Download as pdf or txt
You might also like
- CSEC English SBA Dancehall and CrimeDocument26 pagesCSEC English SBA Dancehall and CrimeRichard DerbyNo ratings yet
- Toddler PDFDocument6 pagesToddler PDFYanti PutraNo ratings yet
- Benefits of Sexuality Education For Young People in NigeriaDocument12 pagesBenefits of Sexuality Education For Young People in NigeriaDebby Wura AbiodunNo ratings yet
- Kenku A Et AlDocument14 pagesKenku A Et Alabueza54No ratings yet
- Sexual Behaviour of In-School Rural Adolescents in Ogun State, NigeriaDocument9 pagesSexual Behaviour of In-School Rural Adolescents in Ogun State, Nigeriachidubemokpala2No ratings yet
- Olawa GB2019Document12 pagesOlawa GB2019game akunkecilNo ratings yet
- Experience of Non-Consensual Sex Among Students in A Tertiary Institution in Ibadan, NigeriaDocument9 pagesExperience of Non-Consensual Sex Among Students in A Tertiary Institution in Ibadan, NigeriaOlaleye Oladipupo SamNo ratings yet
- Abstinence From Premarital Sex: A Precursor To Quality Relationship and Marital Stability in Subsequent Marriage in Nigerian SocietyDocument7 pagesAbstinence From Premarital Sex: A Precursor To Quality Relationship and Marital Stability in Subsequent Marriage in Nigerian SocietyRomeo Jandugan Jr.No ratings yet
- Discrimination Against Girl Child in Rural Haryana, India: From Conception Through ChildhoodDocument20 pagesDiscrimination Against Girl Child in Rural Haryana, India: From Conception Through Childhoodpunjabi songsNo ratings yet
- Parental Attitudes and Sex Education of Children in NigeriaDocument8 pagesParental Attitudes and Sex Education of Children in NigeriaAlim SuardiNo ratings yet
- 43-1-10Document13 pages43-1-10Kyla FacturanNo ratings yet
- Ijrtsat 3 1 3Document9 pagesIjrtsat 3 1 3STATPERSON PUBLISHING CORPORATIONNo ratings yet
- Premarital Sex Safer Sex and Factors Influencing Premarital Sex Practices Among Senior Secondary School Students in Ebonyi Local Government Area of Ebonyi State NigeriaDocument5 pagesPremarital Sex Safer Sex and Factors Influencing Premarital Sex Practices Among Senior Secondary School Students in Ebonyi Local Government Area of Ebonyi State NigeriaCrissa Ysa PasilabanNo ratings yet
- Knowledge, Attitude, and Practice of Intimate Partner Violence and Its Determinants Among Female Nursing Students in Abakaliki, Southeast NigeriaDocument12 pagesKnowledge, Attitude, and Practice of Intimate Partner Violence and Its Determinants Among Female Nursing Students in Abakaliki, Southeast NigeriaLuis Daniel Nunez CubasNo ratings yet
- Teenage Pregnancy and Adolescent Sexual and Reproductive Health Behavior in Suhum, GhanaDocument17 pagesTeenage Pregnancy and Adolescent Sexual and Reproductive Health Behavior in Suhum, GhanaDaniel SumbiNo ratings yet
- Determinants of Risky Sexual Behaviours Among Secondary School Students in Delta State NigeriaDocument12 pagesDeterminants of Risky Sexual Behaviours Among Secondary School Students in Delta State NigeriaEdlawit DamessaNo ratings yet
- ELA LB 2019 Endline BriefingDocument2 pagesELA LB 2019 Endline BriefingD N FNo ratings yet
- Ajphes - Article 02Document11 pagesAjphes - Article 02Katy NelNo ratings yet
- PortrayalofSexualActsinNollywoodMovies AlongeetalDocument22 pagesPortrayalofSexualActsinNollywoodMovies AlongeetalkweensisanNo ratings yet
- Paper 7 PeerpressureDocument12 pagesPaper 7 PeerpressureShana VillamorNo ratings yet
- 10 51819-Jaltc 2021 1072048-2247892Document7 pages10 51819-Jaltc 2021 1072048-2247892blairNo ratings yet
