
Article
Article
You might also like
- Ann Rev Balic Et Al FinalDocument14 pagesAnn Rev Balic Et Al FinalFreddy A. ManayayNo ratings yet
- Liquid Biopsy From Discovery To Clinical ImplementationDocument5 pagesLiquid Biopsy From Discovery To Clinical ImplementationLais BritoNo ratings yet
- Mehta Et Al-2018-American Journal of TransplantationDocument8 pagesMehta Et Al-2018-American Journal of Transplantationpaul00040No ratings yet
- 33Document11 pages33Joana KellenNo ratings yet
- 10 Rosenberg Vitamin CDocument78 pages10 Rosenberg Vitamin CЩербакова ЛенаNo ratings yet
- Referensi 1Document9 pagesReferensi 1Indah Syaidatul MNo ratings yet
- 10 0000@ncbi NLM Nih gov@PMC6325475Document10 pages10 0000@ncbi NLM Nih gov@PMC6325475Tengku AdriansyahNo ratings yet
- Development of Prognostic Signatures For Intermediate Risk Papillary Thyroid CancerDocument12 pagesDevelopment of Prognostic Signatures For Intermediate Risk Papillary Thyroid Cancernfp.panjaitanNo ratings yet
- Brock Et Al Liquid Biopsy 2015Document11 pagesBrock Et Al Liquid Biopsy 2015Jean BiverNo ratings yet
- Fact de Pet n2Document6 pagesFact de Pet n2Pedro ChantaNo ratings yet
- Tiroides ArticuloDocument9 pagesTiroides Articulojuan sebaastianNo ratings yet
- DetectionDocument9 pagesDetectionHarshvardhan RavalNo ratings yet
- Vera2020 Article MultidisciplinaryManagementOfLDocument16 pagesVera2020 Article MultidisciplinaryManagementOfLDiego Andres VasquezNo ratings yet
- Nanotechnology and CancerDocument16 pagesNanotechnology and CancerMarcos LoredoNo ratings yet
- 8424365Document8 pages8424365Melody CyyNo ratings yet
- Epidemiology and Factors Related To The Survival of Metastatic Kidney Cancers: Retrospective Study at The Mohamed VI Center For The Cancer Treatment in Casablanca, MoroccoDocument5 pagesEpidemiology and Factors Related To The Survival of Metastatic Kidney Cancers: Retrospective Study at The Mohamed VI Center For The Cancer Treatment in Casablanca, MoroccoInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Imun PDFDocument4 pagesImun PDFLeyni SabatiniNo ratings yet
- 10 1002@cam4 2286Document11 pages10 1002@cam4 2286Ricardo MarquesNo ratings yet
- Assessment of Tumor Infiltrating Lymphocytes Using.12Document9 pagesAssessment of Tumor Infiltrating Lymphocytes Using.12Muhammad Rifki100% (1)
- The Role of Automated Cytometry in The New Era of Cancer Immunotherapy (Review)Document7 pagesThe Role of Automated Cytometry in The New Era of Cancer Immunotherapy (Review)Andrea SbranaNo ratings yet
- Risk Factors For Brain Metastasis-Colocerctal CancerDocument8 pagesRisk Factors For Brain Metastasis-Colocerctal CancerIstianah SakdullahNo ratings yet
- 408 2020 Article 407Document11 pages408 2020 Article 407CuchuluuNo ratings yet
- CA MammaeDocument6 pagesCA MammaeRiaNo ratings yet
- Int J Lab Hematology - 2017 - Galtseva - Minimal Residual Disease in Multiple Myeloma Benefits of Flow CytometryDocument9 pagesInt J Lab Hematology - 2017 - Galtseva - Minimal Residual Disease in Multiple Myeloma Benefits of Flow CytometrymatanhibNo ratings yet
