Download as pdf or txt
You might also like
- Price Action Market Traps 7 Trap PDFDocument85 pagesPrice Action Market Traps 7 Trap PDFPradeep Chandra71% (7)
- ITECH5500 Mini Research ProposalDocument11 pagesITECH5500 Mini Research ProposalFarheen AhmedNo ratings yet
- Activity 6 GALUPODocument7 pagesActivity 6 GALUPOSophia Manila SillaNo ratings yet
- Deterministic Modelling BiomechanicDocument16 pagesDeterministic Modelling Biomechanicperakang00No ratings yet
- Applied Multivariate Statistical Analysis Solution Manual PDFDocument18 pagesApplied Multivariate Statistical Analysis Solution Manual PDFALVYAN ARIFNo ratings yet
- 3 s2.0 B9780128096338200794 MainDocument8 pages3 s2.0 B9780128096338200794 MainNishad Bapat-DharNo ratings yet
- Dynamic Medicine: Comparison of Two Normative Paediatric Gait DatabasesDocument7 pagesDynamic Medicine: Comparison of Two Normative Paediatric Gait DatabasesDiana Sofia AgredaNo ratings yet
- Imputation of Clinical Covariates in Time Series: Dimitris Bertsimas Agni Orfanoudaki Colin PawlowskiDocument64 pagesImputation of Clinical Covariates in Time Series: Dimitris Bertsimas Agni Orfanoudaki Colin PawlowskiSergio AlumendaNo ratings yet
- Dissertation Svenja CaspersDocument11 pagesDissertation Svenja CaspersBestPaperWritingServicesCanada100% (1)
- Cuellar2019efficient - Efficient Data Management Infrastructure For The Integration of Imaging and Omics Data in Life Science ResearchDocument24 pagesCuellar2019efficient - Efficient Data Management Infrastructure For The Integration of Imaging and Omics Data in Life Science ResearchbgilotNo ratings yet
- Medical Statistics Thesis PDFDocument5 pagesMedical Statistics Thesis PDFtracyjimenezstamford100% (3)
- Biology and Data Interpretation Techniques ConceptsDocument2 pagesBiology and Data Interpretation Techniques ConceptsVani DarjiNo ratings yet
- Extracting Formulaic and Free Text Clinical Research Articles Metadata Using Conditional Random FieldsDocument6 pagesExtracting Formulaic and Free Text Clinical Research Articles Metadata Using Conditional Random FieldsMailtoNo ratings yet
- The Logic of Exploratory and Confirmatory Data Analysis: January 2011Document15 pagesThe Logic of Exploratory and Confirmatory Data Analysis: January 2011Nguyễn VỉnhNo ratings yet
- Data Mining Mphil Thesis PDFDocument8 pagesData Mining Mphil Thesis PDFAngela Shin100% (2)
- On Bioinformatic ResourcesDocument7 pagesOn Bioinformatic ResourcesGana Ibrahim HassanNo ratings yet
- Applied Sciences: Smart HealthcareDocument5 pagesApplied Sciences: Smart HealthcareSumathi GowdaNo ratings yet
- Koo Che Mesh Kian 2020Document26 pagesKoo Che Mesh Kian 2020Mahdi KarimiNo ratings yet
- Artificial Intelligence and Data MiningDocument211 pagesArtificial Intelligence and Data MiningAbderrazek ZeraiiNo ratings yet
- Computational Biology and BioinformaticsDocument11 pagesComputational Biology and BioinformaticsBangaru BabuNo ratings yet
- Journal of Foot and Ankle Research: Normative Values For The Foot Posture IndexDocument9 pagesJournal of Foot and Ankle Research: Normative Values For The Foot Posture IndexAnup PednekarNo ratings yet
- Machine Learning and Electronic Health Records A PDocument3 pagesMachine Learning and Electronic Health Records A PArnob TanjimNo ratings yet