- Peran Orang Tua Merupakan Faktor Dominan Terhadap Perilaku Seksual RemajaDocument6 pagesPeran Orang Tua Merupakan Faktor Dominan Terhadap Perilaku Seksual RemajaRosiana Amelia SariNo ratings yet
- Sexual Permissiveness Among AdolescentsDocument4 pagesSexual Permissiveness Among AdolescentsJohnmarkNo ratings yet
- Adolescence Is A Stage in Life in Which Sexual Behaviors Are Developing and Becoming EstablishedDocument3 pagesAdolescence Is A Stage in Life in Which Sexual Behaviors Are Developing and Becoming EstablishedJohnmarkNo ratings yet
- Female Genital Mutilation As A Socio-Cultural Determinant of Infant and Maternal Mortality in Delta StateDocument11 pagesFemale Genital Mutilation As A Socio-Cultural Determinant of Infant and Maternal Mortality in Delta StateResearch ParkNo ratings yet
- Factors Associated With The Premarital Sex Among Adolescents and The Need For Introduction of Functional Sex-Education in Secondary Schools in EbonyiDocument15 pagesFactors Associated With The Premarital Sex Among Adolescents and The Need For Introduction of Functional Sex-Education in Secondary Schools in EbonyiJohn Marc GONZALESNo ratings yet
- Attitude and Perceptions of University Students in Zimbabwe Towards HomosexualityDocument5 pagesAttitude and Perceptions of University Students in Zimbabwe Towards HomosexualityInternational Organization of Scientific Research (IOSR)No ratings yet
- Premarital Sex, Schoolgirl Pregnancy, and School Quality in Rural KenyaDocument17 pagesPremarital Sex, Schoolgirl Pregnancy, and School Quality in Rural KenyaRamanarayana BharadwajNo ratings yet
- Pre-Marital Sex and Health Outcomes Among Taiwanese Youth: Peer Influence and Contextual EffectDocument13 pagesPre-Marital Sex and Health Outcomes Among Taiwanese Youth: Peer Influence and Contextual EffectWeng WohNo ratings yet
- Filipino Adolescents' Sexual Attitudes and Behaviors: Results From A University CohortDocument11 pagesFilipino Adolescents' Sexual Attitudes and Behaviors: Results From A University CohortCameron Kaye ColamboNo ratings yet
- Experience of Gender-Based Violence To Students inDocument9 pagesExperience of Gender-Based Violence To Students inkorodeNo ratings yet
- Katz2019 - Only Yes Means Yes Sexual Coercion in Rural Adolescent Relationships PDFDocument3 pagesKatz2019 - Only Yes Means Yes Sexual Coercion in Rural Adolescent Relationships PDFRita RangelNo ratings yet
- Peer Influences On Sexual Activity Among Adolescents in GhanaDocument20 pagesPeer Influences On Sexual Activity Among Adolescents in GhanaSutrianiNo ratings yet
- 210-Article Text-410-1-10-20220216Document8 pages210-Article Text-410-1-10-20220216agbajihelennkechiNo ratings yet
- Analisis Faktor Yang Berhubungan Dengan Perilaku Seks Bebas Pada Remaja Di SMK DR Soetomo Surabaya Berdasarkan Teori Perilaku WhoDocument14 pagesAnalisis Faktor Yang Berhubungan Dengan Perilaku Seks Bebas Pada Remaja Di SMK DR Soetomo Surabaya Berdasarkan Teori Perilaku WhoMONIKA SUJOKONo ratings yet
- Knowledge and Perception of Teenage Pregnancy Among Secondary School Girls in Southern Ijaw Local Government Area of Bayelsa StateDocument8 pagesKnowledge and Perception of Teenage Pregnancy Among Secondary School Girls in Southern Ijaw Local Government Area of Bayelsa Stateijmb333No ratings yet
- Lta 1Document9 pagesLta 1Fiona RezfemyNo ratings yet
- Survival Analysis of Timing of First Marriage Among Women of Reproductive Age in Nigeria: Regional DifferencesDocument14 pagesSurvival Analysis of Timing of First Marriage Among Women of Reproductive Age in Nigeria: Regional Differencesbright winmetNo ratings yet
