Download as pdf or txt
You might also like
- US Army Mechanic Metal Auto Body RepairDocument108 pagesUS Army Mechanic Metal Auto Body RepairSpace_Hulker100% (2)
- O Level Computer Studies Notes - ZIMSEC Syllabus PDFDocument98 pagesO Level Computer Studies Notes - ZIMSEC Syllabus PDFkeith magaka71% (89)
- Pecarn ProofDocument5 pagesPecarn Prooftfysksw6q8No ratings yet
- European Journal of Radiology: M Kiani, A ChaparianDocument7 pagesEuropean Journal of Radiology: M Kiani, A ChaparianHamza ArjahNo ratings yet
- Referensi Nomor 13Document5 pagesReferensi Nomor 13khusnulNo ratings yet
- 03 Evaluating and CommunicatingDocument47 pages03 Evaluating and CommunicatingAsif JIELANINo ratings yet
- Multidetector CT in ChildrenDocument21 pagesMultidetector CT in Childrenpaquidermo85No ratings yet
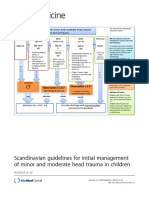
- Scandinavian Guidelines For Initial Management of Minor and Moderate Head Trauma in ChildrenDocument20 pagesScandinavian Guidelines For Initial Management of Minor and Moderate Head Trauma in ChildrenRafael Mujica OreNo ratings yet
- 2361 15492 1 PBDocument6 pages2361 15492 1 PBAndri ArdhanyNo ratings yet
- PECARN Algorithms For Minor Head TraumaDocument11 pagesPECARN Algorithms For Minor Head Traumaedgarjavier65No ratings yet
- Retinoblast Tumor Visìvel 2017Document16 pagesRetinoblast Tumor Visìvel 2017Vinicio CoelhoNo ratings yet
- Paediatric Neck MassesDocument7 pagesPaediatric Neck MassesGiovanni HenryNo ratings yet
- Research: CATCH: A Clinical Decision Rule For The Use of Computed Tomography in Children With Minor Head InjuryDocument8 pagesResearch: CATCH: A Clinical Decision Rule For The Use of Computed Tomography in Children With Minor Head InjuryCarlos Martin Yafac RiscoNo ratings yet
- TSNC - F Cognitivas SubrayadoDocument8 pagesTSNC - F Cognitivas SubrayadoEus CádizNo ratings yet
- Pre-hospital Dutch StudyDocument5 pagesPre-hospital Dutch Studyjose alberto linares valverdeNo ratings yet
- First Page PDFDocument1 pageFirst Page PDFTian Nopita SariNo ratings yet
- RT PediatricDocument9 pagesRT Pediatricfaza mawaddahNo ratings yet
- Quickbrain Mri For The Detection of Acute Pediatric Traumatic Brain InjuryDocument6 pagesQuickbrain Mri For The Detection of Acute Pediatric Traumatic Brain InjuryGenesis VelasteguiNo ratings yet
- Tce 2020 LibanoDocument11 pagesTce 2020 LibanoLaura ScottNo ratings yet
- MRI Findings in Prematurely Born Adolescents and YDocument3 pagesMRI Findings in Prematurely Born Adolescents and YGiska VelindaNo ratings yet
- Pone 0211599Document12 pagesPone 0211599HILA GINANo ratings yet
- 235Document11 pages2350128 Nurul Wahidah YasidNo ratings yet
- Diagnostics 13 03669Document15 pagesDiagnostics 13 03669Micran ThesisNo ratings yet
- Perilongo 1997Document7 pagesPerilongo 1997Gustav RSRNo ratings yet
- JURNAL RetinoblastomaDocument32 pagesJURNAL Retinoblastomadokteradhit891438No ratings yet
- 1 s2.0 S0720048X11003214 MainDocument5 pages1 s2.0 S0720048X11003214 MainHamza ArjahNo ratings yet
- Craniospinal Irradiation Treatment Techniques For Pediatric Medulloblastoma PatientsDocument15 pagesCraniospinal Irradiation Treatment Techniques For Pediatric Medulloblastoma PatientsRus Paul OvidiuNo ratings yet
- Pittsburg Pediatric StudyDocument7 pagesPittsburg Pediatric Studyjose alberto linares valverdeNo ratings yet
- Profile of Congenital Rubella Syndrome in Soetomo General Hospital Surabaya, IndonesiaDocument3 pagesProfile of Congenital Rubella Syndrome in Soetomo General Hospital Surabaya, IndonesiawilmaNo ratings yet
- DOI Problem 2Document11 pagesDOI Problem 2RajendraNo ratings yet
- Use of High-Dose Chemotherapy in Front-Line TherapDocument8 pagesUse of High-Dose Chemotherapy in Front-Line TherapSri Eka HandayaniNo ratings yet
- Early Identification of Cerebral Palsy Using Neonatal MRI and General Movements Assessment in A Cohort of High-Risk Term NeonatesDocument6 pagesEarly Identification of Cerebral Palsy Using Neonatal MRI and General Movements Assessment in A Cohort of High-Risk Term Neonatesarif 2006No ratings yet
