Download as pdf or txt
You might also like
- CE (Vi) F (SK) PF1 (PS OM) PFA (SS) PN (SS) PDFDocument5 pagesCE (Vi) F (SK) PF1 (PS OM) PFA (SS) PN (SS) PDFrizqina ajraNo ratings yet
- Study of Prevalence and Risk Factors of Polycystic Ovarian Syndrome Among Adolescent and Young Adults of Rama UniversityDocument8 pagesStudy of Prevalence and Risk Factors of Polycystic Ovarian Syndrome Among Adolescent and Young Adults of Rama UniversityIJAR JOURNALNo ratings yet
- Medip, IJRCOG-8374 ODocument6 pagesMedip, IJRCOG-8374 Oalaesa2007No ratings yet
- Ijmps - Prevalence of Polycystic Ovarian Syndrome Among PDFDocument10 pagesIjmps - Prevalence of Polycystic Ovarian Syndrome Among PDFAnonymous bqctvu8P3VNo ratings yet
- 140 140 1 PBDocument4 pages140 140 1 PBMina LelymanNo ratings yet
- Original Research PaperDocument4 pagesOriginal Research PaperOviya ChitharthanNo ratings yet
- GWAS PCOS KoreaDocument9 pagesGWAS PCOS KoreaedwardNo ratings yet
- Endometrial Thickness As A Predictor of Endometrial HyperplasiaDocument28 pagesEndometrial Thickness As A Predictor of Endometrial HyperplasiaPirthi MannNo ratings yet
- Predicting Endometrial Hyperplasia and Endometrial Cancer On Recurrent Abnormal Uterine BleedingDocument7 pagesPredicting Endometrial Hyperplasia and Endometrial Cancer On Recurrent Abnormal Uterine Bleedingcarlos.gariza88No ratings yet
- Clinical Trends of Ectopic Pregnancy - A Study in A Tertiary Care Hospital of West Bengal, IndiaDocument7 pagesClinical Trends of Ectopic Pregnancy - A Study in A Tertiary Care Hospital of West Bengal, IndiaIJAR JOURNALNo ratings yet
- Abnormal Uteri BleedingDocument6 pagesAbnormal Uteri Bleedingdirani rahmanNo ratings yet
- 6 - Contemporary Management of Polycystic Ovarian Syndrome - 2019Document11 pages6 - Contemporary Management of Polycystic Ovarian Syndrome - 2019Johanna Bustos NutricionistaNo ratings yet
- 5f33a63892ff020200812article - PDF - FileStep-up Protocol Versus Conventional Dosage of Letrozole For Ovulation Induction in Women With PCOSDocument4 pages5f33a63892ff020200812article - PDF - FileStep-up Protocol Versus Conventional Dosage of Letrozole For Ovulation Induction in Women With PCOSAhmed AnwarNo ratings yet
- Cancer de Endometrio Preserv Fer 2021Document15 pagesCancer de Endometrio Preserv Fer 2021Claudia Mugruza BedoyaNo ratings yet
- Original ArticleDocument4 pagesOriginal ArticlefeyzarezarNo ratings yet
- Medip, IJRCOG-5630 O PDFDocument5 pagesMedip, IJRCOG-5630 O PDFSuraj NagarajNo ratings yet
- The Prevalence of Polycystic Ovary Syndrome in A Community Sample Assessed Under Contrasting Diagnostic CriteriaDocument8 pagesThe Prevalence of Polycystic Ovary Syndrome in A Community Sample Assessed Under Contrasting Diagnostic CriteriaKe XuNo ratings yet
- Gynecology & Reproductive HealthDocument6 pagesGynecology & Reproductive HealthtiaranindyNo ratings yet
- 10 1111@jog 143436777777Document17 pages10 1111@jog 143436777777Epiphany SonderNo ratings yet
- Health-Related Quality of Life in Adult MediterranDocument21 pagesHealth-Related Quality of Life in Adult MediterrancxksvhszsvNo ratings yet