- Jurnal Radiologi 2Document21 pagesJurnal Radiologi 2Adelya Dwi AsyifaNo ratings yet
- Research ArticleDocument7 pagesResearch ArticleZakia DrajatNo ratings yet
- Prognostic Indicators in Differentiated Thyroid Carcinoma: Diana S. Dean, MD, and Ian D. Hay, MB, PHD, FRCPDocument11 pagesPrognostic Indicators in Differentiated Thyroid Carcinoma: Diana S. Dean, MD, and Ian D. Hay, MB, PHD, FRCPEndang Rahayu Fuji LestaryNo ratings yet
- Ijbsv 16 P 1551Document12 pagesIjbsv 16 P 1551Flip Flop ChartNo ratings yet
- 0 Ba 2Document14 pages0 Ba 2faraz.mirza1No ratings yet
- Single Tube Liquid Biopsy For Advanced Non-Small Cell Lung CancerDocument11 pagesSingle Tube Liquid Biopsy For Advanced Non-Small Cell Lung CancerBikash Ranjan SamalNo ratings yet
- 1 s2.0 S1936523320303995 MainDocument10 pages1 s2.0 S1936523320303995 MainNoman M HasanNo ratings yet
- Circulating Tumor DNA and Radiological Tumor VolumDocument7 pagesCirculating Tumor DNA and Radiological Tumor Volumnaomireyes01No ratings yet
- MicroRNA-based Risk Scoring System To Identify EarDocument14 pagesMicroRNA-based Risk Scoring System To Identify EarDavidNo ratings yet
- TNBC PMRTDocument7 pagesTNBC PMRTMed MedNo ratings yet
- Neoadjuvant Treatment For Newly Diagnosed Advanced Ovarian Cancer. 2020Document9 pagesNeoadjuvant Treatment For Newly Diagnosed Advanced Ovarian Cancer. 2020Prodromos KoutoukoglouNo ratings yet
- Warde 2002Document5 pagesWarde 2002Bruno AlanNo ratings yet
- 10.thyroid Cancer TumorigenesisDocument18 pages10.thyroid Cancer TumorigenesisAccounting CV BakerNo ratings yet
- Atm 07 14 323Document9 pagesAtm 07 14 323Ethel GeanNo ratings yet
- The Use and Efficacy of Chemotherapy and Radiotherapy in Children and Adults With Pilocytic AstrocytomaDocument9 pagesThe Use and Efficacy of Chemotherapy and Radiotherapy in Children and Adults With Pilocytic AstrocytomaAlejandro Zurita SaáNo ratings yet
- Oyad006 PDFDocument2 pagesOyad006 PDFRaul Matute MartinNo ratings yet
- Pantel EA - 2012 - Circulating Cancer Cells and DNA - V2Document20 pagesPantel EA - 2012 - Circulating Cancer Cells and DNA - V2Clark Xingzhi ZhangNo ratings yet
- DTH 34 E14981Document9 pagesDTH 34 E14981Henry WijayaNo ratings yet
- Metastatic Hepatocellular Carcinoma Diagnosed by Fine Needle Aspiration: A Clinical and Cytologic StudyDocument6 pagesMetastatic Hepatocellular Carcinoma Diagnosed by Fine Needle Aspiration: A Clinical and Cytologic StudyMara PitrezNo ratings yet
- 11 Preoperative - High - Neutrophil-Lymphocyte - Ratio - MayDocument8 pages11 Preoperative - High - Neutrophil-Lymphocyte - Ratio - MayBridia BogarNo ratings yet
- Plasma MesothelinDocument7 pagesPlasma Mesothelinpaulo saNo ratings yet
- 1 s2.0 S0748798324003974 MainDocument1 page1 s2.0 S0748798324003974 MainShahnaz AhmedNo ratings yet
- International Journal of Scientific Research: OncologyDocument4 pagesInternational Journal of Scientific Research: OncologyRaul Matute MartinNo ratings yet
