute of Medical Sciences, Kochi, KeralaDocument41 pagesTransfusion in Emergency Room by DR Prannoy George, Department of Emergency Medicine, Amrita Institute of Medical Sciences, Kochi, KeralaAETCM Emergency medicineNo ratings yet
- AnaemiaDocument27 pagesAnaemiaSamahir F HusseinNo ratings yet
- Blood Conservation StrategiesDocument31 pagesBlood Conservation Strategiesthalida24100% (1)
- Acute Normovolemic Hemodilution: A Practical Approach: Liana Maria Torres de Araújo, Luis Vicente GarciaDocument6 pagesAcute Normovolemic Hemodilution: A Practical Approach: Liana Maria Torres de Araújo, Luis Vicente Garciabaron1992No ratings yet
- Acute Normovolemic HemodilutionDocument13 pagesAcute Normovolemic Hemodilutionali rabieeNo ratings yet
- Use of Blood Products in The Critically Ill - UpToDateDocument13 pagesUse of Blood Products in The Critically Ill - UpToDateOscar F RojasNo ratings yet
- PBM (Autosaved)Document36 pagesPBM (Autosaved)dr AmitNo ratings yet
- Autologus Blood TransfusionDocument20 pagesAutologus Blood TransfusionHarry PatriceNo ratings yet
- Addison K May, MD John P Reilly, MD, Msce Scott Manaker, MD, PHD Arthur J Silvergleid, MD Geraldine Finlay, MD Contributor DisclosuresDocument12 pagesAddison K May, MD John P Reilly, MD, Msce Scott Manaker, MD, PHD Arthur J Silvergleid, MD Geraldine Finlay, MD Contributor DisclosuresAlvaro HaroNo ratings yet
- Blood Management in Massively Bleeding Patients: Adhrie SugiartoDocument35 pagesBlood Management in Massively Bleeding Patients: Adhrie SugiartoJonathan wiradinataNo ratings yet
- Blood TransfusionDocument11 pagesBlood Transfusionsaid tariqNo ratings yet
- 7: Effective Transfusion in Surgery and Critical CareDocument16 pages7: Effective Transfusion in Surgery and Critical CareNick-Hugh Sean WisdomNo ratings yet
- Use of Blood Products in The Critically IllDocument25 pagesUse of Blood Products in The Critically IllAna María Díaz MedinaNo ratings yet
- Transfusion Guidelines HemDocument4 pagesTransfusion Guidelines HemnandhinisankaranNo ratings yet
- Blood ConservationDocument21 pagesBlood ConservationfraolNo ratings yet
- AutotransfusionDocument5 pagesAutotransfusionydtrgnNo ratings yet
- Management of HemorrhageDocument11 pagesManagement of Hemorrhagemerin sunilNo ratings yet
- Complications During HemodialysisDocument2 pagesComplications During HemodialysisHelconJohn100% (1)
- Acute Normovolemic Hemodilution in Cardiac SurgeryDocument9 pagesAcute Normovolemic Hemodilution in Cardiac SurgeryDsm DsmNo ratings yet
- Blood Transfusion in Pediatrics - Dr. RiniDocument55 pagesBlood Transfusion in Pediatrics - Dr. RiniAndyani PratiwiNo ratings yet
- Platelet Transfusion TherapyDocument3 pagesPlatelet Transfusion TherapydrrdchauhanNo ratings yet
- Blood TransfusionDocument31 pagesBlood TransfusionAbdul HafeezNo ratings yet
- 2015 Haemostatic Management of Cardiac Surgical HaemorrhageDocument12 pages2015 Haemostatic Management of Cardiac Surgical HaemorrhageDidier AdodoNo ratings yet
- Heroes of Medicine Bloodless Surgery - Revista TimeDocument11 pagesHeroes of Medicine Bloodless Surgery - Revista Timejorgeduardo9219No ratings yet
- StudyDocument23 pagesStudyK'winetoy Ra'llavNo ratings yet
- Patient Blood Management, Anemia, and Transfusion Optimization Across Surgical SpecialtiesDocument14 pagesPatient Blood Management, Anemia, and Transfusion Optimization Across Surgical SpecialtiesmatheusbbragacNo ratings yet
- Anaemia and Red Blood CellDocument14 pagesAnaemia and Red Blood CelltomreneyoNo ratings yet
