Download as docx, pdf, or txt
You might also like
- MOA TupadDocument5 pagesMOA TupadEmil BarengNo ratings yet
- Safety Seal Certification Checklist: City Government of CalambaDocument3 pagesSafety Seal Certification Checklist: City Government of CalambaGloria CanapiNo ratings yet
- Safety Seal Certification Checklist: # Requirements Y E S N O N/ ADocument4 pagesSafety Seal Certification Checklist: # Requirements Y E S N O N/ AJay Dela Rama JovenNo ratings yet
- Safet Seal Certification ChecklistDocument2 pagesSafet Seal Certification ChecklistKimberlie DagamiNo ratings yet
- Safety Seal Certification Checklist: (DILG As Issuing Authority)Document3 pagesSafety Seal Certification Checklist: (DILG As Issuing Authority)Mike Noel Baraquiel100% (2)
- Safety Seal Certification ChecklistDocument2 pagesSafety Seal Certification ChecklistKathlynn Joy de GuiaNo ratings yet
- Safet Seal Certification Checklist DILGDocument2 pagesSafet Seal Certification Checklist DILGBLGU Lake DanaoNo ratings yet
- Safety Seal Certification Checklist: Municipality of ArakanDocument2 pagesSafety Seal Certification Checklist: Municipality of ArakanBPLS ArakanNo ratings yet
- Safety Seal Certification Checklist Draft CRA AJLv 052021Document4 pagesSafety Seal Certification Checklist Draft CRA AJLv 052021Barangay Segunda PuloNo ratings yet
- SAFETY SEAL Form2Document3 pagesSAFETY SEAL Form2Al Raymond Dullano TupasNo ratings yet
- Safety Seal Certification Checklist: (DILG As Issuing Authority)Document3 pagesSafety Seal Certification Checklist: (DILG As Issuing Authority)Jeanibabe Perez PanagNo ratings yet
- Safety Seal Certification ChecklistDocument3 pagesSafety Seal Certification ChecklistBARANGAY MOLINO IINo ratings yet
- Safety Seal Certification Checklist: Contact DetailsDocument3 pagesSafety Seal Certification Checklist: Contact DetailsMelania SeangoyNo ratings yet
- Safety Seal Certification ChecklistDocument2 pagesSafety Seal Certification ChecklistMeljovin F. Dela CruzNo ratings yet
- Safety Seal Checklist 2022Document3 pagesSafety Seal Checklist 2022Jocelyn SunigaNo ratings yet
- Safety Seal Certification Checklist: Department of The Interior and Local GovernmentDocument2 pagesSafety Seal Certification Checklist: Department of The Interior and Local GovernmentBarangay CentroNo ratings yet
- Safety Seal Certification ChecklistDocument2 pagesSafety Seal Certification ChecklistHav Cats100% (2)
- Assessment Tool For Health and Safety Standards For The Prevention of Covid-19 in Government Offices and Other Workplaces I. Workplace InformationDocument4 pagesAssessment Tool For Health and Safety Standards For The Prevention of Covid-19 in Government Offices and Other Workplaces I. Workplace InformationEric T. CabayacruzNo ratings yet
- New Checklist Last Edited As of Today October 42022Document2 pagesNew Checklist Last Edited As of Today October 42022Omar Dizon IINo ratings yet
- Module 4 - Safety Seal ChecklistDocument3 pagesModule 4 - Safety Seal ChecklistMyra Flor MagnayeNo ratings yet
- Safety Seal Certification Checklist: (DILG As Issuing Authority)Document3 pagesSafety Seal Certification Checklist: (DILG As Issuing Authority)Mena Yves Delavin BurdeosNo ratings yet
- Safety Seal Certification Checklist: (LGU As Issuing Authority)Document2 pagesSafety Seal Certification Checklist: (LGU As Issuing Authority)Gyne PalacaNo ratings yet
- Legionella Environmental Assessment CDCDocument24 pagesLegionella Environmental Assessment CDCBam ManNo ratings yet
- Checklist - R6-2021-0003345Document3 pagesChecklist - R6-2021-0003345Kenya NacorNo ratings yet
- Safety Seal Certification Checklist: ( - As Issuing Officer)Document2 pagesSafety Seal Certification Checklist: ( - As Issuing Officer)Yoregeff DaiunNo ratings yet