- Prognostic Factors For Relapse and Outcome in Pediatric Acute Transverse MyelitisDocument11 pagesPrognostic Factors For Relapse and Outcome in Pediatric Acute Transverse Myelitisyusak sampeNo ratings yet
- Predictive Value of Cranial Ultrasound For Neurodevelopmental Outcomes of Very Preterm Infants With Brain InjuryDocument8 pagesPredictive Value of Cranial Ultrasound For Neurodevelopmental Outcomes of Very Preterm Infants With Brain Injuryleivaherre10No ratings yet
- Prospective Evaluation of A Pediatric Inpatient Early Warning Scoring SystemDocument7 pagesProspective Evaluation of A Pediatric Inpatient Early Warning Scoring SystemKarma SetiyawanNo ratings yet
- Children and Neonates Anesthesia in Magnetic Resonance Environment in Italy - BMC Anest22Document9 pagesChildren and Neonates Anesthesia in Magnetic Resonance Environment in Italy - BMC Anest22Gunther MirandaNo ratings yet
- Estimating Intracranial Volume Using Intracranial Area inDocument7 pagesEstimating Intracranial Volume Using Intracranial Area inEdbert WielimNo ratings yet
- Diagnosing Delirium in Critically Ill Children - Validity and Reliability of The Pediatric Confusion Assessment Method For The Intensive Care UnitDocument20 pagesDiagnosing Delirium in Critically Ill Children - Validity and Reliability of The Pediatric Confusion Assessment Method For The Intensive Care UnitCarla MesquitaNo ratings yet
- Fneur 12 722696Document7 pagesFneur 12 722696Laraswati RianiNo ratings yet
- Radiol 2019181753Document10 pagesRadiol 2019181753Esteban PalaciosNo ratings yet
- Techniques in Pediatric MRI - Tips For Imaging Children: How-I-do-itDocument11 pagesTechniques in Pediatric MRI - Tips For Imaging Children: How-I-do-itBOUSSAID KARIMNo ratings yet
- American Journal of Emergency MedicineDocument7 pagesAmerican Journal of Emergency MedicineAngelina PondeteNo ratings yet
- Safe Pediatric AnesthesiaDocument24 pagesSafe Pediatric AnesthesiamdNo ratings yet
- Congenital Rubella Syndrome: An Overview of Clinical Presentations in Bangladeshi ChildrenDocument6 pagesCongenital Rubella Syndrome: An Overview of Clinical Presentations in Bangladeshi ChildrenSajjad Hossain ShuvoNo ratings yet
- Pulse Oximetry Screening To Detect Critical Congenital Heart Diseases in Asymptomatic NeonatesDocument6 pagesPulse Oximetry Screening To Detect Critical Congenital Heart Diseases in Asymptomatic Neonatesdebbie_rose89No ratings yet
- Diagnostic ImagingDocument16 pagesDiagnostic ImagingJeffTaborNo ratings yet
- 247 2011 Article 2201 PDFDocument13 pages247 2011 Article 2201 PDFArdianNo ratings yet
- PERCANDocument11 pagesPERCANOscar David Gamarra PerezNo ratings yet
- AJODO-2013 AlNajjar 143 6 784 PDFDocument9 pagesAJODO-2013 AlNajjar 143 6 784 PDFplayer osamaNo ratings yet
- Symposium Article: Imaging of A Child With PolytraumaDocument22 pagesSymposium Article: Imaging of A Child With PolytraumaAnonymous wdmpgxNo ratings yet
- Neonatal Brain Tumors A Review 2017Document5 pagesNeonatal Brain Tumors A Review 2017FarhanNo ratings yet
- Neuroimagenes en Preterminos y Rendimiento EscolarDocument15 pagesNeuroimagenes en Preterminos y Rendimiento EscolarAlejandroVeraVargasNo ratings yet
- Siu - Et - Al - Imaging in CI - 2019-The - LaryngoscopeDocument8 pagesSiu - Et - Al - Imaging in CI - 2019-The - LaryngoscopePhong HoàngNo ratings yet
- Amiel Tison2012Document7 pagesAmiel Tison2012Anonymous Xmb6QQvRNo ratings yet
- Journal 1Document6 pagesJournal 1dr. Nadia SalsabilaNo ratings yet
- Am J Otolaryngol: Jillian N. Printz, Katelin A. Mirkin, Christopher S. Hollenbeak, Michele M. Carr TDocument6 pagesAm J Otolaryngol: Jillian N. Printz, Katelin A. Mirkin, Christopher S. Hollenbeak, Michele M. Carr TruthchristinawibowoNo ratings yet
- Consensus Approach For Standardizing The Screening and Classification of Preterm Brain Injury Diagnosed With Cranial Ultrasound A Canadian PerspectiveDocument19 pagesConsensus Approach For Standardizing The Screening and Classification of Preterm Brain Injury Diagnosed With Cranial Ultrasound A Canadian PerspectiveJemima ChanNo ratings yet
