Download as pdf or txt
You might also like
- The Sadhana of Buddha AkshobhyaDocument22 pagesThe Sadhana of Buddha AkshobhyaNilo Gelais Costa Junior100% (5)
- TDS-11SA Service Manual PDFDocument236 pagesTDS-11SA Service Manual PDFBoris Zaslichko88% (34)
- ECA1 Tests Language Test 2A New2018Document4 pagesECA1 Tests Language Test 2A New2018Anita Cyran100% (1)
- Pediatrics in Review. Dehydration 2015Document14 pagesPediatrics in Review. Dehydration 2015Jorge Eduardo Espinoza Rios100% (2)
- TO Improve Sales at Café Coffee Day PROJECT REPORTDocument85 pagesTO Improve Sales at Café Coffee Day PROJECT REPORTBabasab Patil (Karrisatte)75% (4)
- 1 1 An Overview of Communication Skills in EnglishDocument11 pages1 1 An Overview of Communication Skills in EnglishBARIBOR SHADRACH100% (7)
- NCBI Bookshelf-Diabetes InsipidusDocument44 pagesNCBI Bookshelf-Diabetes InsipidusDiah Pradnya ParamitaNo ratings yet
- Diagnosis of Polyuria and Diabetes Insipidus - UP To DATEDocument15 pagesDiagnosis of Polyuria and Diabetes Insipidus - UP To DATELuis Fernando Arias VillalobosNo ratings yet
- Diabetes InsipidusDocument5 pagesDiabetes InsipidusFazalJaturieNo ratings yet
- Diabetesinsipidus: An UpdateDocument15 pagesDiabetesinsipidus: An UpdateErikaNo ratings yet
- Diabetes Insipidus HandoutDocument4 pagesDiabetes Insipidus HandoutllianNo ratings yet
- Diabetes InsipidusDocument4 pagesDiabetes Insipidusshelly_shellyNo ratings yet
- D InsipidaDocument3 pagesD InsipidaAndrea Valenzuela AedoNo ratings yet
- Diabetes InsipidusDocument18 pagesDiabetes InsipidusElena Patricia GonzálezNo ratings yet
- Diabetes InsipidusDocument14 pagesDiabetes InsipidusTom BiusoNo ratings yet
- Deficiencies of Vasopressin Secretion and ActionDocument71 pagesDeficiencies of Vasopressin Secretion and Actionbiniam MesfinNo ratings yet
- Diabetes InsipidusDocument7 pagesDiabetes Insipiduspaul_stefenson10No ratings yet
- Diabetes INSIPIDUSDocument6 pagesDiabetes INSIPIDUSavinash dhameriya100% (1)
- Case Report - Diabetes InsipidusDocument4 pagesCase Report - Diabetes InsipidusSACHI DANIELLA TATOYNo ratings yet
- Water MetabolismDocument13 pagesWater MetabolismarmyNo ratings yet
- Diabetes Insipidus and SIADHDocument14 pagesDiabetes Insipidus and SIADHHernando CastrillónNo ratings yet
- What's To Know About Diabetes Insipidus?: Last Updated Fri 19 January 2018 byDocument5 pagesWhat's To Know About Diabetes Insipidus?: Last Updated Fri 19 January 2018 byCindy Mae Flores UtlegNo ratings yet
- Pediatric Diabetes InsipidusDocument11 pagesPediatric Diabetes InsipidusVictor Matias BarriosNo ratings yet
- Diabetes InsipidusDocument12 pagesDiabetes InsipidusAbhijeetNo ratings yet
- Sands PDFDocument10 pagesSands PDFAsmaulKhusnaNo ratings yet
- PamphletDocument1 pagePamphletAldenn MinotaurNo ratings yet
- Research Paper On Diabetes InsipidusDocument5 pagesResearch Paper On Diabetes Insipidusfypikovekef2100% (1)
- Nephrogenic Diabetes InsipidusDocument10 pagesNephrogenic Diabetes InsipidusJapheth SalvanNo ratings yet
- Diabetes Insipidus1Document29 pagesDiabetes Insipidus1Zanida ZainonNo ratings yet
- Sonia Nabila (P17220194050) Artikel B.InggrisDocument10 pagesSonia Nabila (P17220194050) Artikel B.InggrisSonia NabilaNo ratings yet