- CAIS2020 Paper25 AlongeDocument6 pagesCAIS2020 Paper25 AlongekweensisanNo ratings yet
- Prevalence Associated Risk Factors and C PDFDocument7 pagesPrevalence Associated Risk Factors and C PDFJay Bryson RuizNo ratings yet
- Child Rearing Practices and Cultural Inhibition As CorrelatesDocument9 pagesChild Rearing Practices and Cultural Inhibition As CorrelatesFAITH LEONARDNo ratings yet
- Topic Sentences (Pestaño and Martillan)Document8 pagesTopic Sentences (Pestaño and Martillan)Gerald HermosaNo ratings yet
- For MenDocument9 pagesFor MenRazkhal KunmoNo ratings yet
- Crisa Abstract 2Document1 pageCrisa Abstract 2Obosi Abel ChibuzorNo ratings yet
- Premarital Sex and Pregnancy I PDFDocument23 pagesPremarital Sex and Pregnancy I PDFRoyyan MursyidanNo ratings yet
- Abortion 7Document8 pagesAbortion 7Ram Chandra BogatiNo ratings yet
- Faktor - Faktor Yang Berhubungan Dengan Perilaku Seksual Remaja Yang Tinggal Di Lingkungan Resosialisasi Argorejo Kota SemarangDocument10 pagesFaktor - Faktor Yang Berhubungan Dengan Perilaku Seksual Remaja Yang Tinggal Di Lingkungan Resosialisasi Argorejo Kota SemarangYan ParirakNo ratings yet
- Risky Sexual Behaviors Among Unmarried Youth in India: Evidences From National Family Health Survey, 2019-21Document27 pagesRisky Sexual Behaviors Among Unmarried Youth in India: Evidences From National Family Health Survey, 2019-21skhushbusahniNo ratings yet
- JPAIRVol33CC 117 132Document16 pagesJPAIRVol33CC 117 132Jennifer Raya-TalaugonNo ratings yet
- 1 SMDocument6 pages1 SMedi_wsNo ratings yet
- 6C Bullying00202Document8 pages6C Bullying00202Idayu Badilla IdrisNo ratings yet
- OKPAKO & DOTIMI Justification For Sexuality EducationDocument12 pagesOKPAKO & DOTIMI Justification For Sexuality Educationvirus_xxxNo ratings yet
- Exploring Safe Sex Awareness and Sexual Experiences of Adolescents in PatnaDocument8 pagesExploring Safe Sex Awareness and Sexual Experiences of Adolescents in PatnaRishabh K RanaNo ratings yet
- Emerging Teen Fatherhood and Its Implications For National DevelopmentDocument15 pagesEmerging Teen Fatherhood and Its Implications For National DevelopmentLAILANE MAE LAGMAYNo ratings yet
- Lta 1Document9 pagesLta 1Fiona RezfemyNo ratings yet
- Family Planning Service Utilization in Mojo Town E (2) 33333333333333333Document10 pagesFamily Planning Service Utilization in Mojo Town E (2) 33333333333333333yonasalemayehu49No ratings yet
- Social Wellbeing and Quality oDocument20 pagesSocial Wellbeing and Quality oRun CapNo ratings yet
- MarriageJBSpaper ChoeThapaVinodDocument21 pagesMarriageJBSpaper ChoeThapaVinodsanjaNo ratings yet
- Influence of Peer Pressure As A Determinant of Premarital Sexual Behaviour Among Senior Secondary School Students in Kaduna State, NigeriaDocument9 pagesInfluence of Peer Pressure As A Determinant of Premarital Sexual Behaviour Among Senior Secondary School Students in Kaduna State, Nigeriaramadhanti salsabilaNo ratings yet
- Secrets: The Conflicted Role of First-Generation Nigerian American Women Experiencing Domestic ViolenceFrom EverandSecrets: The Conflicted Role of First-Generation Nigerian American Women Experiencing Domestic ViolenceNo ratings yet
- The POCSO Act and Associated Issues - ForumIAS BlogDocument8 pagesThe POCSO Act and Associated Issues - ForumIAS BlogAjeet KumarNo ratings yet
- Schindel y Colombo 2014Document282 pagesSchindel y Colombo 2014martina eva garcia100% (1)