- SafetysealchecklistDocument1 pageSafetysealchecklistKatherine VerceluzNo ratings yet
- CDC / SNP / Pelc / Tahderiyyah Center Health and Safety ChecklistDocument1 pageCDC / SNP / Pelc / Tahderiyyah Center Health and Safety ChecklistAr FaNo ratings yet
- Safety Seal Presentation For DepEdDocument11 pagesSafety Seal Presentation For DepEdjoy sotoNo ratings yet
- Safety Seal For BarangayDocument18 pagesSafety Seal For BarangayBarangay Segunda PuloNo ratings yet
- Safety Seal ProcessDocument18 pagesSafety Seal Processkeith tanuecoNo ratings yet
- Department of Environment and Natural Resources: 3 Floor Northwing Building, DENR-XI Compound, Lanang, Davao CityDocument2 pagesDepartment of Environment and Natural Resources: 3 Floor Northwing Building, DENR-XI Compound, Lanang, Davao CityKaren Feyt MallariNo ratings yet
- Checklist Iv TerminationDocument2 pagesChecklist Iv TerminationMichaelNo ratings yet
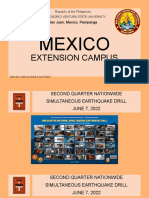
- DHVSU Mexico Campus UOSH and DRRMODocument37 pagesDHVSU Mexico Campus UOSH and DRRMOJeff GarciaNo ratings yet
- Lead Registration Form and LMP OutlineDocument5 pagesLead Registration Form and LMP OutlineonaljenNo ratings yet
- DHVSU Mexico CampusDocument37 pagesDHVSU Mexico CampusJeff GarciaNo ratings yet
- Ny Forward Safety Plan TemplateDocument6 pagesNy Forward Safety Plan Templatejim francoNo ratings yet
- Safety Seal Certification Checklist: (LGU As Issuing Authority)Document4 pagesSafety Seal Certification Checklist: (LGU As Issuing Authority)Mena Yves Delavin BurdeosNo ratings yet
- Self-Monitoring Compliance Form: Safety Requirements Compliant Yes NoDocument1 pageSelf-Monitoring Compliance Form: Safety Requirements Compliant Yes NoCRISOL JR CATENo ratings yet
- Self-Monitoring Compliance Form: Safety Requirements Compliant Yes NoDocument1 pageSelf-Monitoring Compliance Form: Safety Requirements Compliant Yes NoCRISOL JR CATENo ratings yet
- Covid - 19 Contact Tracers Performance Monitoring of Weekly AccomplishmentsDocument3 pagesCovid - 19 Contact Tracers Performance Monitoring of Weekly AccomplishmentsClaudine PuyaoNo ratings yet
- New York State Department of Health Ny Forward Business Reopening Safety PlanDocument4 pagesNew York State Department of Health Ny Forward Business Reopening Safety PlanPriti SaldanhaNo ratings yet
- Ascotf Checklist NewDocument4 pagesAscotf Checklist NewChristine Joy BautistaNo ratings yet
- Cco-Asbestos Registration FormDocument4 pagesCco-Asbestos Registration FormKaren Feyt MallariNo ratings yet
- Rise 2021 Informed Consent Form To The Pogs Data Privacy PolicyDocument2 pagesRise 2021 Informed Consent Form To The Pogs Data Privacy PolicyJonelle baloloyNo ratings yet
- AO New Normal FinalDocument5 pagesAO New Normal FinalTumasitoe Bautista LasquiteNo ratings yet
- COVIDSafe Event ChecklistDocument4 pagesCOVIDSafe Event ChecklistBerina KatanaNo ratings yet
- New York State Business Reopening Safety Plan TemplateDocument6 pagesNew York State Business Reopening Safety Plan TemplateThe Livingston County NewsNo ratings yet
- CHRDR Application FormDocument2 pagesCHRDR Application FormNifee NipsNo ratings yet
- CCENRODocument2 pagesCCENRObrenda louNo ratings yet
- General OSH Checklist FINALDocument3 pagesGeneral OSH Checklist FINALEMELYN HIWATIG100% (1)
- Poly Fiber Reducer R65-75Document2 pagesPoly Fiber Reducer R65-75Mark Evan SalutinNo ratings yet
- MC 2020041Document3 pagesMC 2020041Jerrick LimNo ratings yet
- Visitor HSE Induction FormDocument3 pagesVisitor HSE Induction Formch.kashifpervezNo ratings yet
- COVID-19 Preparedness and Response Plan Template - Updated 6.8.20 - 202006081252049904Document8 pagesCOVID-19 Preparedness and Response Plan Template - Updated 6.8.20 - 202006081252049904Sujit ShahNo ratings yet