- Diabetes InsipidaDocument15 pagesDiabetes Insipidapaulito_delgadoNo ratings yet
- Hyperglycemic Hyperosmolar Nonketotic Syndrome: R. Venkatraman and Sunit C. SinghiDocument6 pagesHyperglycemic Hyperosmolar Nonketotic Syndrome: R. Venkatraman and Sunit C. Singhisharu4291No ratings yet
- Diabetes InsidipusDocument2 pagesDiabetes InsidipusLena RoweNo ratings yet
- Case Report ..Document69 pagesCase Report ..sashadilanNo ratings yet
- Juraj Artner - Cancer and Neoplasia FactsheetDocument11 pagesJuraj Artner - Cancer and Neoplasia FactsheetBogdan SoltuzuNo ratings yet
- Pediatrics in Review 2013 HiponatremiaDocument5 pagesPediatrics in Review 2013 HiponatremiaCarlos Elio Polo Vargas100% (1)
- DehydrationDocument17 pagesDehydrationLaura Anghel-MocanuNo ratings yet
- DeshidratacionpedDocument6 pagesDeshidratacionpedKaren Alejandra RiveraNo ratings yet
- DeshidratacionDocument14 pagesDeshidratacionAlvaro Andres Flores JimenezNo ratings yet
- Dehydration Isonatremic, Hyponatremic, andDocument15 pagesDehydration Isonatremic, Hyponatremic, andalfredoibcNo ratings yet
- Fluid and ElectrolytesDocument135 pagesFluid and ElectrolytesLindsay PinedaNo ratings yet
- Refardt 2020Document14 pagesRefardt 2020ushNo ratings yet
- NCP CKD From CaneDocument74 pagesNCP CKD From CaneSheela Khrystyn LeeNo ratings yet
- What Is Diabetes InsipidusDocument16 pagesWhat Is Diabetes InsipidusllianNo ratings yet
- Jurnal Geriatri Dr. BrinnaDocument12 pagesJurnal Geriatri Dr. Brinnabrinna aninditaNo ratings yet
- Case Study 12Document7 pagesCase Study 12Steve MizzoNo ratings yet
- 02 Iajps02052023Document10 pages02 Iajps02052023ruchiNo ratings yet
- Diabetes Insipidus: Pathogenesis, Diagnosis, and Clinical ManagementDocument13 pagesDiabetes Insipidus: Pathogenesis, Diagnosis, and Clinical Managementputrirahayu srikandiNo ratings yet
- Tipo InsipidaDocument9 pagesTipo InsipidaNegro SoyNo ratings yet
- Ispad DkaDocument48 pagesIspad DkaJisaNo ratings yet
- Diabetes Insipidus: Done By: Farah Suhimat Sereen MajaliDocument23 pagesDiabetes Insipidus: Done By: Farah Suhimat Sereen Majaliraed faisalNo ratings yet
- HHS TreatmentDocument12 pagesHHS TreatmentJoshua TompulNo ratings yet
- Hockenberry: Wong's Essentials of Pediatric Nursing, 9th EditionDocument3 pagesHockenberry: Wong's Essentials of Pediatric Nursing, 9th EditionSNo ratings yet
- DIABETES CorrectedDocument16 pagesDIABETES CorrectedBlaise PascalNo ratings yet
- Hyponatremia and Hypernatremia in The ElderlyDocument15 pagesHyponatremia and Hypernatremia in The ElderlyStacey WoodsNo ratings yet
- Nephrotic Syndrome FinalDocument5 pagesNephrotic Syndrome FinalAaron AntonioNo ratings yet
- Hypernatremia: Hypernatremia Is Defined As A Plasma Na+ Concentration 145 Mmol/lDocument13 pagesHypernatremia: Hypernatremia Is Defined As A Plasma Na+ Concentration 145 Mmol/ltamir14No ratings yet
- KMB Diabetes InsipidusDocument24 pagesKMB Diabetes InsipidusNur Rofikoh Bil Karomah100% (1)
- Asymptomatic Hyperuricemia: To Treat or Not To Treat: ReviewDocument8 pagesAsymptomatic Hyperuricemia: To Treat or Not To Treat: ReviewkkichaNo ratings yet
- Kidney18 407Document4 pagesKidney18 407api-240473826No ratings yet