- 2013 Predicting Lymph Node Metastases in Early Rectal CancerDocument5 pages2013 Predicting Lymph Node Metastases in Early Rectal CancerjohnnhekoNo ratings yet
- Mir-155-5P Modulates Malignant Behaviors Of Hepatocellular Carcinoma By Directly Targeting Cthrc1 And Indirectly Regulating Gsk-3Β-Involved Wnt/Β-Catenin SignalingDocument12 pagesMir-155-5P Modulates Malignant Behaviors Of Hepatocellular Carcinoma By Directly Targeting Cthrc1 And Indirectly Regulating Gsk-3Β-Involved Wnt/Β-Catenin SignalingDeedee RenovaldiNo ratings yet
- Atm 08 20 1292Document11 pagesAtm 08 20 1292Ethel GeanNo ratings yet
- Church 2015Document1 pageChurch 2015TrabelsiNo ratings yet
- The Significance of Neutrophil/lymphocyte Ratio As A Possible Marker of Underlying Papillary Microcarcinomas in Thyroidal Goiters: A Pilot StudyDocument6 pagesThe Significance of Neutrophil/lymphocyte Ratio As A Possible Marker of Underlying Papillary Microcarcinomas in Thyroidal Goiters: A Pilot StudyagusNo ratings yet
- Liquid BiopsyDocument2 pagesLiquid BiopsySalman MajidNo ratings yet
- Radiotherapy and OncologyDocument6 pagesRadiotherapy and OncologyIntan Kartika NursyahbaniNo ratings yet
- Extracellular Nucleic Acids and Cancer: Michael - Fleischhacker@uk-Halle - de Bernd - Schmidt@uk-Halle - deDocument55 pagesExtracellular Nucleic Acids and Cancer: Michael - Fleischhacker@uk-Halle - de Bernd - Schmidt@uk-Halle - deAirin LeonieNo ratings yet
- Characterization of Adrenal Metastatic Cancer Using FDG PET CTDocument8 pagesCharacterization of Adrenal Metastatic Cancer Using FDG PET CTEngky ChristianNo ratings yet
- AlbaBernal ChallengesAndDocument10 pagesAlbaBernal ChallengesAndKhairul ScNo ratings yet
- The Journal of Pathology CR - 2024 - Knight - The Glasgow Microenvironment Score An Exemplar of Contemporary BiomarkerDocument16 pagesThe Journal of Pathology CR - 2024 - Knight - The Glasgow Microenvironment Score An Exemplar of Contemporary Biomarkerenrichedenlightenment05No ratings yet
- 10 1016@j Ejso 2020 03 188Document1 page10 1016@j Ejso 2020 03 188Andrіі DudashNo ratings yet
- 20.01.2024 Seating PlanDocument6 pages20.01.2024 Seating PlanPericherla Rakesh varmaNo ratings yet
- RMO 2016 Detailed AnalysisDocument6 pagesRMO 2016 Detailed AnalysisSaksham HoodaNo ratings yet
- Assessing The Feasibility of A New Venture 1.1 Assessment and Evaluation of Entrepreneurial OpportunitiesDocument13 pagesAssessing The Feasibility of A New Venture 1.1 Assessment and Evaluation of Entrepreneurial OpportunitiesBereket Desalegn100% (1)
- Cincinnati Retirement System Update: March 28, 2022Document24 pagesCincinnati Retirement System Update: March 28, 2022WVXU NewsNo ratings yet
- From Rice To Apple-Pear Style - An Ecocritical Approach To China's Korean Ethnic MinorityDocument14 pagesFrom Rice To Apple-Pear Style - An Ecocritical Approach To China's Korean Ethnic MinorityLing LIUNo ratings yet
- Product Risk Management Report For Spine ProductsDocument25 pagesProduct Risk Management Report For Spine ProductsAlejandro Landinez100% (1)
