
jurnal 2 gst
jurnal 2 gst
You might also like
- AGA-DDSEP-10-Chapter-7-1653072629120 2Document34 pagesAGA-DDSEP-10-Chapter-7-1653072629120 2yyr4cdwcjdNo ratings yet
- Project Milton in Hershey, 2022Document2 pagesProject Milton in Hershey, 2022PennLiveNo ratings yet
- Cartridge List by FamilyDocument10 pagesCartridge List by Familydomi3316No ratings yet
- Donne Mie, La Fate A Tanti: From "Cosí Fan Tutte"Document13 pagesDonne Mie, La Fate A Tanti: From "Cosí Fan Tutte"Connor McCowanNo ratings yet
- Experiment ResultsDocument10 pagesExperiment ResultsArdita Rizky Putri ArcanggiNo ratings yet
- COPD TextbookDocument10 pagesCOPD Textbooknob2011nobNo ratings yet
- New Insights Into Electromagnetic Processes in HumansDocument7 pagesNew Insights Into Electromagnetic Processes in HumansmarcelogiovaneNo ratings yet
- DahoDocument29 pagesDahofodiy49587No ratings yet
- Review: Radiology of Obstructive Pulmonary DiseaseDocument13 pagesReview: Radiology of Obstructive Pulmonary DiseaseAngel IschiaNo ratings yet
- Radiology 101Document2 pagesRadiology 101Nadhirah AnandaNo ratings yet
- ChangosDocument1 pageChangostenzo_xxNo ratings yet
- Metro MapDocument1 pageMetro MapMohammed ZuhaibNo ratings yet
- BURNS Concept MapDocument1 pageBURNS Concept MapJunam DisimbanNo ratings yet
- 21900511 - 이성민 - Chapter 3 Reading SummaryDocument1 page21900511 - 이성민 - Chapter 3 Reading Summary이성민학부생No ratings yet
- Michael Romeo - Paganini Concerto in B Minor (Ver 2 by Marvin Zemanate)Document7 pagesMichael Romeo - Paganini Concerto in B Minor (Ver 2 by Marvin Zemanate)Labis Pop FlorentinNo ratings yet
- True North Project North: BOD BOD BOD BOD SHDocument8 pagesTrue North Project North: BOD BOD BOD BOD SHEbin NakarmiNo ratings yet
- Gore Et Al 2013 CT Features of Ulcerative Colitis and Crohn S DiseaseDocument25 pagesGore Et Al 2013 CT Features of Ulcerative Colitis and Crohn S DiseaseAustinNo ratings yet
- AspirationsDocument10 pagesAspirationsdr satnam kaurNo ratings yet
- Electronic Government PosterDocument1 pageElectronic Government Posterabadran100% (1)
- Revl0266 - WD Rollings Brochure - With Sticker Over ProductDocument136 pagesRevl0266 - WD Rollings Brochure - With Sticker Over ProductQue NguyenNo ratings yet
- Oral Sur 2 MidtermDocument22 pagesOral Sur 2 Midtermnapat kidsanakaraketNo ratings yet
- Untitled NotebookDocument1 pageUntitled Notebookpixisom201No ratings yet
- Trabajo Humanidades Unidad IIDocument3 pagesTrabajo Humanidades Unidad IIsergioNo ratings yet
- Parenthood: General Dynamic Factors - Age - Gender - Ethnicity - Social Economic Status - Educational BackgroundDocument1 pageParenthood: General Dynamic Factors - Age - Gender - Ethnicity - Social Economic Status - Educational Backgroundjunebug3No ratings yet
- Apparatus: DisintegrationDocument2 pagesApparatus: Disintegration-No ratings yet
- Real Life Intermediate SBDocument73 pagesReal Life Intermediate SBAnna MNo ratings yet
- Porgy & Bess (Libretto)Document26 pagesPorgy & Bess (Libretto)bplapresentacaoNo ratings yet
- Wizzair Magazine Mediakit 2022Document14 pagesWizzair Magazine Mediakit 2022RobertVasilescuNo ratings yet
- BSP1702 NotesDocument7 pagesBSP1702 NotesliyangwongNo ratings yet
- Put Campus in Your PocketDocument1 pagePut Campus in Your PocketJB BrionesNo ratings yet