- E37 FullDocument10 pagesE37 FullAtika RahmahNo ratings yet
- DOI:10.31557/APJCC.2018.3.2.37: Golda Asina Miranda, Et Al: Retinoblastoma in A Tertiary Hospital in A Remote AreaDocument9 pagesDOI:10.31557/APJCC.2018.3.2.37: Golda Asina Miranda, Et Al: Retinoblastoma in A Tertiary Hospital in A Remote Areasyerin fitria sariNo ratings yet
- GSCBPS 2020 0295Document7 pagesGSCBPS 2020 0295Istianah SakdullahNo ratings yet
- Target Volume Delineation for Pediatric CancersFrom EverandTarget Volume Delineation for Pediatric CancersStephanie A. TerezakisNo ratings yet
- Echography and Doppler of the BrainFrom EverandEchography and Doppler of the BrainChiara RobbaNo ratings yet
- PivotapiDocument35 pagesPivotapiscribd.resident588No ratings yet
- Boiler Operator Exam Preparation Guide pdf-1 PDFDocument27 pagesBoiler Operator Exam Preparation Guide pdf-1 PDFEmmanuel Jesus Marquez Rea100% (1)
- Intersection Matlab FunctionDocument5 pagesIntersection Matlab FunctionNadeem Ul HaqNo ratings yet
- Catalytic Wet Air OxidationDocument10 pagesCatalytic Wet Air OxidationAman PrasadNo ratings yet
- Asat Paper (Iq) Series (Easy) (11 To 12) : A. B. C. DDocument7 pagesAsat Paper (Iq) Series (Easy) (11 To 12) : A. B. C. DAbhijeet Singh PanwarNo ratings yet
- IECEx Za Namur Davač ImpulsaDocument12 pagesIECEx Za Namur Davač Impulsajosip miskovicNo ratings yet
- DT 13 05 2018Document29 pagesDT 13 05 2018TIRTH JOSHINo ratings yet
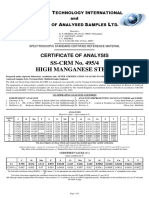
- Ss CRM 495 - 4Document2 pagesSs CRM 495 - 4lehdruk7100No ratings yet
- Design, Implementation and Verification of 32-Bit ALU With VIODocument6 pagesDesign, Implementation and Verification of 32-Bit ALU With VIONubia DiazNo ratings yet
- B 121 101 (Cb-11a-33 (3a) (3C) (3Q) )Document1 pageB 121 101 (Cb-11a-33 (3a) (3C) (3Q) )sasidharreddyNo ratings yet
- Surround Processor NJW1186Document17 pagesSurround Processor NJW1186MadhanNo ratings yet
- 1mesh TrackDocument92 pages1mesh TrackAbdon CastroNo ratings yet
- System Resources On PC (IRQ, DMA, I-OAddress)Document4 pagesSystem Resources On PC (IRQ, DMA, I-OAddress)guilhangNo ratings yet
- Masonry TutorialDocument45 pagesMasonry TutorialGajendra Joshi100% (2)
- EuroGeo6 Carmine Gerardo GragnanoDocument12 pagesEuroGeo6 Carmine Gerardo GragnanoJON DAVIDNo ratings yet
- 02 Final Basic Hydraulic (Module-II)Document8 pages02 Final Basic Hydraulic (Module-II)Pyae Phyoe AungNo ratings yet
- The Data.: Question 1: Create A Table Insert Records and ManipulateDocument32 pagesThe Data.: Question 1: Create A Table Insert Records and ManipulateSSC CHSL100% (1)
- The History and Evolution of QuaternionsDocument3 pagesThe History and Evolution of QuaternionsAnton Van WykNo ratings yet
- Voltaic Cell - Yale UniversityDocument4 pagesVoltaic Cell - Yale UniversityBelenNo ratings yet
- Phased Array Radars: J. L. Chau, C. J. Heinselman, M. J. NicollsDocument52 pagesPhased Array Radars: J. L. Chau, C. J. Heinselman, M. J. NicollsNguyễn Hoàng Giang100% (1)
- Ca1 PDocument2 pagesCa1 PYash jangidNo ratings yet
- Malanjkhend Report Raj Veer Singh CHATEN BHOPALDocument53 pagesMalanjkhend Report Raj Veer Singh CHATEN BHOPALvidhya associateNo ratings yet
- Film Formation in Coatings - Properties, Mechanisms, and ApplicationsDocument10 pagesFilm Formation in Coatings - Properties, Mechanisms, and ApplicationsAadhi InnovativesNo ratings yet
- Basic Principles in Formworks Design-ACELDocument44 pagesBasic Principles in Formworks Design-ACELronelyn bernalNo ratings yet
- Best Microscope PPT Prepared ...Document134 pagesBest Microscope PPT Prepared ...Daniel Lemma100% (1)
- IoT Applications in The Maintenance IndustryDocument15 pagesIoT Applications in The Maintenance IndustrypriyalNo ratings yet
- Nouradini PDFDocument15 pagesNouradini PDFDavi AhmadNo ratings yet
- Bai Giang - CT361 - Chuong 4 (PDF - Io)Document18 pagesBai Giang - CT361 - Chuong 4 (PDF - Io)Nghiệp Nguyễn ThànhNo ratings yet