- Bio Drosophilia Mini Project 2 1Document15 pagesBio Drosophilia Mini Project 2 1jocyeo0% (1)
- Tc3yf en Manual 170905 He PDFDocument1 pageTc3yf en Manual 170905 He PDFJuan Manuel EscorihuelaNo ratings yet
- A Burdizzo Is Used For: A. Branding B. Dehorning C. Castration D. All of The AboveDocument54 pagesA Burdizzo Is Used For: A. Branding B. Dehorning C. Castration D. All of The AboveMac Dwayne CarpesoNo ratings yet
- PMP Exam EVOVLE Free SampleDocument47 pagesPMP Exam EVOVLE Free SampleEvolve trainingmaterialsNo ratings yet
- Revised 04/01/2021Document33 pagesRevised 04/01/2021Kim PowellNo ratings yet
- VarahamihiraDocument6 pagesVarahamihiraSTAR GROUPS100% (1)
- Suraj Estate Developers Limited RHPDocument532 pagesSuraj Estate Developers Limited RHPJerry SinghNo ratings yet
- Nunez v. Sec - y of HHS - 2019 U.S. Claims LEXIS 644Document40 pagesNunez v. Sec - y of HHS - 2019 U.S. Claims LEXIS 644Kirk HartleyNo ratings yet
- ASR 2020 J2Prelim H2Chem P4 QP PDFDocument20 pagesASR 2020 J2Prelim H2Chem P4 QP PDFchuasioklengNo ratings yet
- Biostat IntroductionDocument31 pagesBiostat IntroductionteklayNo ratings yet
- اختبار الوزن النوعي و امتصاص الماء لركامDocument78 pagesاختبار الوزن النوعي و امتصاص الماء لركامحسين المهندسNo ratings yet
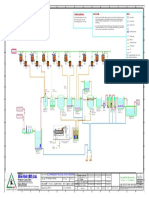
- Alim Knit (BD) LTD.: Recommended Process Flow DiagramDocument1 pageAlim Knit (BD) LTD.: Recommended Process Flow DiagramKamrul HasanNo ratings yet
- التحليل المكاني والوظيفي للخدمات التعليمية في مدينة سوران باستخدام نظم المعلومات الجغرافية- عمر حسن حسين رواندزي- ماجستيرDocument178 pagesالتحليل المكاني والوظيفي للخدمات التعليمية في مدينة سوران باستخدام نظم المعلومات الجغرافية- عمر حسن حسين رواندزي- ماجستيرMahmoud Abdelrahman86% (7)
- Material ManagementDocument20 pagesMaterial Managementgkataria110100% (1)
- SSC Gr10 ICT Q4 Module 2 WK 2 - v.01-CC-released-7June2021Document16 pagesSSC Gr10 ICT Q4 Module 2 WK 2 - v.01-CC-released-7June2021Vj AleserNo ratings yet
- Recounttext 160409104911Document9 pagesRecounttext 160409104911Anif Ough GtuwNo ratings yet
- Botech. IDocument37 pagesBotech. IKevin Rose BarnuevoNo ratings yet
- Achieving Success Through Effective Business CommunicationDocument36 pagesAchieving Success Through Effective Business Communicationfaizankhan23No ratings yet
- HP Catalogue-NewDocument5 pagesHP Catalogue-NewNasree NiswongNo ratings yet
- Midtown Ratepayers Association's Letter To Ontario OmbudsmenDocument3 pagesMidtown Ratepayers Association's Letter To Ontario OmbudsmenAndrew GrahamNo ratings yet
- Pinoy Development of Groups and TeamsDocument19 pagesPinoy Development of Groups and TeamsSarah Jane SeñaNo ratings yet
- Podman Part4Document5 pagesPodman Part4anbuchennai82No ratings yet
- Ebiz Steps PDFDocument59 pagesEbiz Steps PDFBathina Srinivasa RaoNo ratings yet
- Midas - NFX - 2022R1 - Release NoteDocument10 pagesMidas - NFX - 2022R1 - Release NoteCristian Camilo Londoño PiedrahítaNo ratings yet
























































