- Just A SampleDocument10 pagesJust A SampleVone MoresNo ratings yet
- Georgia PracticesDocument11 pagesGeorgia PracticesTHR100% (1)
- Game Plan of Hospitality and Tourism Industry During Covid-19 Pandemic: Highlight of Best PracticesDocument11 pagesGame Plan of Hospitality and Tourism Industry During Covid-19 Pandemic: Highlight of Best PracticesQuintin Fronda Jr.No ratings yet
- Barrosa-Esteves-Mahomoc-Ojt-Final-Narrative 2Document2 pagesBarrosa-Esteves-Mahomoc-Ojt-Final-Narrative 2pumarigam7No ratings yet
- Mozart Andante in C MajorDocument7 pagesMozart Andante in C Majorparia dNo ratings yet
- MEMO Safety Induction Nov 2022Document2 pagesMEMO Safety Induction Nov 2022Siddiq RahimNo ratings yet
- Covid 19 WorksheetsDocument16 pagesCovid 19 WorksheetsKarla Paola MoralesNo ratings yet
- Maklumat Vaksinasi: Vaccination DetailsDocument2 pagesMaklumat Vaksinasi: Vaccination DetailsRedha HaqimiNo ratings yet
- Hindko. Likhtaan Magazine 1.Document64 pagesHindko. Likhtaan Magazine 1.Near N DearNo ratings yet
- Bhert Ex - OrderDocument3 pagesBhert Ex - OrderJoy Javier Abonita RazadoNo ratings yet
- H8ST9K: Clarence Alcordo (Booking No: H8ST9K) 23 Mar 2023 Manila Davao - Travel ItineraryDocument3 pagesH8ST9K: Clarence Alcordo (Booking No: H8ST9K) 23 Mar 2023 Manila Davao - Travel ItineraryNoreen AquinoNo ratings yet
- Contingency Plan On Limited f2fDocument36 pagesContingency Plan On Limited f2fJoannie AmparoNo ratings yet
- You Must Believe in Spring - Bill EvansDocument6 pagesYou Must Believe in Spring - Bill Evanssimix 02No ratings yet
- G 12 STEM HRPTA Minutes of The MeetingDocument3 pagesG 12 STEM HRPTA Minutes of The MeetingAlvin Ray GarciaNo ratings yet
- School Contingency PlanDocument3 pagesSchool Contingency PlanVictoria Beltran SubaranNo ratings yet
- MMWGH Milestone 2019-2023Document3 pagesMMWGH Milestone 2019-2023Aaron Christopher SungaNo ratings yet
- 김성백의 영어뉴스 핵심패턴 (126-130회) - 업로드용Document20 pages김성백의 영어뉴스 핵심패턴 (126-130회) - 업로드용aganamuyaNo ratings yet
- CertificateDocument1 pageCertificateriteshNo ratings yet
- 1.3.6.3 Bukti Pelaksanaan Imunisasi PegawaiDocument2 pages1.3.6.3 Bukti Pelaksanaan Imunisasi Pegawaienglautami013No ratings yet
- Presentation - Inter-Agency Task Force (Iatf) New Normal Guidelines For The New NormalDocument19 pagesPresentation - Inter-Agency Task Force (Iatf) New Normal Guidelines For The New NormalLyka Marie DesepedaNo ratings yet
- Vaccination CertificateDocument1 pageVaccination CertificateAjay MahtoNo ratings yet
- Webinar#3 (Victor Bangun Mulia)Document11 pagesWebinar#3 (Victor Bangun Mulia)setyaaristuNo ratings yet
- PSC Minutes Jan 2023Document2 pagesPSC Minutes Jan 2023KAUSPH NURSING SERVICENo ratings yet
- Certificate Manju 2Document1 pageCertificate Manju 2ಅ ಪರಿಚಿತNo ratings yet
- Mission Ballroom - Permitted Items and General RulesDocument1 pageMission Ballroom - Permitted Items and General RulesLogan NovakNo ratings yet
- Magicar 906 Remote FunctionsDocument19 pagesMagicar 906 Remote FunctionsravzatovboburNo ratings yet
- ArticleDocument1 pageArticleKaren Fae Manalo JimenezNo ratings yet
- Essay On Covid - 19Document2 pagesEssay On Covid - 19SK SintujaNo ratings yet
- Maklumat Vaksinasi: Vaccination DetailsDocument2 pagesMaklumat Vaksinasi: Vaccination DetailsHafizNo ratings yet
- Coronavirus (COVID-19) RecordsDocument2 pagesCoronavirus (COVID-19) Recordspepenig977No ratings yet
- Philosphy AssignmentDocument2 pagesPhilosphy Assignmentpang jing zheNo ratings yet
- Front PageDocument1 pageFront PagePan PanNo ratings yet
- Health Pass SertifikaDocument2 pagesHealth Pass SertifikaburcingulecNo ratings yet
- C 17 Paginearee 5367 0 FileDocument1 pageC 17 Paginearee 5367 0 FileDionisius Dino BrianantoNo ratings yet