- Anesthesia Considerations During Cytoreductive SurDocument9 pagesAnesthesia Considerations During Cytoreductive Surdrardigustian2986No ratings yet
- Perioperative Patient Blood Management To Improve.19Document10 pagesPerioperative Patient Blood Management To Improve.19Reinaldi octaNo ratings yet
- ApheresisDocument3 pagesApheresisaminata6No ratings yet
- Impact of Hemodialysis On Bleeding Tendency in End Stage Renal DiseaseDocument7 pagesImpact of Hemodialysis On Bleeding Tendency in End Stage Renal DiseasedrosabryNo ratings yet
- Bloodcomponenttherap 1Document18 pagesBloodcomponenttherap 1marataningutukuNo ratings yet
- Indications For Blood and Blood Product Transfusion: Review ArticleDocument6 pagesIndications For Blood and Blood Product Transfusion: Review ArticleIzzatul YazidahNo ratings yet
- Ilovepdf Merged 14Document20 pagesIlovepdf Merged 14Qudamah JasemNo ratings yet
- Dietrich 2005Document8 pagesDietrich 2005my accountNo ratings yet
- Anestesi Pada PerdarahanDocument39 pagesAnestesi Pada Perdarahandiklat rsudcibinongNo ratings yet
- BT in Cardiac AnaesthesiaDocument6 pagesBT in Cardiac AnaesthesiaPruthvi RajNo ratings yet
- Blood TransfusionDocument50 pagesBlood TransfusionIsaac Tan Yieng LerNo ratings yet
- Now Get From Our Live Expert On Rea Ltime Basis Join Us and Get Homework HelpDocument24 pagesNow Get From Our Live Expert On Rea Ltime Basis Join Us and Get Homework HelplicservernoidaNo ratings yet
- Estimated Blood Loss in Craniotomy: Diana Sitohang, Rachmawati AM, Mansyur ArifDocument3 pagesEstimated Blood Loss in Craniotomy: Diana Sitohang, Rachmawati AM, Mansyur ArifJihadatul KholilahNo ratings yet
- Share RateDocument26 pagesShare Ratevirtualpop3No ratings yet
- Transfusión IntraoperatoriaDocument24 pagesTransfusión IntraoperatoriaGiovany Salinas100% (1)
- Transfusion of Blood & Blood ProductsDocument18 pagesTransfusion of Blood & Blood ProductsdrlenaaaNo ratings yet
- Blood Conservation StrategiesDocument62 pagesBlood Conservation StrategiesHarika BandaruNo ratings yet
- 4.massive HemorrhageDocument44 pages4.massive HemorrhageyeabsraNo ratings yet
- Blood Transfusion - Indications, Administration and Adverse Reactions PDFDocument9 pagesBlood Transfusion - Indications, Administration and Adverse Reactions PDFStacey WoodsNo ratings yet
- Blood-Ordering For OtolaryngologyDocument5 pagesBlood-Ordering For OtolaryngologyDeba P SarmaNo ratings yet
- Blood Transfusion ICUDocument64 pagesBlood Transfusion ICUSherif ElbadrawyNo ratings yet
- HEMODIALYSIS FinalDocument8 pagesHEMODIALYSIS Finalvineeta.ashoknagarNo ratings yet
- Update On (Approach To) Anemia1 (Changes)Document39 pagesUpdate On (Approach To) Anemia1 (Changes)Balchand KukrejaNo ratings yet
- Management of HemorrhageDocument11 pagesManagement of HemorrhageClara VerlinaNo ratings yet
- Research ArticleDocument10 pagesResearch ArticleAnonymous SbnDyANo ratings yet
- SLED Vs CRRT PDFDocument9 pagesSLED Vs CRRT PDFquilino2012No ratings yet
- Week-176-Allowable-Blood-Loss-REVDocument2 pagesWeek-176-Allowable-Blood-Loss-REVMohammed A SalamaNo ratings yet
- Blood TransfusionsDocument52 pagesBlood TransfusionsZuhri RomiNo ratings yet
- !!NEW DR Lausevic 20200714-003Document4 pages!!NEW DR Lausevic 20200714-003assialnadaweeNo ratings yet
- Blood Transfusion in Hemorrhagic ShockDocument28 pagesBlood Transfusion in Hemorrhagic Shocklas100% (2)
- Massive Transfusion - StatPearls - NCBI BookshelfDocument6 pagesMassive Transfusion - StatPearls - NCBI Bookshelfsadam sodomNo ratings yet