Download as pdf or txt
You might also like
- Ann Rev Balic Et Al FinalDocument14 pagesAnn Rev Balic Et Al FinalFreddy A. ManayayNo ratings yet
- Liquid Biopsy From Discovery To Clinical ImplementationDocument5 pagesLiquid Biopsy From Discovery To Clinical ImplementationLais BritoNo ratings yet
- Mehta Et Al-2018-American Journal of TransplantationDocument8 pagesMehta Et Al-2018-American Journal of Transplantationpaul00040No ratings yet
- 33Document11 pages33Joana KellenNo ratings yet
- 10 Rosenberg Vitamin CDocument78 pages10 Rosenberg Vitamin CЩербакова ЛенаNo ratings yet
- Referensi 1Document9 pagesReferensi 1Indah Syaidatul MNo ratings yet
- 10 0000@ncbi NLM Nih gov@PMC6325475Document10 pages10 0000@ncbi NLM Nih gov@PMC6325475Tengku AdriansyahNo ratings yet
- Development of Prognostic Signatures For Intermediate Risk Papillary Thyroid CancerDocument12 pagesDevelopment of Prognostic Signatures For Intermediate Risk Papillary Thyroid Cancernfp.panjaitanNo ratings yet
- Brock Et Al Liquid Biopsy 2015Document11 pagesBrock Et Al Liquid Biopsy 2015Jean BiverNo ratings yet
- Fact de Pet n2Document6 pagesFact de Pet n2Pedro ChantaNo ratings yet
- Tiroides ArticuloDocument9 pagesTiroides Articulojuan sebaastianNo ratings yet
- DetectionDocument9 pagesDetectionHarshvardhan RavalNo ratings yet
- Vera2020 Article MultidisciplinaryManagementOfLDocument16 pagesVera2020 Article MultidisciplinaryManagementOfLDiego Andres VasquezNo ratings yet
- Nanotechnology and CancerDocument16 pagesNanotechnology and CancerMarcos LoredoNo ratings yet
- 8424365Document8 pages8424365Melody CyyNo ratings yet
- Epidemiology and Factors Related To The Survival of Metastatic Kidney Cancers: Retrospective Study at The Mohamed VI Center For The Cancer Treatment in Casablanca, MoroccoDocument5 pagesEpidemiology and Factors Related To The Survival of Metastatic Kidney Cancers: Retrospective Study at The Mohamed VI Center For The Cancer Treatment in Casablanca, MoroccoInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Imun PDFDocument4 pagesImun PDFLeyni SabatiniNo ratings yet
- 10 1002@cam4 2286Document11 pages10 1002@cam4 2286Ricardo MarquesNo ratings yet
- Assessment of Tumor Infiltrating Lymphocytes Using.12Document9 pagesAssessment of Tumor Infiltrating Lymphocytes Using.12Muhammad Rifki100% (1)
- The Role of Automated Cytometry in The New Era of Cancer Immunotherapy (Review)Document7 pagesThe Role of Automated Cytometry in The New Era of Cancer Immunotherapy (Review)Andrea SbranaNo ratings yet
- Risk Factors For Brain Metastasis-Colocerctal CancerDocument8 pagesRisk Factors For Brain Metastasis-Colocerctal CancerIstianah SakdullahNo ratings yet
- 408 2020 Article 407Document11 pages408 2020 Article 407CuchuluuNo ratings yet
- CA MammaeDocument6 pagesCA MammaeRiaNo ratings yet
- Int J Lab Hematology - 2017 - Galtseva - Minimal Residual Disease in Multiple Myeloma Benefits of Flow CytometryDocument9 pagesInt J Lab Hematology - 2017 - Galtseva - Minimal Residual Disease in Multiple Myeloma Benefits of Flow CytometrymatanhibNo ratings yet