- Research Papers Computers in Medical FieldDocument7 pagesResearch Papers Computers in Medical Fieldkrqovxbnd100% (1)
- Sudan University of Science & Technology College of Engineering MSC Biomedical EngineeringDocument15 pagesSudan University of Science & Technology College of Engineering MSC Biomedical Engineeringمحمد أحمد عبدالوهاب محمدNo ratings yet
- A Literature Review in Health Informatics Using Data Mining TechniquesDocument5 pagesA Literature Review in Health Informatics Using Data Mining TechniquesafmzzgidncysunNo ratings yet
- Bioinformatics Thesis DownloadDocument8 pagesBioinformatics Thesis Downloadkatrinagreeneugene100% (2)
- Project 5467Document13 pagesProject 5467stephennrobertNo ratings yet
- Classification of Interviews - A Case Study On Cancer PatientsDocument10 pagesClassification of Interviews - A Case Study On Cancer Patientspatel_musicmsncomNo ratings yet
- Symptom Science: Repurposing Existing Omics DataDocument10 pagesSymptom Science: Repurposing Existing Omics DataSircaNo ratings yet
- Advance Statistical Methods in Data Science ChenDocument229 pagesAdvance Statistical Methods in Data Science Chene-cevik100% (1)
- Ebook Modern Statistical Methods For Health Research 1St Edition Yichuan Zhao Online PDF All ChapterDocument69 pagesEbook Modern Statistical Methods For Health Research 1St Edition Yichuan Zhao Online PDF All Chaptercody.robles478100% (7)
- Zlib - Pub Advanced Data Analytics in HealthDocument221 pagesZlib - Pub Advanced Data Analytics in HealthyosNo ratings yet
- Bio Final Report BTDocument15 pagesBio Final Report BTK NandanNo ratings yet
- Systematic Literature Review EpidemiologyDocument6 pagesSystematic Literature Review Epidemiologyc5qx9hq5100% (1)
- Seminar ReportDocument25 pagesSeminar ReportTejaswiniNo ratings yet
- Challenges and Opportunities in Coding The Commons: Problems, Procedures, and Potential Solutions in Large-N Comparative Case StudiesDocument27 pagesChallenges and Opportunities in Coding The Commons: Problems, Procedures, and Potential Solutions in Large-N Comparative Case StudiesAlan HartogNo ratings yet
- Dynamics of Human GaitDocument73 pagesDynamics of Human GaitAjinkya JainNo ratings yet
- ImputabilityDocument12 pagesImputability康乘舟No ratings yet
- A Survey of Transfer and Multitask Learning in BioinformaticsDocument12 pagesA Survey of Transfer and Multitask Learning in BioinformaticsJefferson Quispe PinaresNo ratings yet
- An Improved Rank Based Disease Prediction Using Web Navigation Patterns On Bio-Medical DatabasesDocument15 pagesAn Improved Rank Based Disease Prediction Using Web Navigation Patterns On Bio-Medical DatabasesRamani KNo ratings yet
- The Case For Researching Biomechanics and Human Movement Using A Stochastic Model in A Peer Reviewed Journal To Generate Qualitative EvidenceDocument3 pagesThe Case For Researching Biomechanics and Human Movement Using A Stochastic Model in A Peer Reviewed Journal To Generate Qualitative Evidencedennis shavelsonNo ratings yet
- University of Reading MSC DissertationDocument7 pagesUniversity of Reading MSC DissertationBuyThesisPaperVirginiaBeach100% (1)
- Bitstream 3552674Document21 pagesBitstream 3552674himanshu011623No ratings yet
