Download as pdf or txt
You might also like
- Lashes PDFDocument7 pagesLashes PDFsamanthaNo ratings yet
- Zac's Cutting Diet Plan: Lean ProteinDocument5 pagesZac's Cutting Diet Plan: Lean ProteinJackNo ratings yet
- Echocardiography in Hemodynamic MonitoringDocument5 pagesEchocardiography in Hemodynamic MonitoringDr.Biswajit jenaNo ratings yet
- Terapi CairanDocument5 pagesTerapi CairanZikry SitaniaNo ratings yet
- Goal-Directed Fluid Restriction During Brain Surgery: A Prospective Randomized Controlled TrialDocument7 pagesGoal-Directed Fluid Restriction During Brain Surgery: A Prospective Randomized Controlled TrialkenjiNo ratings yet
- Fluid and HemodynamicsDocument13 pagesFluid and HemodynamicsandreeaNo ratings yet
- Clinical Review: Hemodynamic Monitoring in The Intensive Care UnitDocument8 pagesClinical Review: Hemodynamic Monitoring in The Intensive Care Unitmasfak97No ratings yet
- Noninvasive Monitoring 2016Document6 pagesNoninvasive Monitoring 2016Maria LaiaNo ratings yet
- 01_Stamatakis_ReviewDocument8 pages01_Stamatakis_Reviewsanyu.warNo ratings yet
- 9) Fluid and HemodynamicsDocument13 pages9) Fluid and HemodynamicsPablo MartinezNo ratings yet
- Postoperative CareDocument15 pagesPostoperative CarelhalamNo ratings yet
- Jurding Anes AditDocument10 pagesJurding Anes Aditmaudi fitriantiNo ratings yet
- Elia Jennifer Perioperative Fluid Management andDocument19 pagesElia Jennifer Perioperative Fluid Management andSiddhartha PalaciosNo ratings yet
- Contemporary Perioperative Haemodynamic MonitoringDocument12 pagesContemporary Perioperative Haemodynamic MonitoringrjerezrNo ratings yet
- Fluid and HemodynamicsDocument13 pagesFluid and HemodynamicsJoelGámezNo ratings yet
- 10 1016@j Anclin 2020 08 004Document11 pages10 1016@j Anclin 2020 08 004Luis David Gárate CastañedaNo ratings yet
- Blood Transfusion in Anaesthesia and Critical Care: Less Is More!Document4 pagesBlood Transfusion in Anaesthesia and Critical Care: Less Is More!Maya_AnggrainiKNo ratings yet
- Hypertension Arterielle 2016Document5 pagesHypertension Arterielle 2016Nabil YahioucheNo ratings yet
- 1 s2.0 S1053077019303039 MainDocument6 pages1 s2.0 S1053077019303039 MainADELIAADENo ratings yet
- Peri Operative Blood ManagementDocument7 pagesPeri Operative Blood ManagementCarlos Garcia MonteroNo ratings yet
- A High Mean Arterial PressureDocument8 pagesA High Mean Arterial Pressureadek07No ratings yet
- Advances in Anesthesia: Optimal Perioperative Blood Pressure ManagementDocument13 pagesAdvances in Anesthesia: Optimal Perioperative Blood Pressure Managementfabian arassiNo ratings yet
- Wjem 23 358Document10 pagesWjem 23 358drsubramanianNo ratings yet
- Perioperative Patient Blood Management To Improve.19Document10 pagesPerioperative Patient Blood Management To Improve.19Reinaldi octaNo ratings yet
- 7: Effective Transfusion in Surgery and Critical CareDocument16 pages7: Effective Transfusion in Surgery and Critical CareNick-Hugh Sean WisdomNo ratings yet
- Anesthesia Considerations During Cytoreductive SurDocument9 pagesAnesthesia Considerations During Cytoreductive Surdrardigustian2986No ratings yet
- 1 s2.0 S0007091217542075 MainDocument11 pages1 s2.0 S0007091217542075 Maineny_sumaini65No ratings yet
- 10 1002@bjs 11457Document7 pages10 1002@bjs 11457maudi fitriantiNo ratings yet
- The Importance of Mean Platelet Volume To Lymphocyte Ratio in Predicting Atrial Fibrillation After Coronary Bypass OperationsDocument5 pagesThe Importance of Mean Platelet Volume To Lymphocyte Ratio in Predicting Atrial Fibrillation After Coronary Bypass OperationsM Ali AdrianNo ratings yet
- Passive Leg Raising-Induced Changes in Pulse Pressure Variation To Assess Fluid Responsiveness in Mechanically Ventilated Patients - A Multicentre Prospective Observational StudyDocument9 pagesPassive Leg Raising-Induced Changes in Pulse Pressure Variation To Assess Fluid Responsiveness in Mechanically Ventilated Patients - A Multicentre Prospective Observational Studycardionerd101No ratings yet
- Massive Hemorrhage ProtocolDocument19 pagesMassive Hemorrhage ProtocolYeseniaNo ratings yet