- 3.杨欣 3.4区EN 多囊卵巢综合征合并无胰岛素抵抗子宫内膜的蛋白质组学和生物信息学分析 组学研究-Pcos 如何开展与筛选标准。Document8 pages3.杨欣 3.4区EN 多囊卵巢综合征合并无胰岛素抵抗子宫内膜的蛋白质组学和生物信息学分析 组学研究-Pcos 如何开展与筛选标准。johnheshanxiNo ratings yet
- Systematic Review On Recognising Patterns in Incidence of Polycystic Ovarian Syndrome in Young WomenDocument4 pagesSystematic Review On Recognising Patterns in Incidence of Polycystic Ovarian Syndrome in Young WomenInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 1 s2.0 S0020729209615502 Main PDFDocument1 page1 s2.0 S0020729209615502 Main PDFPaula UrsuNo ratings yet
- JURNALDocument11 pagesJURNALdiklat.rsakademis2024No ratings yet
- Cervical Cytology in Women With Abnormal Cervix.: Dr. Veena Rahatgaonkar, Dr. Savita MehendaleDocument4 pagesCervical Cytology in Women With Abnormal Cervix.: Dr. Veena Rahatgaonkar, Dr. Savita MehendaleIOSR Journal of PharmacyNo ratings yet
- Ijrcog-13706 oDocument7 pagesIjrcog-13706 olcddebllbNo ratings yet
- Evaluation of Some Immunological Aspects of Women With Polycystic Ovary Syndrome in Wasit GovernorateDocument8 pagesEvaluation of Some Immunological Aspects of Women With Polycystic Ovary Syndrome in Wasit GovernorateCentral Asian StudiesNo ratings yet
- AACE/ACE Disease State Clinical ReviewDocument10 pagesAACE/ACE Disease State Clinical ReviewSanjay NavaleNo ratings yet
- 2013 Article 414Document5 pages2013 Article 414Nisa MahmudahNo ratings yet
- Assessment of Thyroid and Prolactin Levels Among The Women With Abnormal Uterine BleedingDocument6 pagesAssessment of Thyroid and Prolactin Levels Among The Women With Abnormal Uterine BleedingMezouar AbdennacerNo ratings yet
- Is It Worth Preserving The Uterus? Unanticipated Pathology in Hysterectomy For Pelvic Organ Prolapse (POP)Document38 pagesIs It Worth Preserving The Uterus? Unanticipated Pathology in Hysterectomy For Pelvic Organ Prolapse (POP)Anonymous kte9KuGNo ratings yet
- Journal Gyn KETDocument8 pagesJournal Gyn KETImaylani S. SitanggangNo ratings yet
- Study On Ovarian Tumors in Pediatric and Adolescent Girls in A Tertiary Care CentreDocument7 pagesStudy On Ovarian Tumors in Pediatric and Adolescent Girls in A Tertiary Care CentreIJAR JOURNALNo ratings yet
- Soluble Urokinase-Type Plasminogen Activator Receptor (Supar) and Interleukin-6 Levels in Hyperemesis GravidarumDocument5 pagesSoluble Urokinase-Type Plasminogen Activator Receptor (Supar) and Interleukin-6 Levels in Hyperemesis GravidarumMuhammad AdithiaNo ratings yet
- Insight Into The Pathogensis of Polycystic OvarianDocument10 pagesInsight Into The Pathogensis of Polycystic OvarianHAVIZ YUADNo ratings yet
- Interactions Between Glioma and Pregnancy: Insight From A 52-Case Multicenter SeriesDocument11 pagesInteractions Between Glioma and Pregnancy: Insight From A 52-Case Multicenter Seriesppds ui jan2017No ratings yet
- Obstetric Complications in Women With Polycystic Ovary Syndrome: A Systematic Review and Meta-AnalysisDocument26 pagesObstetric Complications in Women With Polycystic Ovary Syndrome: A Systematic Review and Meta-AnalysisPany Chandra LestariNo ratings yet
- Risk Factors, Clinical Presentation and Treatment Modalities of Ectopic Pregnancy: A Cross Sectional Study at Tertiary Care HospitalDocument6 pagesRisk Factors, Clinical Presentation and Treatment Modalities of Ectopic Pregnancy: A Cross Sectional Study at Tertiary Care HospitalIJAR JOURNALNo ratings yet