- Bikes Are Permitted On Metro Buses and Metro Rail Trains. For Rules and More Information Please VisitDocument3 pagesBikes Are Permitted On Metro Buses and Metro Rail Trains. For Rules and More Information Please VisitMiguel QuinteroNo ratings yet
- Manila Ocean ParkDocument1 pageManila Ocean ParkkrllNo ratings yet
- 220802DTDG09905 Exde00 01Document1 page220802DTDG09905 Exde00 01kepuren loroNo ratings yet
- Map of AV Neighborhood CouncilDocument1 pageMap of AV Neighborhood CouncilLoriNo ratings yet
- Cardiovascular Pharmacology) 08 ACE-I - ARBs - KeyDocument1 pageCardiovascular Pharmacology) 08 ACE-I - ARBs - Keyhasanatiya41No ratings yet
- Scan 31 Mar 2023Document2 pagesScan 31 Mar 2023Jayshree YadavNo ratings yet
- CT NoteDocument17 pagesCT NoteTNP StaRkNo ratings yet
- Rock Garden: Manila Bay Dolomite BeachDocument1 pageRock Garden: Manila Bay Dolomite BeachkrllNo ratings yet
- ICT PracticalDocument4 pagesICT PracticalXyrex XNo ratings yet
- Walsh, David - Quacks, False Remedies and The Public HealthDocument68 pagesWalsh, David - Quacks, False Remedies and The Public HealthLucaNo ratings yet
- Rudolf ScoreDocument2 pagesRudolf Scorealvarogc_207923100% (1)
- Warmness On The Soul Page 2Document1 pageWarmness On The Soul Page 2venny_septania6893No ratings yet
- Waltz: From Moi Laskovyi I Nezhnyi Zver'Document1 pageWaltz: From Moi Laskovyi I Nezhnyi Zver'Anh NguyenNo ratings yet
- JGB BrochureDocument8 pagesJGB Brochureramadan rashadNo ratings yet
- Downloaded From: Bajado De/ De/ DeDocument3 pagesDownloaded From: Bajado De/ De/ DeHomero Ruiz HernandezNo ratings yet
- Blank DiagramDocument1 pageBlank Diagramxixi tNo ratings yet
- Pib Mun 2014Document198 pagesPib Mun 2014Eve MoralesNo ratings yet
- Ca 7159 enDocument1 pageCa 7159 enmmarshalzNo ratings yet
- Chique Tango Rodolfo MederosDocument2 pagesChique Tango Rodolfo MederosAlexandru Nuca100% (1)
- Recalls Hamza SurgeryDocument2 pagesRecalls Hamza SurgeryNazem Abd RaboNo ratings yet
- Concept Map #1 - Analyzing Leadership Concepts - Gil OrenseDocument1 pageConcept Map #1 - Analyzing Leadership Concepts - Gil OrenseGil OrenseNo ratings yet
- ARQUITECTONICODocument1 pageARQUITECTONICOYedani SanNo ratings yet
- MapDocument1 pageMapfalah alqagtanyNo ratings yet
- Respiration SummaryDocument1 pageRespiration SummaryXyrex XNo ratings yet
- pPYqnlFGTC2UMT6pBejw - 3004-101 Proposed PlansDocument1 pagepPYqnlFGTC2UMT6pBejw - 3004-101 Proposed PlanserniE抖音 AI Mobile Phone Based MovieNo ratings yet
- Cheat SheetDocument2 pagesCheat SheetRuth TheNo ratings yet
- BP SDEIS Comparison of 2008 & 2010 Layout - Fig - 2.8-2 Cape VincentDocument1 pageBP SDEIS Comparison of 2008 & 2010 Layout - Fig - 2.8-2 Cape VincentpandorasboxofrocksNo ratings yet
- Grieg/Solvejg's SongDocument4 pagesGrieg/Solvejg's Songshig_aokiNo ratings yet
- DHQC Cecb MB Ti Ar DW ML 02 80529Document1 pageDHQC Cecb MB Ti Ar DW ML 02 80529Kumudu PereraNo ratings yet
- Detail - B3: Typical Door Detail (SHEET 11 OF 12)Document1 pageDetail - B3: Typical Door Detail (SHEET 11 OF 12)Kumudu PereraNo ratings yet
- The GodfatherDocument1 pageThe GodfatherStambouli SohibNo ratings yet
- Padhle OPN - Nationalism in IndiaDocument1 pagePadhle OPN - Nationalism in IndiaGouri RajNo ratings yet
