Download as pdf or txt
You might also like
- Disability HandbookDocument231 pagesDisability HandbookRoberto Manuel Meléndez NegrónNo ratings yet
- ملف 58 معدلDocument58 pagesملف 58 معدلraghdah alhogailNo ratings yet
- NCP DengueDocument8 pagesNCP Dengueelaine_tengco50% (2)
- Normal Flora of HumanDocument54 pagesNormal Flora of Humankumari astha rupaliNo ratings yet
- LabReportNew - 2024-07-09T165725.084Document3 pagesLabReportNew - 2024-07-09T165725.084Maroof AliNo ratings yet
- Krishan Lal PDFDocument10 pagesKrishan Lal PDFAyub AlamNo ratings yet
- KARANVEERDocument7 pagesKARANVEER81688samsungNo ratings yet
- Krishan Lal PDFDocument5 pagesKrishan Lal PDFAyub AlamNo ratings yet
- Haematology: Investigation Observed Value Unit Biological Reference IntervalDocument10 pagesHaematology: Investigation Observed Value Unit Biological Reference IntervalVanshitaNo ratings yet
- 58 Ebabeea 44 e 8Document8 pages58 Ebabeea 44 e 8AL Wahid SpareNo ratings yet
- Haematology Basic Screening Package Complete Blood Count (CBC EXT)Document6 pagesHaematology Basic Screening Package Complete Blood Count (CBC EXT)Anil PeshinNo ratings yet
- SK Singh Lab Report 09042018Document8 pagesSK Singh Lab Report 09042018ankit ojhaNo ratings yet
- Med111487409 33864299 118 79600569Document7 pagesMed111487409 33864299 118 79600569Akhil MuraliNo ratings yet
- Haematology Basic Screening Package Complete Blood Count (CBC EXT)Document6 pagesHaematology Basic Screening Package Complete Blood Count (CBC EXT)Anil PeshinNo ratings yet
- Haematology: Investigation Observed Value Unit Biological Reference IntervalDocument2 pagesHaematology: Investigation Observed Value Unit Biological Reference IntervalVivek RadhakrishnanNo ratings yet
- Haematology: Investigation Observed Value Unit Biological Reference IntervalDocument6 pagesHaematology: Investigation Observed Value Unit Biological Reference IntervalumeshlpsNo ratings yet
- Kamala Kannan KDocument5 pagesKamala Kannan Kparamesh.sriram2194No ratings yet
- Test Results Units Biological Reference Range Hematology:::::: Ms. Farha MemonDocument5 pagesTest Results Units Biological Reference Range Hematology:::::: Ms. Farha MemonKM GASTRO CENTERNo ratings yet
- Wa0110Document3 pagesWa0110venkat yeluriNo ratings yet
- 4700003265: Patient ID 47000838 Sid No Mumbai Branch Mr. DEENBANDHU (89579)Document9 pages4700003265: Patient ID 47000838 Sid No Mumbai Branch Mr. DEENBANDHU (89579)Deenbandhu SahaniNo ratings yet
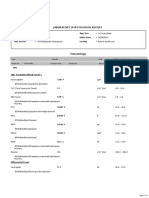
- Laboratory Investigation ReportDocument2 pagesLaboratory Investigation ReportAnilNo ratings yet
- Haematology Complete Hemogram WBC Parameter: Test Obtained Value Units Bio - Ref.IntervalsDocument3 pagesHaematology Complete Hemogram WBC Parameter: Test Obtained Value Units Bio - Ref.IntervalsRANJITGANA TVM24No ratings yet
- Fully Automated Lab Accurate Reports Reports Verified by PathologistDocument11 pagesFully Automated Lab Accurate Reports Reports Verified by PathologistBathri NathanNo ratings yet
- Authenticity CheckDocument2 pagesAuthenticity Checkvlande897No ratings yet
- Abhishek Avate19211531Document2 pagesAbhishek Avate19211531vlande897No ratings yet
- SK Singh Lab Report 09042018Document8 pagesSK Singh Lab Report 09042018Iasam Groups'sNo ratings yet
- Haematology Complete Blood Count (CBC EXT) : 021808250310 MR - AJAY KUMAR 662326Document7 pagesHaematology Complete Blood Count (CBC EXT) : 021808250310 MR - AJAY KUMAR 662326ANSHU KUMAR RANANo ratings yet
- Haematology: Investigation Observed Value Unit Biological Reference IntervalDocument9 pagesHaematology: Investigation Observed Value Unit Biological Reference IntervalSandeep Konapur M KNo ratings yet
- Full ReportDocument16 pagesFull ReportGarv BaliNo ratings yet