- Impact of Oligohydramnios On Maternal and PerinataDocument6 pagesImpact of Oligohydramnios On Maternal and PerinataDiana SchlittlerNo ratings yet
- Anxiety in PCOSDocument5 pagesAnxiety in PCOSUsama Bin ZubairNo ratings yet
- Original Articles: Reproductive Endocrinology: A A B C D e e ADocument11 pagesOriginal Articles: Reproductive Endocrinology: A A B C D e e ACoco MelonNo ratings yet
- Study On Outcomes of PROMDocument5 pagesStudy On Outcomes of PROMRohit MaliNo ratings yet
- Whither PCOS The Challenges of Establishing Hyperandrogenism in Adolescent Girls 2008 Journal of Adolescent HealthDocument3 pagesWhither PCOS The Challenges of Establishing Hyperandrogenism in Adolescent Girls 2008 Journal of Adolescent HealthfujimeisterNo ratings yet
- Bakker 2012Document10 pagesBakker 2012ieoNo ratings yet
- JurnalDocument7 pagesJurnalEko WidodoNo ratings yet
- Journal Obgy Vitamin DDocument6 pagesJournal Obgy Vitamin Drosa snakNo ratings yet
- Diagnostics 13 01559Document13 pagesDiagnostics 13 01559Rifki YsNo ratings yet
- Lancet 2019Document11 pagesLancet 2019melinaparedes293No ratings yet
- Acog 194Document15 pagesAcog 194Marco DiestraNo ratings yet
- Atm 20 5463Document9 pagesAtm 20 5463Aline Costales TafoyaNo ratings yet
- Epidemiology of Polycystic Ovary Syndrome: A Cross Sectional Study of University Students at An-Najah National University-PalestineDocument6 pagesEpidemiology of Polycystic Ovary Syndrome: A Cross Sectional Study of University Students at An-Najah National University-PalestineOckta KaruniaNo ratings yet
- Phenotype Characteristics of PCOS BROSDocument10 pagesPhenotype Characteristics of PCOS BROSnarayani17No ratings yet
- ArticleDocument16 pagesArticleobbyNo ratings yet
- ImprovedDocument8 pagesImprovedCecilia CabanagNo ratings yet
- Thyroid Autoimmunity and Female Infertility: Kris Poppe, Daniel Glinoer, Brigitte VelkeniersDocument16 pagesThyroid Autoimmunity and Female Infertility: Kris Poppe, Daniel Glinoer, Brigitte VelkenierselenNo ratings yet
- Journal Pone 0105882Document7 pagesJournal Pone 0105882Ayu Wedhani SpcNo ratings yet
- Maternal Serum Triglycerides in Women With Pre-Eclampsia: Original ArticleDocument5 pagesMaternal Serum Triglycerides in Women With Pre-Eclampsia: Original ArticleGladys SusantyNo ratings yet
- Impact of Polycystic Ovary, Metabolic Syndrome and Obesity on Women Health: Volume 8: Frontiers in Gynecological EndocrinologyFrom EverandImpact of Polycystic Ovary, Metabolic Syndrome and Obesity on Women Health: Volume 8: Frontiers in Gynecological EndocrinologyNo ratings yet
- Translational Research in Breast CancerFrom EverandTranslational Research in Breast CancerDong-Young NohNo ratings yet
- Clinical Management of Infertility: Problems and SolutionsFrom EverandClinical Management of Infertility: Problems and SolutionsJoseph G. SchenkerNo ratings yet
- SpironolaktoneDocument2 pagesSpironolaktoneReza Ervanda ZilmiNo ratings yet
- Sparsh Gupta 14e-Anti Diabetes MCQDocument12 pagesSparsh Gupta 14e-Anti Diabetes MCQSubodh ChaudhariNo ratings yet