- Catalog of Book Publish in Burma 1877-1882Document26 pagesCatalog of Book Publish in Burma 1877-1882kerrypwlNo ratings yet
- Ot ProtocolDocument38 pagesOt ProtocolSelva KumarNo ratings yet
- Ipmat Indore 2021 PaperDocument8 pagesIpmat Indore 2021 PaperdivyanshjoshidpsjkpNo ratings yet
- Audiologist Job Description Band 5 2019Document9 pagesAudiologist Job Description Band 5 2019M LubisNo ratings yet
- Parts of An InsectDocument4 pagesParts of An InsectJohn ezekiel AntipoloNo ratings yet
- Health Surveillance Affirmative and Negative - Michigan7 2015Document323 pagesHealth Surveillance Affirmative and Negative - Michigan7 2015Davis HillNo ratings yet
- Cold Chain and Vaccine ManagementDocument20 pagesCold Chain and Vaccine Managementabdisalaan hassanNo ratings yet
- Blood and Marrow Transplant:: Resident Education Lecture SeriesDocument30 pagesBlood and Marrow Transplant:: Resident Education Lecture SeriesAparna KinginiNo ratings yet
- Introduction A&sDocument7 pagesIntroduction A&sMajaNo ratings yet
- Vsim - Edited Clinical WorksheetsDocument8 pagesVsim - Edited Clinical WorksheetsTedra FloydNo ratings yet
- Ayurvedic Medicine - Core Concept - Therapeutic Principles and PDFDocument15 pagesAyurvedic Medicine - Core Concept - Therapeutic Principles and PDFFelipe Marin100% (1)
- DG Du Diabète Type 1Document1 pageDG Du Diabète Type 1Daoud IssaNo ratings yet
- Jama Mazzone 2022 RV 210019 1641843868.64143Document10 pagesJama Mazzone 2022 RV 210019 1641843868.64143Javier RiquelmeNo ratings yet
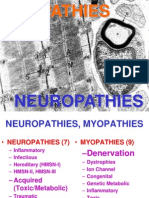
- Myopathies: NeuropathiesDocument71 pagesMyopathies: NeuropathiesmeeeenonNo ratings yet
- AbbreviationsDocument9 pagesAbbreviationsYuuki Chitose (tai-kun)No ratings yet
- SRSIReport9 27 12Document162 pagesSRSIReport9 27 12Jon CampbellNo ratings yet
- Christian Medical College VelloreDocument167 pagesChristian Medical College VelloreElisa 1209No ratings yet
- Glioma in Adults - Beyond The Basics (High-Grade)Document9 pagesGlioma in Adults - Beyond The Basics (High-Grade)Hugh Ell - auNo ratings yet
- Diet Readiness QuestionnaireDocument3 pagesDiet Readiness Questionnairesavvy_as_98100% (1)
- Human Digestive SystemDocument15 pagesHuman Digestive SystemKomalesh Theeran100% (1)
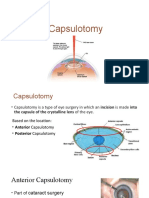
- CapsulotomyDocument15 pagesCapsulotomyAdrian PearlNo ratings yet
- Anatomy and Physiology FinalDocument2 pagesAnatomy and Physiology FinalChloé Jane Hilario100% (1)
- Fix It See and Solve The Problems of Digital Healthcare 1St Edition Thimbleby Full ChapterDocument67 pagesFix It See and Solve The Problems of Digital Healthcare 1St Edition Thimbleby Full Chapterwai.clark961100% (14)
- Luaab Bahi-Dana (Mucilage) Quince SeedsDocument3 pagesLuaab Bahi-Dana (Mucilage) Quince Seedsintikhabansari100% (1)
- Studies On The Kinetic Changes of Mixed Fruit Marmalade Developed From Lemon and OrangeDocument11 pagesStudies On The Kinetic Changes of Mixed Fruit Marmalade Developed From Lemon and OrangeRahma NusandariNo ratings yet
- Research Article: Cutaneous Mycoses Among Rice Farmers in Anambra State, NigeriaDocument6 pagesResearch Article: Cutaneous Mycoses Among Rice Farmers in Anambra State, NigeriakamalNo ratings yet
- Intro To MicrobiologyDocument31 pagesIntro To MicrobiologyLyka Durian LamosteNo ratings yet




















































