- 866 PDFDocument1 page866 PDFMalarVizhiNo ratings yet
- Mali T11Document2 pagesMali T11vlande897No ratings yet
- 5 10 2024123458PMfinalDocument3 pages5 10 2024123458PMfinalRakhi PritamNo ratings yet
- Rajendra Singh KushwahaDocument3 pagesRajendra Singh KushwahadrneerajpalsinghNo ratings yet
- 13 Apr 2024Document7 pages13 Apr 2024Nitul DoshiNo ratings yet
- Haematology: Investigation Observed Value Unit Biological Reference IntervalDocument6 pagesHaematology: Investigation Observed Value Unit Biological Reference IntervalShankara NarayanaNo ratings yet
- Lab Report 12452726 20230404120153Document4 pagesLab Report 12452726 20230404120153Amal SMNo ratings yet
- Yash Yadav - 2406103Document3 pagesYash Yadav - 2406103dr.menganeNo ratings yet
- MAHAAM3Document2 pagesMAHAAM3vlande897No ratings yet
- ABHIDE2Document5 pagesABHIDE2vlande897No ratings yet
- Complete Blood Picture: Clincal Pathology Consultant DR - Khaled AbdellahDocument2 pagesComplete Blood Picture: Clincal Pathology Consultant DR - Khaled Abdellahbasl.hazm34No ratings yet
- Indra Lal - (MRN 1006076) - 1023001085Document3 pagesIndra Lal - (MRN 1006076) - 1023001085yukeonnaNo ratings yet
- Fully Automated Lab Accurate Reports Reports Verified by PathologistDocument9 pagesFully Automated Lab Accurate Reports Reports Verified by PathologistJayshree BawaniyaNo ratings yet
- Department of Hematology Comprehensive Full Body Checkup Test Name Result Unit Bio. Ref. IntervalDocument11 pagesDepartment of Hematology Comprehensive Full Body Checkup Test Name Result Unit Bio. Ref. IntervalshyamNo ratings yet
- Shahbaz Khan 2406082Document2 pagesShahbaz Khan 2406082dr.menganeNo ratings yet
- SAKH21Document2 pagesSAKH21vlande897No ratings yet
- 8000000936: Patient ID 80001350 Sid No Nehru Nagar Branch Mr. Vasanth NDocument3 pages8000000936: Patient ID 80001350 Sid No Nehru Nagar Branch Mr. Vasanth NSudha SaravananNo ratings yet
- Kgmu Trauma 22092200943 7355326825Document2 pagesKgmu Trauma 22092200943 7355326825Ravi KumarNo ratings yet
- ATTAR49Document10 pagesATTAR49vlande897No ratings yet
- Complete Blood Count: Test Reference Range Unit MethodologyDocument1 pageComplete Blood Count: Test Reference Range Unit MethodologytahazaidiNo ratings yet
- Ms SEEMABALAYAN 9 24 2022 7 04 10 PMDocument22 pagesMs SEEMABALAYAN 9 24 2022 7 04 10 PMMohammad Ali NPNo ratings yet
- PdfText - 2023-06-01T222329.740Document8 pagesPdfText - 2023-06-01T222329.740Rahul NemadeNo ratings yet
- Archana Lab ReportDocument10 pagesArchana Lab Reportprabalsoni125No ratings yet
- 1-Glucose - Postprandial - PO2611259108-802Document16 pages1-Glucose - Postprandial - PO2611259108-802Meet PatelNo ratings yet
- Haematology: Investigation Observed Value Unit Biological Reference IntervalDocument5 pagesHaematology: Investigation Observed Value Unit Biological Reference Intervalshivanand.n ShivanandNo ratings yet
- Erythrocytes: Reference: DR - SELF Mrs. Rashmi VID: 15821730013744Document6 pagesErythrocytes: Reference: DR - SELF Mrs. Rashmi VID: 15821730013744Senthil VelNo ratings yet
- Rajesh R D - 2312316Document2 pagesRajesh R D - 2312316dr.menganeNo ratings yet
- Shankar 30P00430014990Document1 pageShankar 30P00430014990ShankarNo ratings yet
- Hematology Test Name (Methodology) Result Flag Units Biological Reference IntervalDocument2 pagesHematology Test Name (Methodology) Result Flag Units Biological Reference IntervalMonu SahotaNo ratings yet
- SMT Lakshmi Devi 07 05 2024 02 53 48 PMDocument2 pagesSMT Lakshmi Devi 07 05 2024 02 53 48 PMraghuveera407No ratings yet
- Sona.M:::: Patient Age / Sex 40 Y / Female BranchDocument7 pagesSona.M:::: Patient Age / Sex 40 Y / Female Branchsuresh babujiNo ratings yet