- Diabetes InsipidusDocument17 pagesDiabetes InsipidusSan Siddz100% (2)
- Medical Surgical Fluid and Electrolytes FVD FVEDocument7 pagesMedical Surgical Fluid and Electrolytes FVD FVEMichaelaKatrinaTrinidadNo ratings yet
- Lab 5 Diabetes InsipidusDocument6 pagesLab 5 Diabetes InsipidusLisa EkapratiwiNo ratings yet
- DiabetesDocument1 pageDiabetesSantiagoNo ratings yet
- Hypoglycemia in Diabetes: Pathophysiology, Prevalence, and PreventionFrom EverandHypoglycemia in Diabetes: Pathophysiology, Prevalence, and PreventionNo ratings yet
- Gis Prac1Document126 pagesGis Prac1Brijesh JavakeNo ratings yet
- Baked Salmon SushiDocument2 pagesBaked Salmon Sushivetsnsr71No ratings yet
- Infinitigeneralcatalog Compressed (1) CompressedDocument31 pagesInfinitigeneralcatalog Compressed (1) CompressedBilher SihombingNo ratings yet
- 2 Functional AnalysisDocument17 pages2 Functional AnalysisnidhiNo ratings yet
- Pathway To English Peminatan 3 Bab 3Document9 pagesPathway To English Peminatan 3 Bab 3Agung PrasetyoNo ratings yet
- Steckel Mill 1 PDFDocument178 pagesSteckel Mill 1 PDFSomnathNaskarNo ratings yet
- Speed Control of DC Motor Using Fuzzy PID ControllerDocument15 pagesSpeed Control of DC Motor Using Fuzzy PID Controllerthhluong.sdh232No ratings yet
- Storage Regulations For Petroleum ProductsDocument3 pagesStorage Regulations For Petroleum ProductsSaumyaChandraNo ratings yet
- Stress Concentrations at Holes in Thin Rotating Discs: ANG L. TANDocument3 pagesStress Concentrations at Holes in Thin Rotating Discs: ANG L. TANKris SmaczekNo ratings yet
- Solutions l4 Chemistry Class 12 Cbse by Ashu SirDocument16 pagesSolutions l4 Chemistry Class 12 Cbse by Ashu Sirvedantu495No ratings yet
- Lab 1a RASPlib Installation Instructions R5 2016b-2017aDocument10 pagesLab 1a RASPlib Installation Instructions R5 2016b-2017aaleNo ratings yet
- Petroleum Act 1934 SlidesDocument7 pagesPetroleum Act 1934 SlidesHamza Masood100% (1)
- Digital Fundamentals: FloydDocument17 pagesDigital Fundamentals: FloydadilNo ratings yet
- Aquatic ActivitiesDocument21 pagesAquatic ActivitiesJames Baryl GarceloNo ratings yet
- Techciti: Managed ServicesDocument6 pagesTechciti: Managed ServicesTechciti TechnologiesNo ratings yet
- SHS Core - Reading and Writing CG PDFDocument8 pagesSHS Core - Reading and Writing CG PDFRoy Ivan Manuel Reyes67% (6)
- Invitation Accp 2011Document5 pagesInvitation Accp 2011Klub 'Apoteker' IndonesiaNo ratings yet
- ME - Paper 3 - Part B1 - Data FileDocument12 pagesME - Paper 3 - Part B1 - Data Filemmontagne1No ratings yet
- 1 Microbiology Course ContentDocument16 pages1 Microbiology Course ContentAziz AnisahNo ratings yet
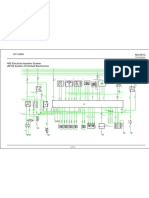
- Circuit Diagram: Ecu A/7Document1 pageCircuit Diagram: Ecu A/7RubénNo ratings yet
- Evidence DraftDocument15 pagesEvidence DraftAishwarya1312No ratings yet
- Chapter-9-Soil VIIDocument8 pagesChapter-9-Soil VIIPreeti BansalNo ratings yet
- BodasurudabixDocument3 pagesBodasurudabixtom.quang6112No ratings yet
- Gradsaleh PDFDocument257 pagesGradsaleh PDFميرفت بكرى نمرNo ratings yet
- Geologic Time Scale IndonesiaDocument1 pageGeologic Time Scale IndonesiasyariefiqbalNo ratings yet