- CC 9070Document15 pagesCC 9070ossinNo ratings yet
- 1-s2.0-S1932227520300677Document11 pages1-s2.0-S1932227520300677Pamela Trujillo TapiaNo ratings yet
- 052018RCBCDocument6 pages052018RCBCWillian HolandaNo ratings yet
- Journal Pone 0035634Document5 pagesJournal Pone 0035634Nathaly AráuzNo ratings yet
- How To Measure Blood Pressure Using An Arterial Catheter: A Systematic 5-Step ApproachDocument10 pagesHow To Measure Blood Pressure Using An Arterial Catheter: A Systematic 5-Step ApproachdmallozziNo ratings yet
- Massive Hemorrhage ProtocolDocument19 pagesMassive Hemorrhage ProtocolJefferson Duque MartinezNo ratings yet
- Lung Ultrasound Dry WeightDocument16 pagesLung Ultrasound Dry WeightBhanu KumarNo ratings yet
- Strategies For Improving Visualization During Endoscopic Skull Base SurgeryDocument10 pagesStrategies For Improving Visualization During Endoscopic Skull Base SurgeryTi FaNo ratings yet
- 1 s2.0 S0735675721001972 MainDocument7 pages1 s2.0 S0735675721001972 MaindrsubramanianNo ratings yet
- Articulo 1Document8 pagesArticulo 1Julio Cosme CastorenaNo ratings yet
- Noninvasive Hemodynamic Monitoring in The Intensive Care UnitDocument18 pagesNoninvasive Hemodynamic Monitoring in The Intensive Care UnitmegaNo ratings yet
- Optimal Blood Pressure During CPBDocument7 pagesOptimal Blood Pressure During CPBAdy WarsanaNo ratings yet
- NICE 2010 Guidelines On VTEDocument509 pagesNICE 2010 Guidelines On VTEzaidharbNo ratings yet
- Hemodynamic Assessment in The Contemporary ICUDocument33 pagesHemodynamic Assessment in The Contemporary ICUnacxit6No ratings yet
- PIIS0007091221004359Document7 pagesPIIS0007091221004359luisfernandoamaya89No ratings yet
- Inhaled Milrinone For Pulmonary Hypertension in High-Risk Cardiac Surgery: Silver Bullet or Just Part of A Broader Management Strategy?Document6 pagesInhaled Milrinone For Pulmonary Hypertension in High-Risk Cardiac Surgery: Silver Bullet or Just Part of A Broader Management Strategy?inaNo ratings yet
- Guiding Goal-Directed TherapyDocument16 pagesGuiding Goal-Directed TherapyValeriy LevinNo ratings yet
- Use of Stepwise Lung Recruitment Maneuver To Predict Fluid Responsiveness Under Lung Protective Ventilation in The Operating RoomDocument10 pagesUse of Stepwise Lung Recruitment Maneuver To Predict Fluid Responsiveness Under Lung Protective Ventilation in The Operating RoompedromoralesacvNo ratings yet
- Harrison's Principles of Internal Medicine, Twenty-First Edition (Vol.1 & Vol.2) - Part7 - Part1Document500 pagesHarrison's Principles of Internal Medicine, Twenty-First Edition (Vol.1 & Vol.2) - Part7 - Part1Daniel CostaNo ratings yet
- s13089 022 00286 2Document11 pagess13089 022 00286 2Maudiel BrionesNo ratings yet
- Blood Pressure Variability in Surgical and Intensive Care Patients: Is There A Potential For Closed-Loop Vasopressor Administration?Document3 pagesBlood Pressure Variability in Surgical and Intensive Care Patients: Is There A Potential For Closed-Loop Vasopressor Administration?pingkyNo ratings yet
- International Consensus On Standardized Clinic Blood Pressure MeasurementDocument9 pagesInternational Consensus On Standardized Clinic Blood Pressure MeasurementElmer MoscosoNo ratings yet
- Introduction To The Postanaesthetic Care Unit: Review Open AccessDocument7 pagesIntroduction To The Postanaesthetic Care Unit: Review Open AccessSamsul BahriNo ratings yet
- Benign Paroxysmal Positional Vertigo: Opportunities SquanderedDocument8 pagesBenign Paroxysmal Positional Vertigo: Opportunities SquanderedNia UtariNo ratings yet
- Pi Is 0007091221007339Document18 pagesPi Is 0007091221007339Jeremy WongNo ratings yet
- Anestesia - Cardiovascular - Luna OrtizDocument11 pagesAnestesia - Cardiovascular - Luna OrtizWeimar Andres Bonilla MosqueraNo ratings yet
- Joacp 35 29Document6 pagesJoacp 35 29kenjiNo ratings yet
- AnastesiDocument22 pagesAnastesidhitadwynNo ratings yet
- Prone Ventilation in Acute Respiratory Distress SyndromeDocument10 pagesProne Ventilation in Acute Respiratory Distress Syndromecelma44No ratings yet