- Menstrual CycleDocument12 pagesMenstrual CycleJadessa VallarNo ratings yet
- Abnormal Uterine Bleeding: The Menstrual CycleDocument2 pagesAbnormal Uterine Bleeding: The Menstrual CycleindahmahfuzhahNo ratings yet
- 02 February 2022Document7 pages02 February 2022Vihan ShuklaNo ratings yet
- Developmental Disorders of The Gallbladder, Extrahepatic Biliary Tract, and PancreasDocument1 pageDevelopmental Disorders of The Gallbladder, Extrahepatic Biliary Tract, and PancreasbloodsphereNo ratings yet
- Diabetes ManagementDocument44 pagesDiabetes ManagementRahaf AlhubailNo ratings yet
- "A Study On The Awareness of Infertilityamong People": Investigatory Project ReportDocument36 pages"A Study On The Awareness of Infertilityamong People": Investigatory Project ReportSABARI SRINIVAS ANo ratings yet
- HD 201 E1 20140127 Histology of The Male Reproductive SystemDocument7 pagesHD 201 E1 20140127 Histology of The Male Reproductive SystemMaxine Alba100% (1)
- Prame HaDocument59 pagesPrame HaHajusha PNo ratings yet
- Does Masturbation Cause Acne in Men?Document3 pagesDoes Masturbation Cause Acne in Men?AndyJenkinsNo ratings yet
- Obstetric Complications in Women With Polycystic Ovary Syndrome: A Systematic Review and Meta-AnalysisDocument26 pagesObstetric Complications in Women With Polycystic Ovary Syndrome: A Systematic Review and Meta-AnalysisPany Chandra LestariNo ratings yet
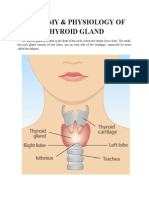
- Anatomy & Physiology of Thyroid GlandDocument5 pagesAnatomy & Physiology of Thyroid GlandJohnpaul DelapenaNo ratings yet
- CortisolDocument2 pagesCortisolkitu_alagappan4720No ratings yet
- Live Birth After IVF in A 46-Year-Old Woman: Case ReportDocument3 pagesLive Birth After IVF in A 46-Year-Old Woman: Case ReportReni ReniNo ratings yet
- Endocrine Quiz AnswersDocument31 pagesEndocrine Quiz AnswersDr Sumant Sharma100% (2)
- AKI FlowchartDocument1 pageAKI FlowchartTush RameNo ratings yet
- Embryology Lecture's NoteDocument11 pagesEmbryology Lecture's NotejdkejshNo ratings yet
- Hypothalamus and Pituitary GlandDocument48 pagesHypothalamus and Pituitary GlandMohsin AbbasNo ratings yet
- Articlee-Deac AndreiDocument3 pagesArticlee-Deac AndreiAndrei DeacNo ratings yet
- Gamatogenesis ProccesDocument15 pagesGamatogenesis ProccesvimamufliantiNo ratings yet
- Diabetes MellitusDocument9 pagesDiabetes MellitusErline Suzette GabrielNo ratings yet
- Final STD X Project Compiled 2023 - 24Document11 pagesFinal STD X Project Compiled 2023 - 24Kalavathi JNo ratings yet
- NASC 4 Fact or BluffDocument33 pagesNASC 4 Fact or BluffJona MangabanNo ratings yet
- Diabetes The NumbersDocument24 pagesDiabetes The NumbersSasikala RajendranNo ratings yet
- A P Research Paper DiabetesDocument8 pagesA P Research Paper Diabetesapi-353042837No ratings yet
- Reproductive System Old FormatDocument4 pagesReproductive System Old FormatRobie SanaoNo ratings yet
- Human Male and Female Reproductive System (Reviewer)Document8 pagesHuman Male and Female Reproductive System (Reviewer)Justine Yuan DoradoNo ratings yet
- Drug-Study-Metformin 1Document2 pagesDrug-Study-Metformin 1Caroline Cha100% (1)
- Suffix-Prefix and AbbreviationDocument2 pagesSuffix-Prefix and AbbreviationSachin TomarNo ratings yet