Download as pdf or txt
You might also like
- AGA-DDSEP-10-Chapter-7-1653072629120 2Document34 pagesAGA-DDSEP-10-Chapter-7-1653072629120 2yyr4cdwcjdNo ratings yet
- Project Milton in Hershey, 2022Document2 pagesProject Milton in Hershey, 2022PennLiveNo ratings yet
- Cartridge List by FamilyDocument10 pagesCartridge List by Familydomi3316No ratings yet
- Donne Mie, La Fate A Tanti: From "Cosí Fan Tutte"Document13 pagesDonne Mie, La Fate A Tanti: From "Cosí Fan Tutte"Connor McCowanNo ratings yet
- Experiment ResultsDocument10 pagesExperiment ResultsArdita Rizky Putri ArcanggiNo ratings yet
- COPD TextbookDocument10 pagesCOPD Textbooknob2011nobNo ratings yet
- New Insights Into Electromagnetic Processes in HumansDocument7 pagesNew Insights Into Electromagnetic Processes in HumansmarcelogiovaneNo ratings yet
- DahoDocument29 pagesDahofodiy49587No ratings yet
- Review: Radiology of Obstructive Pulmonary DiseaseDocument13 pagesReview: Radiology of Obstructive Pulmonary DiseaseAngel IschiaNo ratings yet
- Radiology 101Document2 pagesRadiology 101Nadhirah AnandaNo ratings yet
- ChangosDocument1 pageChangostenzo_xxNo ratings yet
- Metro MapDocument1 pageMetro MapMohammed ZuhaibNo ratings yet
- BURNS Concept MapDocument1 pageBURNS Concept MapJunam DisimbanNo ratings yet
- 21900511 - 이성민 - Chapter 3 Reading SummaryDocument1 page21900511 - 이성민 - Chapter 3 Reading Summary이성민학부생No ratings yet
- Michael Romeo - Paganini Concerto in B Minor (Ver 2 by Marvin Zemanate)Document7 pagesMichael Romeo - Paganini Concerto in B Minor (Ver 2 by Marvin Zemanate)Labis Pop FlorentinNo ratings yet
- True North Project North: BOD BOD BOD BOD SHDocument8 pagesTrue North Project North: BOD BOD BOD BOD SHEbin NakarmiNo ratings yet
- Gore Et Al 2013 CT Features of Ulcerative Colitis and Crohn S DiseaseDocument25 pagesGore Et Al 2013 CT Features of Ulcerative Colitis and Crohn S DiseaseAustinNo ratings yet
- AspirationsDocument10 pagesAspirationsdr satnam kaurNo ratings yet
- Electronic Government PosterDocument1 pageElectronic Government Posterabadran100% (1)
- Revl0266 - WD Rollings Brochure - With Sticker Over ProductDocument136 pagesRevl0266 - WD Rollings Brochure - With Sticker Over ProductQue NguyenNo ratings yet
- Oral Sur 2 MidtermDocument22 pagesOral Sur 2 Midtermnapat kidsanakaraketNo ratings yet
- Untitled NotebookDocument1 pageUntitled Notebookpixisom201No ratings yet
- Trabajo Humanidades Unidad IIDocument3 pagesTrabajo Humanidades Unidad IIsergioNo ratings yet
- Parenthood: General Dynamic Factors - Age - Gender - Ethnicity - Social Economic Status - Educational BackgroundDocument1 pageParenthood: General Dynamic Factors - Age - Gender - Ethnicity - Social Economic Status - Educational Backgroundjunebug3No ratings yet
- Apparatus: DisintegrationDocument2 pagesApparatus: Disintegration-No ratings yet
- Real Life Intermediate SBDocument73 pagesReal Life Intermediate SBAnna MNo ratings yet
- Porgy & Bess (Libretto)Document26 pagesPorgy & Bess (Libretto)bplapresentacaoNo ratings yet
- Wizzair Magazine Mediakit 2022Document14 pagesWizzair Magazine Mediakit 2022RobertVasilescuNo ratings yet
- BSP1702 NotesDocument7 pagesBSP1702 NotesliyangwongNo ratings yet