- Hemodynamic Impact of Isobaric Levobupivacaine Versus Hyperbaric Bupivacaine For Subarachnoid Anesthesia in Patients Aged 65 and Older Undergoing Hip SurgeryDocument11 pagesHemodynamic Impact of Isobaric Levobupivacaine Versus Hyperbaric Bupivacaine For Subarachnoid Anesthesia in Patients Aged 65 and Older Undergoing Hip SurgeryHana MitayaniNo ratings yet
- Essentials in Lung TransplantationFrom EverandEssentials in Lung TransplantationAllan R. GlanvilleNo ratings yet
- Social Currency: With or Without SoundDocument1 pageSocial Currency: With or Without SoundAlina MihaelaNo ratings yet
- Module 1: Human Development, Meaning, Concepts and Approaches Content OutlineDocument28 pagesModule 1: Human Development, Meaning, Concepts and Approaches Content OutlineCristine Joy CalingacionNo ratings yet
- SSRN Id2257668 PDFDocument16 pagesSSRN Id2257668 PDFDaniel Ivan Milandres100% (4)
- SH-F43 - PTW Format - R02Document2 pagesSH-F43 - PTW Format - R02vini100% (1)
- Time Management and Assessment Results of Senior High Abm StudentsDocument44 pagesTime Management and Assessment Results of Senior High Abm StudentsJustin Bidan100% (1)
- AA - 16 - Ev #4 ''Taller Safety Signs''Document6 pagesAA - 16 - Ev #4 ''Taller Safety Signs''Anny Margarita Herrera VillaNo ratings yet
- Agrahara Claim Form (English)Document14 pagesAgrahara Claim Form (English)hema160% (1)
- Psych Abnormal Child Psychology - 6th Edition (2015) - 501-550Document50 pagesPsych Abnormal Child Psychology - 6th Edition (2015) - 501-550tin_ally9059No ratings yet
- Good Governance FormatDocument16 pagesGood Governance FormatMarjonNo ratings yet
- Hi-Tech Pharmaceuticals Anavar Pill-Tablet Prohormone Supplement - Supplement WarehouseDocument1 pageHi-Tech Pharmaceuticals Anavar Pill-Tablet Prohormone Supplement - Supplement WarehouseAlfredoNo ratings yet
- One Direct Method Statement: Main Hazards Preventative MeasuresDocument5 pagesOne Direct Method Statement: Main Hazards Preventative MeasuresFaisal RazaNo ratings yet
- Chest CT Signs in Pulmonary Disease PDFDocument19 pagesChest CT Signs in Pulmonary Disease PDFpvs5155No ratings yet
- Active VFC ProvidersDocument50 pagesActive VFC ProvidersClint AnthonyNo ratings yet
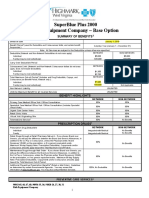
- Rish Equipment Base Plan Option Eff. 1.1.2019Document4 pagesRish Equipment Base Plan Option Eff. 1.1.2019michala anthonyNo ratings yet
- Diabetes and Detection by AstrologyDocument5 pagesDiabetes and Detection by AstrologyJatinder SandhuNo ratings yet
- The FWP in BriefDocument30 pagesThe FWP in BriefAllysonDumayag100% (1)
- ISPNO 2022 - Impact of The COVID-19 Pandemic On 30-Day Mortality and Unplanned Reoperation Rates For Pediatric Central Nervous System TumorsDocument2 pagesISPNO 2022 - Impact of The COVID-19 Pandemic On 30-Day Mortality and Unplanned Reoperation Rates For Pediatric Central Nervous System TumorsDiana SanchezNo ratings yet
- Activity STS, Gamil, Marion Claire BSN 1CDocument13 pagesActivity STS, Gamil, Marion Claire BSN 1CRenie Serrano0% (1)
- BORLAND Douglas Infuluenza PDFDocument18 pagesBORLAND Douglas Infuluenza PDFJxson GomezNo ratings yet
- Z - Data Dictionary-20200727Document4 pagesZ - Data Dictionary-20200727beef soupNo ratings yet
- Lauren Eng CV 2021Document4 pagesLauren Eng CV 2021api-386203310No ratings yet
- Alveolar Ridge AugmentationDocument23 pagesAlveolar Ridge AugmentationA ZNo ratings yet
- The Filipino Children in Prostitution: A Worst Form of Child LabourDocument41 pagesThe Filipino Children in Prostitution: A Worst Form of Child LabourDaveNo ratings yet
- Beloved: The Physical Embodiment of Psychological TraumaDocument16 pagesBeloved: The Physical Embodiment of Psychological TraumaShilpa English0060No ratings yet
- Research JD P&S ResearchDocument2 pagesResearch JD P&S ResearchAparnesh MukhopadhyayNo ratings yet
- Foundations of EpidemiologyDocument106 pagesFoundations of EpidemiologySudaysi AbdisalamNo ratings yet
- Laporan Igd Mei 2021Document12 pagesLaporan Igd Mei 2021Aris Eka KristiantoNo ratings yet
- Jeffrey DahmerDocument3 pagesJeffrey DahmerAMERICA DAYANA PORTILLO FIERRONo ratings yet