- 37120500696#43440#37120500696#1 - 11 - 2020 12 - 00 - 00 AmDocument2 pages37120500696#43440#37120500696#1 - 11 - 2020 12 - 00 - 00 AmMohammad BolockNo ratings yet
- Screenshot 2023-12-19 at 15.34.42Document3 pagesScreenshot 2023-12-19 at 15.34.42yukeonnaNo ratings yet
- Screenshot 2023-12-19 at 15.34.42Document3 pagesScreenshot 2023-12-19 at 15.34.42yukeonnaNo ratings yet
- 27.4 Immune Response-1Document3 pages27.4 Immune Response-1Melissa ShamburgNo ratings yet
- NCP Post TermDocument2 pagesNCP Post TermFhairy Jhoy Rhayta100% (1)
- Biology TmaDocument7 pagesBiology TmaMISS RASHMINo ratings yet
- Listingempannednewlist 04052023Document27 pagesListingempannednewlist 04052023dhawalduvey95No ratings yet
- CTE NFL Part 1 PDFDocument7 pagesCTE NFL Part 1 PDFMariana PardoNo ratings yet
- R/ The Alternative Term Are Not Entirely Appropriate Because It Can Be Misleading, Even Unpleasant For Some PeopleDocument2 pagesR/ The Alternative Term Are Not Entirely Appropriate Because It Can Be Misleading, Even Unpleasant For Some PeopleLaura BorjaNo ratings yet
- Obstetrics and Gynecology SpecialtyDocument96 pagesObstetrics and Gynecology SpecialtyAdis Gudukasa100% (1)
- All NCPsDocument83 pagesAll NCPsDennis Nyambane Momanyi100% (6)
- CPW Drugs in PPMP Number of DuplictesDocument9 pagesCPW Drugs in PPMP Number of DuplictesSunshine BNo ratings yet
- Jinnah Postgraduate Medical Centre KarachiDocument3 pagesJinnah Postgraduate Medical Centre KarachiFatima FaizanNo ratings yet
- Annotated BibliographyDocument3 pagesAnnotated Bibliographyjuadel316100% (1)
- Working As A Team in Airway Surgery History Pres 2021 Seminars in PediatriDocument6 pagesWorking As A Team in Airway Surgery History Pres 2021 Seminars in PediatriSavaNo ratings yet
- Drug Therapy Assessment Worksheet (Dtaw) : 1. A Problem ExistsDocument6 pagesDrug Therapy Assessment Worksheet (Dtaw) : 1. A Problem ExistsputriNo ratings yet
- EFEKTIVITAS PERASAN DAUN BUNGA SEPATU (Hibiscus Rosa-Sinensis L) TERHADAP PERTUMBUHAN Staphylococcus AureusDocument5 pagesEFEKTIVITAS PERASAN DAUN BUNGA SEPATU (Hibiscus Rosa-Sinensis L) TERHADAP PERTUMBUHAN Staphylococcus Aureusverawaty watyNo ratings yet
- Jeyakumar Dhileeban Rrroll 41Document34 pagesJeyakumar Dhileeban Rrroll 41Rupesh TamizhaNo ratings yet
- Sympathetic GanglionectomyDocument8 pagesSympathetic GanglionectomyCeaGarsakyNo ratings yet
- Circulatory System: (Blood Transport)Document27 pagesCirculatory System: (Blood Transport)Josephine AcioNo ratings yet
- Presenter 1: Psychological Causes of Drug AddictionDocument4 pagesPresenter 1: Psychological Causes of Drug AddictionJeremiah AimitonNo ratings yet
- Alfa - CBC 2Document1 pageAlfa - CBC 2ayaabouaufNo ratings yet
- Case Pres Drug Study RevisionDocument3 pagesCase Pres Drug Study RevisionJose Luis HernandezNo ratings yet
- Anesthesia Quiz With ReferencesDocument16 pagesAnesthesia Quiz With ReferencesfrancisNo ratings yet
- Parto Prematuro ACOGDocument10 pagesParto Prematuro ACOGAngela_Maria_M_7864No ratings yet
- Amoxgentin - Amoxycillin & Potassium Clavulanate Injection - Export 600mg I.V - InFODocument1 pageAmoxgentin - Amoxycillin & Potassium Clavulanate Injection - Export 600mg I.V - InFOAnonymous BVD7IKfNo ratings yet
- Do's and Dont's During PregnancyDocument11 pagesDo's and Dont's During PregnancyNinoyz™100% (2)
- Comparative in Vitro Study of The Antimicrobial Efficacy of Nigella Sativa Seed Oil (Black Seed Oil) Against Selected Microorganisms With Conventional AntibiticsDocument4 pagesComparative in Vitro Study of The Antimicrobial Efficacy of Nigella Sativa Seed Oil (Black Seed Oil) Against Selected Microorganisms With Conventional AntibiticsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Cancer Pain ManagementDocument40 pagesCancer Pain ManagementindahirmawatiNo ratings yet