- Jurnal Radiologi 2Document21 pagesJurnal Radiologi 2Adelya Dwi AsyifaNo ratings yet
- Research ArticleDocument7 pagesResearch ArticleZakia DrajatNo ratings yet
- Prognostic Indicators in Differentiated Thyroid Carcinoma: Diana S. Dean, MD, and Ian D. Hay, MB, PHD, FRCPDocument11 pagesPrognostic Indicators in Differentiated Thyroid Carcinoma: Diana S. Dean, MD, and Ian D. Hay, MB, PHD, FRCPEndang Rahayu Fuji LestaryNo ratings yet
- Ijbsv 16 P 1551Document12 pagesIjbsv 16 P 1551Flip Flop ChartNo ratings yet
- 0 Ba 2Document14 pages0 Ba 2faraz.mirza1No ratings yet
- Single Tube Liquid Biopsy For Advanced Non-Small Cell Lung CancerDocument11 pagesSingle Tube Liquid Biopsy For Advanced Non-Small Cell Lung CancerBikash Ranjan SamalNo ratings yet
- 1 s2.0 S1936523320303995 MainDocument10 pages1 s2.0 S1936523320303995 MainNoman M HasanNo ratings yet
- Circulating Tumor DNA and Radiological Tumor VolumDocument7 pagesCirculating Tumor DNA and Radiological Tumor Volumnaomireyes01No ratings yet
- MicroRNA-based Risk Scoring System To Identify EarDocument14 pagesMicroRNA-based Risk Scoring System To Identify EarDavidNo ratings yet
- TNBC PMRTDocument7 pagesTNBC PMRTMed MedNo ratings yet
- Neoadjuvant Treatment For Newly Diagnosed Advanced Ovarian Cancer. 2020Document9 pagesNeoadjuvant Treatment For Newly Diagnosed Advanced Ovarian Cancer. 2020Prodromos KoutoukoglouNo ratings yet
- Warde 2002Document5 pagesWarde 2002Bruno AlanNo ratings yet
- 10.thyroid Cancer TumorigenesisDocument18 pages10.thyroid Cancer TumorigenesisAccounting CV BakerNo ratings yet
- Atm 07 14 323Document9 pagesAtm 07 14 323Ethel GeanNo ratings yet
- The Use and Efficacy of Chemotherapy and Radiotherapy in Children and Adults With Pilocytic AstrocytomaDocument9 pagesThe Use and Efficacy of Chemotherapy and Radiotherapy in Children and Adults With Pilocytic AstrocytomaAlejandro Zurita SaáNo ratings yet
- Oyad006 PDFDocument2 pagesOyad006 PDFRaul Matute MartinNo ratings yet
- Pantel EA - 2012 - Circulating Cancer Cells and DNA - V2Document20 pagesPantel EA - 2012 - Circulating Cancer Cells and DNA - V2Clark Xingzhi ZhangNo ratings yet
- DTH 34 E14981Document9 pagesDTH 34 E14981Henry WijayaNo ratings yet
- Metastatic Hepatocellular Carcinoma Diagnosed by Fine Needle Aspiration: A Clinical and Cytologic StudyDocument6 pagesMetastatic Hepatocellular Carcinoma Diagnosed by Fine Needle Aspiration: A Clinical and Cytologic StudyMara PitrezNo ratings yet
- 11 Preoperative - High - Neutrophil-Lymphocyte - Ratio - MayDocument8 pages11 Preoperative - High - Neutrophil-Lymphocyte - Ratio - MayBridia BogarNo ratings yet
- Plasma MesothelinDocument7 pagesPlasma Mesothelinpaulo saNo ratings yet
- 1 s2.0 S0748798324003974 MainDocument1 page1 s2.0 S0748798324003974 MainShahnaz AhmedNo ratings yet
- International Journal of Scientific Research: OncologyDocument4 pagesInternational Journal of Scientific Research: OncologyRaul Matute MartinNo ratings yet