- Samra Shehzadi, Peace Psy, Assignment 1Document12 pagesSamra Shehzadi, Peace Psy, Assignment 1Fatima MalikNo ratings yet
- Cell Count Issue 83Document12 pagesCell Count Issue 83Cell CountNo ratings yet
- The Philippine Commission On Women States That Violence Against WomenDocument1 pageThe Philippine Commission On Women States That Violence Against WomenFederico TomayaoNo ratings yet
- Professionals and Practitioners in CounselingDocument25 pagesProfessionals and Practitioners in CounselingLuna Dela CruzNo ratings yet
- Stages of Genocide1Document17 pagesStages of Genocide1api-237645575No ratings yet
- Unlocking DiscriminationDocument34 pagesUnlocking DiscriminationChristina SturdivantNo ratings yet
- Business Continuity PlanDocument52 pagesBusiness Continuity PlanGigi De LeonNo ratings yet
- City Limits Magazine, Behind Bars - Love, Sex, Rape and New York's Women PrisonersDocument48 pagesCity Limits Magazine, Behind Bars - Love, Sex, Rape and New York's Women PrisonersCity Limits (New York)No ratings yet
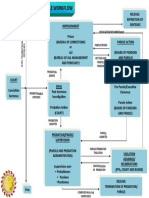
- Probation and Parole WorkflowDocument1 pageProbation and Parole WorkflowDoni June AlmioNo ratings yet
- Gender and Violence in Toni Morrison's A MercyDocument20 pagesGender and Violence in Toni Morrison's A MercyAida Dziho-SatorNo ratings yet
- Conflict With The Law PDFDocument2 pagesConflict With The Law PDFJupiter ZangelNo ratings yet
- Small Arms ReviewDocument213 pagesSmall Arms ReviewRebecca Rivers100% (1)
- AssaultDocument2 pagesAssaultBeatrice MatamaNo ratings yet
- 66-People v. Genosa-G.R. No. 135981-Jan. 15, 2004Document2 pages66-People v. Genosa-G.R. No. 135981-Jan. 15, 2004Jude Thaddeus DamianNo ratings yet
- MR Sanjiv Bhatt Writes To SIT Chairman MR R K Raghavan in Regards To Prosecuting Narendra Modi - 25 Jan 2012Document109 pagesMR Sanjiv Bhatt Writes To SIT Chairman MR R K Raghavan in Regards To Prosecuting Narendra Modi - 25 Jan 2012sneh7940No ratings yet
- Borders Kritik - UTNIF 2013Document257 pagesBorders Kritik - UTNIF 2013James Tyler AdamsNo ratings yet
- Honour Based Violence in Kurdish CommunitiesDocument11 pagesHonour Based Violence in Kurdish CommunitiesSDaroosterNo ratings yet
- Ush 5.04HDocument2 pagesUsh 5.04HAubrey HovanNo ratings yet
- Invitations To Responsibility The Therapeutic Engagement of Men Who Are Violent and Abusive (Jenkins, Alan) (Z-Library)Document280 pagesInvitations To Responsibility The Therapeutic Engagement of Men Who Are Violent and Abusive (Jenkins, Alan) (Z-Library)Adriana Marcela Galeano AmayaNo ratings yet
- Ostrich Sensitive Text Categorization InstructionsDocument19 pagesOstrich Sensitive Text Categorization InstructionsKenn ReyesNo ratings yet
- FMST 314 Finals NotesDocument8 pagesFMST 314 Finals NotesmoomoomaoNo ratings yet
- Nurnberg Media Workshop Programme 1 December 2014 FINALDocument2 pagesNurnberg Media Workshop Programme 1 December 2014 FINALWayamo FoundationNo ratings yet
- IntroductionDocument12 pagesIntroductionMahar Asif AliNo ratings yet
- Leon County Sheriff'S Office Daily Booking Report 16-Oct-2020 Page 1 of 3Document3 pagesLeon County Sheriff'S Office Daily Booking Report 16-Oct-2020 Page 1 of 3WCTV Digital Team100% (1)
- DCPCR Guidelines 14052014Document172 pagesDCPCR Guidelines 14052014Vaishnavi JayakumarNo ratings yet
- Q4 HEALTH 9 Module 1 Week1.ALPHA TESTEDDocument14 pagesQ4 HEALTH 9 Module 1 Week1.ALPHA TESTEDCyris Gay AdolfoNo ratings yet
- Not in Our Name - EnglishDocument196 pagesNot in Our Name - EnglishSanjana HattotuwaNo ratings yet