- Big Data Analytics For Personalized Medicine: SciencedirectDocument7 pagesBig Data Analytics For Personalized Medicine: Sciencedirectbagas parlambangNo ratings yet
- JPB3 1Document4 pagesJPB3 1Muhammad TahirNo ratings yet
- Veterinary Computer Software Research PaperDocument6 pagesVeterinary Computer Software Research Papertrsrpyznd100% (1)
- Mass Spectrometry Big Data To KnowledgeDocument49 pagesMass Spectrometry Big Data To KnowledgeChris LinNo ratings yet
- Data Mining MetaAnalysisDocument39 pagesData Mining MetaAnalysispaparountasNo ratings yet
- Paràmetres A Medir en La Marxa HumanaDocument28 pagesParàmetres A Medir en La Marxa HumanaMaria Antonia Mateu PonsNo ratings yet
- A Fuzzy Based Association Mining Approach For Medical Disease PredictionDocument3 pagesA Fuzzy Based Association Mining Approach For Medical Disease PredictionIJERDNo ratings yet
- Literature Review On HmisDocument7 pagesLiterature Review On Hmisea219sww100% (1)
- Dissertation InstrumentationDocument5 pagesDissertation InstrumentationCustomPaperWritingServicesUK100% (1)
- BMC Bioinformatics: Comparison of Concept Recognizers For Building The Open Biomedical AnnotatorDocument9 pagesBMC Bioinformatics: Comparison of Concept Recognizers For Building The Open Biomedical AnnotatorMohy Abonoh0% (1)
- UntitledDocument3 pagesUntitledRameshchandra K ECENo ratings yet
- A Survey of Deep Learning Models Final 2.0Document42 pagesA Survey of Deep Learning Models Final 2.0nessrine blelNo ratings yet
- Literature Review Data Extraction ToolDocument4 pagesLiterature Review Data Extraction Toolafdtalblw100% (1)
- Limitations Systematic Literature ReviewDocument5 pagesLimitations Systematic Literature Reviewc5rqq644100% (1)
- Wearable Sensors For Clinical Applications in Epilepsy, Parkinson's Disease, and Stroke: A Mixed Methods Systematic ReviewDocument13 pagesWearable Sensors For Clinical Applications in Epilepsy, Parkinson's Disease, and Stroke: A Mixed Methods Systematic ReviewMANIMEGALAI M. ECENo ratings yet
- Begon Et Al. - 2018 - Multibody Kinematics Optimization For The EstimatiDocument45 pagesBegon Et Al. - 2018 - Multibody Kinematics Optimization For The EstimatiLou StuhlsNo ratings yet
- Xóa 2Document21 pagesXóa 2Rin TohsakaNo ratings yet
- Muniz 2010Document7 pagesMuniz 2010seyedmohamadNo ratings yet
- Par Des 2016Document6 pagesPar Des 2016seyedmohamadNo ratings yet
- Archive of SID: Functional Movement Screening FMS Deep Squat LungeDocument11 pagesArchive of SID: Functional Movement Screening FMS Deep Squat LungeseyedmohamadNo ratings yet
- Understanding Muscle Coordination of The Human Leg With Dynamical SimulationsDocument8 pagesUnderstanding Muscle Coordination of The Human Leg With Dynamical SimulationsseyedmohamadNo ratings yet
- Journal of Biomechanics: Marcel Dreischarf, Antonius Rohlmann, Friedmar Graichen, Georg Bergmann, Hendrik SchmidtDocument6 pagesJournal of Biomechanics: Marcel Dreischarf, Antonius Rohlmann, Friedmar Graichen, Georg Bergmann, Hendrik SchmidtseyedmohamadNo ratings yet
- Journal of Biomechanics: Aaron M. Kociolek, Jimmy Tat, Peter J. KeirDocument7 pagesJournal of Biomechanics: Aaron M. Kociolek, Jimmy Tat, Peter J. KeirseyedmohamadNo ratings yet
- 1137200L AutoSet Manual ExtranetDocument102 pages1137200L AutoSet Manual Extranetaggarwalsahil88No ratings yet