- 2013 Predicting Lymph Node Metastases in Early Rectal CancerDocument5 pages2013 Predicting Lymph Node Metastases in Early Rectal CancerjohnnhekoNo ratings yet
- Mir-155-5P Modulates Malignant Behaviors Of Hepatocellular Carcinoma By Directly Targeting Cthrc1 And Indirectly Regulating Gsk-3Β-Involved Wnt/Β-Catenin SignalingDocument12 pagesMir-155-5P Modulates Malignant Behaviors Of Hepatocellular Carcinoma By Directly Targeting Cthrc1 And Indirectly Regulating Gsk-3Β-Involved Wnt/Β-Catenin SignalingDeedee RenovaldiNo ratings yet
- Atm 08 20 1292Document11 pagesAtm 08 20 1292Ethel GeanNo ratings yet
- Church 2015Document1 pageChurch 2015TrabelsiNo ratings yet
- The Significance of Neutrophil/lymphocyte Ratio As A Possible Marker of Underlying Papillary Microcarcinomas in Thyroidal Goiters: A Pilot StudyDocument6 pagesThe Significance of Neutrophil/lymphocyte Ratio As A Possible Marker of Underlying Papillary Microcarcinomas in Thyroidal Goiters: A Pilot StudyagusNo ratings yet
- Liquid BiopsyDocument2 pagesLiquid BiopsySalman MajidNo ratings yet
- Radiotherapy and OncologyDocument6 pagesRadiotherapy and OncologyIntan Kartika NursyahbaniNo ratings yet
- Extracellular Nucleic Acids and Cancer: Michael - Fleischhacker@uk-Halle - de Bernd - Schmidt@uk-Halle - deDocument55 pagesExtracellular Nucleic Acids and Cancer: Michael - Fleischhacker@uk-Halle - de Bernd - Schmidt@uk-Halle - deAirin LeonieNo ratings yet
- Characterization of Adrenal Metastatic Cancer Using FDG PET CTDocument8 pagesCharacterization of Adrenal Metastatic Cancer Using FDG PET CTEngky ChristianNo ratings yet
- AlbaBernal ChallengesAndDocument10 pagesAlbaBernal ChallengesAndKhairul ScNo ratings yet
- The Journal of Pathology CR - 2024 - Knight - The Glasgow Microenvironment Score An Exemplar of Contemporary BiomarkerDocument16 pagesThe Journal of Pathology CR - 2024 - Knight - The Glasgow Microenvironment Score An Exemplar of Contemporary Biomarkerenrichedenlightenment05No ratings yet
- 10 1016@j Ejso 2020 03 188Document1 page10 1016@j Ejso 2020 03 188Andrіі DudashNo ratings yet
- 20.01.2024 Seating PlanDocument6 pages20.01.2024 Seating PlanPericherla Rakesh varmaNo ratings yet
- RMO 2016 Detailed AnalysisDocument6 pagesRMO 2016 Detailed AnalysisSaksham HoodaNo ratings yet
- Assessing The Feasibility of A New Venture 1.1 Assessment and Evaluation of Entrepreneurial OpportunitiesDocument13 pagesAssessing The Feasibility of A New Venture 1.1 Assessment and Evaluation of Entrepreneurial OpportunitiesBereket Desalegn100% (1)
- Cincinnati Retirement System Update: March 28, 2022Document24 pagesCincinnati Retirement System Update: March 28, 2022WVXU NewsNo ratings yet
- From Rice To Apple-Pear Style - An Ecocritical Approach To China's Korean Ethnic MinorityDocument14 pagesFrom Rice To Apple-Pear Style - An Ecocritical Approach To China's Korean Ethnic MinorityLing LIUNo ratings yet