- Laboratory Investigations in Oral and Maxillofacial SurgeryDocument187 pagesLaboratory Investigations in Oral and Maxillofacial SurgeryTarun KashyapNo ratings yet
- Presented By, Dr. Likhit T House Surgeon Medicine D Unit MmcriDocument73 pagesPresented By, Dr. Likhit T House Surgeon Medicine D Unit MmcriVasu LohraNo ratings yet
- 5 - Cardio Batch 2016 AnsweredDocument8 pages5 - Cardio Batch 2016 AnsweredCaroline AgathaNo ratings yet
- Nursing Case Study... 22Document8 pagesNursing Case Study... 22Benjamin KelwonNo ratings yet
- Student Exploration: Circulatory SystemDocument4 pagesStudent Exploration: Circulatory SystemAndreNo ratings yet
- Sick Sinus Syndrome 1Document23 pagesSick Sinus Syndrome 1Salman HabeebNo ratings yet
- 2013q1 Susar Liraglutide PublishedDocument11 pages2013q1 Susar Liraglutide PublishedSofija VukadinovićNo ratings yet
- Pharmacology Final TermDocument19 pagesPharmacology Final TermDWIGHT LESTER O. MANGILANo ratings yet
- What Do We Know About Patent Dustus Arteriosus - Dr. Adhi Teguh, Sp.a (K)Document39 pagesWhat Do We Know About Patent Dustus Arteriosus - Dr. Adhi Teguh, Sp.a (K)laurentiaNo ratings yet
- MSLIF08 Quantitative Immunofluorescence AnalyzerDocument2 pagesMSLIF08 Quantitative Immunofluorescence AnalyzerVictoria AnnaNo ratings yet
- Answer Key Sas SAS 15 1. 2. 3Document11 pagesAnswer Key Sas SAS 15 1. 2. 3Kharlotta RamosNo ratings yet
- Drug Induced Liver DiseaseDocument15 pagesDrug Induced Liver DiseaseMUGHALNo ratings yet
- Sample Test Questions: Krok 2Document29 pagesSample Test Questions: Krok 2Hisham aliNo ratings yet
- Holter MonitorDocument2 pagesHolter MonitorLady RedNo ratings yet
- Rubins-Q A ENDOCRINEDocument14 pagesRubins-Q A ENDOCRINECRUZ Jill EraNo ratings yet
- Unconscious and Comatose Patients DR Moses KazevuDocument17 pagesUnconscious and Comatose Patients DR Moses KazevuMoses Jr KazevuNo ratings yet
- Anti Haemostatic MechanismDocument29 pagesAnti Haemostatic MechanismDorin PathakNo ratings yet
- Aneurysmal Subarachnoid Hemorrhage Nursing Self-Paced Case StudyDocument100 pagesAneurysmal Subarachnoid Hemorrhage Nursing Self-Paced Case StudyAndi rahma AnugrahNo ratings yet
- NCM 112 - Med SurgDocument7 pagesNCM 112 - Med SurgKierzteen Brianna TaromaNo ratings yet
- 2013 Abstract Book SmallDocument454 pages2013 Abstract Book SmallOscarNo ratings yet
- SciolyDocument91 pagesSciolyaarnavskrishnaNo ratings yet
- Nursing Diagnosis Planning Interventions Rationale Evaluation Risk For Ineffective Breathing Pattern IndependentDocument5 pagesNursing Diagnosis Planning Interventions Rationale Evaluation Risk For Ineffective Breathing Pattern Independentjeff_scarlet26No ratings yet
- Birth History - Prenatal, Perinatal, Postnatal Drainage, OtorrheaDocument12 pagesBirth History - Prenatal, Perinatal, Postnatal Drainage, OtorrheaWYNE BRENT M CORPUZNo ratings yet
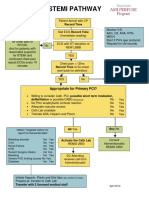
- Stemi Pathway: Record TimeDocument2 pagesStemi Pathway: Record TimeOlga Jadha CasmiraNo ratings yet
- Neuroscience Physical Therapy Evaluation FormDocument7 pagesNeuroscience Physical Therapy Evaluation FormTaral PatelNo ratings yet
- Program 1-CI AND Program 2 - AccCIBDocument2 pagesProgram 1-CI AND Program 2 - AccCIBRon CatalanNo ratings yet
- Antiarrhythmic DrugsDocument56 pagesAntiarrhythmic DrugsHassan MohammadNo ratings yet
- Cardiovascular Disease,: ObesityDocument24 pagesCardiovascular Disease,: ObesityEmran HossainNo ratings yet
- Calcium & Phosphorus DentalDocument48 pagesCalcium & Phosphorus Dentalfathimatezil123No ratings yet
- QB NeuroDocument30 pagesQB Neurorichard bolinaoNo ratings yet