- Quantum Information Theory Chapter 1Document12 pagesQuantum Information Theory Chapter 1juanNo ratings yet
- Determination of Negative Permittivity and PermeabDocument6 pagesDetermination of Negative Permittivity and PermeabNewton GomesNo ratings yet
- Computation of Abutment Scour Using HEC-18 Equations SpreadsheetDocument7 pagesComputation of Abutment Scour Using HEC-18 Equations SpreadsheetAfolabi OladunniNo ratings yet
- Brochure In-Lite - EN - 2019Document122 pagesBrochure In-Lite - EN - 2019Roi HbbNo ratings yet
- Making Your Sailor S1303 Free-RunningDocument15 pagesMaking Your Sailor S1303 Free-Runningmrservice7782No ratings yet
- ALD Management (SRAN15.1 02)Document160 pagesALD Management (SRAN15.1 02)waelq20030% (1)
- Airavata DasaDocument67 pagesAiravata DasayogalinkNo ratings yet
- Editing, Coding, Data Entry, TabulationDocument3 pagesEditing, Coding, Data Entry, TabulationNutukurthi Venkat Ramji100% (1)
- Sachin ArjoonsinghDocument9 pagesSachin ArjoonsinghCharlotte BNo ratings yet
- Homework Practice Ordering Real NumbersDocument1 pageHomework Practice Ordering Real Numbersapi-2932600260% (1)
- Interpreting Tables and ChartsDocument3 pagesInterpreting Tables and ChartsLILIAN ROSE DE LARANo ratings yet
- FitanezajowetavinewulDocument2 pagesFitanezajowetavinewulmavas istaNo ratings yet
- Sense Amplifier For SRAMDocument28 pagesSense Amplifier For SRAMPrateek AgrawalNo ratings yet
- Motor Data For 32038Document1 pageMotor Data For 32038zo-kaNo ratings yet
- Pro SiteDocument887 pagesPro SiteManish SharmaNo ratings yet
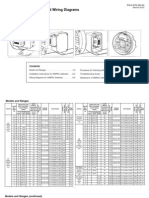
- Installation Instructions and Wiring Diagrams For All Models and RangesDocument8 pagesInstallation Instructions and Wiring Diagrams For All Models and RangesMaria MusyNo ratings yet
- Low-Power and Fast Full Adder by Exploring New and Gates: XOR XnorDocument13 pagesLow-Power and Fast Full Adder by Exploring New and Gates: XOR XnorBhargav Naidu PulugujjuNo ratings yet
- Transportation Engineering 1 Question Bank - Mumbai UniversityDocument10 pagesTransportation Engineering 1 Question Bank - Mumbai UniversityMegha Thomas0% (1)
- USAPHODocument3 pagesUSAPHOKrish KalraNo ratings yet
- Operating Manual: DW-AA4530F Atomic Absorption SpectrometerDocument147 pagesOperating Manual: DW-AA4530F Atomic Absorption Spectrometerteam engineerNo ratings yet
- Time Series QuestionsDocument1 pageTime Series QuestionsAdityNo ratings yet
- GAMESS Overview CTMC PDFDocument22 pagesGAMESS Overview CTMC PDFciwebNo ratings yet
- Vinay Sharma - inDocument3 pagesVinay Sharma - inVinay SharmaNo ratings yet
- SamsoniteDocument17 pagesSamsoniteDeepak Nayak100% (1)
- 8500c 2985Document2 pages8500c 2985Adel Khelifi100% (1)
- SKF Microlog CMXA51-IS PDFDocument4 pagesSKF Microlog CMXA51-IS PDFerikmaxramos72No ratings yet
- Rideable Segway Clone - Low Cost and Easy Build: Digital MPU6050 Accelerometer/gyro IMU BoardDocument45 pagesRideable Segway Clone - Low Cost and Easy Build: Digital MPU6050 Accelerometer/gyro IMU BoardpaolaNo ratings yet
- Vishveshwarya Technological University BELAGAVI - 590018.: A Mini Project Report OnDocument35 pagesVishveshwarya Technological University BELAGAVI - 590018.: A Mini Project Report OnSoul ReaperNo ratings yet