- Product Risk Management Report For Spine ProductsDocument25 pagesProduct Risk Management Report For Spine ProductsAlejandro Landinez100% (1)
- Bio Drosophilia Mini Project 2 1Document15 pagesBio Drosophilia Mini Project 2 1jocyeo0% (1)
- Tc3yf en Manual 170905 He PDFDocument1 pageTc3yf en Manual 170905 He PDFJuan Manuel EscorihuelaNo ratings yet
- A Burdizzo Is Used For: A. Branding B. Dehorning C. Castration D. All of The AboveDocument54 pagesA Burdizzo Is Used For: A. Branding B. Dehorning C. Castration D. All of The AboveMac Dwayne CarpesoNo ratings yet
- PMP Exam EVOVLE Free SampleDocument47 pagesPMP Exam EVOVLE Free SampleEvolve trainingmaterialsNo ratings yet
- Revised 04/01/2021Document33 pagesRevised 04/01/2021Kim PowellNo ratings yet
- VarahamihiraDocument6 pagesVarahamihiraSTAR GROUPS100% (1)
- Suraj Estate Developers Limited RHPDocument532 pagesSuraj Estate Developers Limited RHPJerry SinghNo ratings yet
- Nunez v. Sec - y of HHS - 2019 U.S. Claims LEXIS 644Document40 pagesNunez v. Sec - y of HHS - 2019 U.S. Claims LEXIS 644Kirk HartleyNo ratings yet
- ASR 2020 J2Prelim H2Chem P4 QP PDFDocument20 pagesASR 2020 J2Prelim H2Chem P4 QP PDFchuasioklengNo ratings yet
- Biostat IntroductionDocument31 pagesBiostat IntroductionteklayNo ratings yet
- اختبار الوزن النوعي و امتصاص الماء لركامDocument78 pagesاختبار الوزن النوعي و امتصاص الماء لركامحسين المهندسNo ratings yet
- Alim Knit (BD) LTD.: Recommended Process Flow DiagramDocument1 pageAlim Knit (BD) LTD.: Recommended Process Flow DiagramKamrul HasanNo ratings yet
- التحليل المكاني والوظيفي للخدمات التعليمية في مدينة سوران باستخدام نظم المعلومات الجغرافية- عمر حسن حسين رواندزي- ماجستيرDocument178 pagesالتحليل المكاني والوظيفي للخدمات التعليمية في مدينة سوران باستخدام نظم المعلومات الجغرافية- عمر حسن حسين رواندزي- ماجستيرMahmoud Abdelrahman86% (7)
- Material ManagementDocument20 pagesMaterial Managementgkataria110100% (1)
- SSC Gr10 ICT Q4 Module 2 WK 2 - v.01-CC-released-7June2021Document16 pagesSSC Gr10 ICT Q4 Module 2 WK 2 - v.01-CC-released-7June2021Vj AleserNo ratings yet
- Recounttext 160409104911Document9 pagesRecounttext 160409104911Anif Ough GtuwNo ratings yet
- Botech. IDocument37 pagesBotech. IKevin Rose BarnuevoNo ratings yet
- Achieving Success Through Effective Business CommunicationDocument36 pagesAchieving Success Through Effective Business Communicationfaizankhan23No ratings yet
- HP Catalogue-NewDocument5 pagesHP Catalogue-NewNasree NiswongNo ratings yet
- Midtown Ratepayers Association's Letter To Ontario OmbudsmenDocument3 pagesMidtown Ratepayers Association's Letter To Ontario OmbudsmenAndrew GrahamNo ratings yet
- Pinoy Development of Groups and TeamsDocument19 pagesPinoy Development of Groups and TeamsSarah Jane SeñaNo ratings yet
- Podman Part4Document5 pagesPodman Part4anbuchennai82No ratings yet
- Ebiz Steps PDFDocument59 pagesEbiz Steps PDFBathina Srinivasa RaoNo ratings yet
- Midas - NFX - 2022R1 - Release NoteDocument10 pagesMidas - NFX - 2022R1 - Release NoteCristian Camilo Londoño PiedrahítaNo ratings yet