- Put Campus in Your PocketDocument1 pagePut Campus in Your PocketJB BrionesNo ratings yet
- Bikes Are Permitted On Metro Buses and Metro Rail Trains. For Rules and More Information Please VisitDocument3 pagesBikes Are Permitted On Metro Buses and Metro Rail Trains. For Rules and More Information Please VisitMiguel QuinteroNo ratings yet
- Manila Ocean ParkDocument1 pageManila Ocean ParkkrllNo ratings yet
- 220802DTDG09905 Exde00 01Document1 page220802DTDG09905 Exde00 01kepuren loroNo ratings yet
- Map of AV Neighborhood CouncilDocument1 pageMap of AV Neighborhood CouncilLoriNo ratings yet
- Cardiovascular Pharmacology) 08 ACE-I - ARBs - KeyDocument1 pageCardiovascular Pharmacology) 08 ACE-I - ARBs - Keyhasanatiya41No ratings yet
- Scan 31 Mar 2023Document2 pagesScan 31 Mar 2023Jayshree YadavNo ratings yet
- CT NoteDocument17 pagesCT NoteTNP StaRkNo ratings yet
- Rock Garden: Manila Bay Dolomite BeachDocument1 pageRock Garden: Manila Bay Dolomite BeachkrllNo ratings yet
- ICT PracticalDocument4 pagesICT PracticalXyrex XNo ratings yet
- Walsh, David - Quacks, False Remedies and The Public HealthDocument68 pagesWalsh, David - Quacks, False Remedies and The Public HealthLucaNo ratings yet
- Rudolf ScoreDocument2 pagesRudolf Scorealvarogc_207923100% (1)
- Warmness On The Soul Page 2Document1 pageWarmness On The Soul Page 2venny_septania6893No ratings yet
- Waltz: From Moi Laskovyi I Nezhnyi Zver'Document1 pageWaltz: From Moi Laskovyi I Nezhnyi Zver'Anh NguyenNo ratings yet
- JGB BrochureDocument8 pagesJGB Brochureramadan rashadNo ratings yet
- Downloaded From: Bajado De/ De/ DeDocument3 pagesDownloaded From: Bajado De/ De/ DeHomero Ruiz HernandezNo ratings yet
- Blank DiagramDocument1 pageBlank Diagramxixi tNo ratings yet
- Pib Mun 2014Document198 pagesPib Mun 2014Eve MoralesNo ratings yet
- Ca 7159 enDocument1 pageCa 7159 enmmarshalzNo ratings yet
- Chique Tango Rodolfo MederosDocument2 pagesChique Tango Rodolfo MederosAlexandru Nuca100% (1)
- Recalls Hamza SurgeryDocument2 pagesRecalls Hamza SurgeryNazem Abd RaboNo ratings yet
- Concept Map #1 - Analyzing Leadership Concepts - Gil OrenseDocument1 pageConcept Map #1 - Analyzing Leadership Concepts - Gil OrenseGil OrenseNo ratings yet
- ARQUITECTONICODocument1 pageARQUITECTONICOYedani SanNo ratings yet
- MapDocument1 pageMapfalah alqagtanyNo ratings yet
- Respiration SummaryDocument1 pageRespiration SummaryXyrex XNo ratings yet
- pPYqnlFGTC2UMT6pBejw - 3004-101 Proposed PlansDocument1 pagepPYqnlFGTC2UMT6pBejw - 3004-101 Proposed PlanserniE抖音 AI Mobile Phone Based MovieNo ratings yet
- Cheat SheetDocument2 pagesCheat SheetRuth TheNo ratings yet
- BP SDEIS Comparison of 2008 & 2010 Layout - Fig - 2.8-2 Cape VincentDocument1 pageBP SDEIS Comparison of 2008 & 2010 Layout - Fig - 2.8-2 Cape VincentpandorasboxofrocksNo ratings yet
- Grieg/Solvejg's SongDocument4 pagesGrieg/Solvejg's Songshig_aokiNo ratings yet
- DHQC Cecb MB Ti Ar DW ML 02 80529Document1 pageDHQC Cecb MB Ti Ar DW ML 02 80529Kumudu PereraNo ratings yet
- Detail - B3: Typical Door Detail (SHEET 11 OF 12)Document1 pageDetail - B3: Typical Door Detail (SHEET 11 OF 12)Kumudu PereraNo ratings yet
- The GodfatherDocument1 pageThe GodfatherStambouli SohibNo ratings yet
- Padhle OPN - Nationalism in IndiaDocument1 pagePadhle OPN - Nationalism in IndiaGouri RajNo ratings yet
- Catalog of Book Publish in Burma 1877-1882Document26 pagesCatalog of Book Publish in Burma 1877-1882kerrypwlNo ratings yet
- Ot ProtocolDocument38 pagesOt ProtocolSelva KumarNo ratings yet
- Ipmat Indore 2021 PaperDocument8 pagesIpmat Indore 2021 PaperdivyanshjoshidpsjkpNo ratings yet
- Audiologist Job Description Band 5 2019Document9 pagesAudiologist Job Description Band 5 2019M LubisNo ratings yet
- Parts of An InsectDocument4 pagesParts of An InsectJohn ezekiel AntipoloNo ratings yet
- Health Surveillance Affirmative and Negative - Michigan7 2015Document323 pagesHealth Surveillance Affirmative and Negative - Michigan7 2015Davis HillNo ratings yet
- Cold Chain and Vaccine ManagementDocument20 pagesCold Chain and Vaccine Managementabdisalaan hassanNo ratings yet
- Blood and Marrow Transplant:: Resident Education Lecture SeriesDocument30 pagesBlood and Marrow Transplant:: Resident Education Lecture SeriesAparna KinginiNo ratings yet
- Introduction A&sDocument7 pagesIntroduction A&sMajaNo ratings yet
- Vsim - Edited Clinical WorksheetsDocument8 pagesVsim - Edited Clinical WorksheetsTedra FloydNo ratings yet
- Ayurvedic Medicine - Core Concept - Therapeutic Principles and PDFDocument15 pagesAyurvedic Medicine - Core Concept - Therapeutic Principles and PDFFelipe Marin100% (1)
- DG Du Diabète Type 1Document1 pageDG Du Diabète Type 1Daoud IssaNo ratings yet
- Jama Mazzone 2022 RV 210019 1641843868.64143Document10 pagesJama Mazzone 2022 RV 210019 1641843868.64143Javier RiquelmeNo ratings yet
- Myopathies: NeuropathiesDocument71 pagesMyopathies: NeuropathiesmeeeenonNo ratings yet
- AbbreviationsDocument9 pagesAbbreviationsYuuki Chitose (tai-kun)No ratings yet
- SRSIReport9 27 12Document162 pagesSRSIReport9 27 12Jon CampbellNo ratings yet
- Christian Medical College VelloreDocument167 pagesChristian Medical College VelloreElisa 1209No ratings yet
- Glioma in Adults - Beyond The Basics (High-Grade)Document9 pagesGlioma in Adults - Beyond The Basics (High-Grade)Hugh Ell - auNo ratings yet
- Diet Readiness QuestionnaireDocument3 pagesDiet Readiness Questionnairesavvy_as_98100% (1)
- Human Digestive SystemDocument15 pagesHuman Digestive SystemKomalesh Theeran100% (1)
- CapsulotomyDocument15 pagesCapsulotomyAdrian PearlNo ratings yet
- Anatomy and Physiology FinalDocument2 pagesAnatomy and Physiology FinalChloé Jane Hilario100% (1)
- Fix It See and Solve The Problems of Digital Healthcare 1St Edition Thimbleby Full ChapterDocument67 pagesFix It See and Solve The Problems of Digital Healthcare 1St Edition Thimbleby Full Chapterwai.clark961100% (14)
- Luaab Bahi-Dana (Mucilage) Quince SeedsDocument3 pagesLuaab Bahi-Dana (Mucilage) Quince Seedsintikhabansari100% (1)
- Studies On The Kinetic Changes of Mixed Fruit Marmalade Developed From Lemon and OrangeDocument11 pagesStudies On The Kinetic Changes of Mixed Fruit Marmalade Developed From Lemon and OrangeRahma NusandariNo ratings yet
- Research Article: Cutaneous Mycoses Among Rice Farmers in Anambra State, NigeriaDocument6 pagesResearch Article: Cutaneous Mycoses Among Rice Farmers in Anambra State, NigeriakamalNo ratings yet
- Intro To MicrobiologyDocument31 pagesIntro To MicrobiologyLyka Durian LamosteNo ratings yet