Download as pdf or txt
You might also like
- Marie Seton - Sergei Eisenstein, The Definitive Einsenstein - 1960Document612 pagesMarie Seton - Sergei Eisenstein, The Definitive Einsenstein - 1960Fernando Svetko0% (1)
- Scenario Planning StarBucksDocument10 pagesScenario Planning StarBucksA.k. Aditya33% (3)
- Iap 2010Document6 pagesIap 2010Shalinee PrasadNo ratings yet
- Role of Bpni in Promotion of Breast Feeding in IndiaDocument32 pagesRole of Bpni in Promotion of Breast Feeding in IndiaAnju RaniNo ratings yet
- 50 Years of Neonatology in India Progress and FutureDocument3 pages50 Years of Neonatology in India Progress and FutureSutirtha RoyNo ratings yet
- Breastfeeding Promotion by Breastfeeding Promotion Group Kerala University of Health Sciences Kerala IndiaDocument7 pagesBreastfeeding Promotion by Breastfeeding Promotion Group Kerala University of Health Sciences Kerala Indiamrs raamNo ratings yet
- Breastfeeding Policy Analysis in IndonesiaDocument4 pagesBreastfeeding Policy Analysis in IndonesiaAndini PramonoNo ratings yet
- Operational Guidelines For Establishing Sentinel Stillbirth Surveillance SystemDocument40 pagesOperational Guidelines For Establishing Sentinel Stillbirth Surveillance Systemraval anil.uNo ratings yet
- Anmguidelines 100713234718 Phpapp01Document140 pagesAnmguidelines 100713234718 Phpapp01kirank_11100% (1)
- Reproductive, Maternal, Newborn, Child and Adolescent Health ProgrammeDocument14 pagesReproductive, Maternal, Newborn, Child and Adolescent Health ProgrammeDiksha singhNo ratings yet
- Jurnal International PDFDocument6 pagesJurnal International PDFFitriNo ratings yet
- 17Document12 pages17Johana RiveraNo ratings yet
- Save The Children Child Survival - Position Paper 2009Document7 pagesSave The Children Child Survival - Position Paper 2009nileshsingh29062092No ratings yet
- Xu 2018 - Childbirth and EENC Practices in 4 Provinces in ChinaDocument9 pagesXu 2018 - Childbirth and EENC Practices in 4 Provinces in ChinaZhao LiNo ratings yet
- Participant Manual Fbcsa MalnutritionDocument138 pagesParticipant Manual Fbcsa MalnutritionPriyaancaHaarsh100% (2)
- IBFANDocument11 pagesIBFANlrodríguez_309124No ratings yet
- Clinical Guidelines On IYCF - 1Document37 pagesClinical Guidelines On IYCF - 1ইসরাত বারীNo ratings yet
- Family Welfare Programme in IndiaDocument25 pagesFamily Welfare Programme in IndiaTirumalesha DadigeNo ratings yet
- Brief Note On Child HealthDocument6 pagesBrief Note On Child HealthSivakumar Reddy JeevanNo ratings yet
- Optimizing Breastfeeding For Better Health Outcomes The Way ForwardDocument4 pagesOptimizing Breastfeeding For Better Health Outcomes The Way ForwardEditor IJTSRDNo ratings yet
- Iyt FeedingDocument16 pagesIyt FeedingAfnita LestaryNo ratings yet
- Improving Breastfeeding Support Through The Implementation of The Baby-Friendly Hospital and Community Initiatives: A Scoping ReviewDocument18 pagesImproving Breastfeeding Support Through The Implementation of The Baby-Friendly Hospital and Community Initiatives: A Scoping ReviewonemNo ratings yet
- Protocol - 7 - English TranslationDocument16 pagesProtocol - 7 - English Translationsebastianidenise2No ratings yet
- Infant and Young Child FeedingDocument31 pagesInfant and Young Child FeedingKhair Soomro100% (2)
- Consensus Statement of The Indian Academy of Pediatrics On Integrated Management of Severe Acute MalnutritionDocument6 pagesConsensus Statement of The Indian Academy of Pediatrics On Integrated Management of Severe Acute MalnutritiondrtgodeNo ratings yet
- Midwifery ENGDocument92 pagesMidwifery ENGindaNo ratings yet
- Maternal Child Nutrition - 2016 - P Rez Escamilla - Impact of The Baby Friendly Hospital Initiative On Breastfeeding andDocument16 pagesMaternal Child Nutrition - 2016 - P Rez Escamilla - Impact of The Baby Friendly Hospital Initiative On Breastfeeding andNur FauziyahNo ratings yet
- Adaptation and Psychometric Evaluation of The Breastfeeding Self-Efficacy Scale To Assess Exclusive BreastfeedingDocument14 pagesAdaptation and Psychometric Evaluation of The Breastfeeding Self-Efficacy Scale To Assess Exclusive Breastfeedingcardenala haganinthaNo ratings yet
- 19 PDFDocument2 pages19 PDFSakshi SharmaNo ratings yet
- Report On Model Anganwadi KendrasDocument5 pagesReport On Model Anganwadi KendrasNakul ArunNo ratings yet
- Operational Guidelines For FimnciDocument29 pagesOperational Guidelines For FimnciAkashdeep RathodNo ratings yet
- 3 BBL Q1 JurnalDocument8 pages3 BBL Q1 JurnalarumNo ratings yet
- A SWOT Analysis of Government Schemes For Pregnant and Lactating Women in IndiaDocument7 pagesA SWOT Analysis of Government Schemes For Pregnant and Lactating Women in IndiaIJRASETPublicationsNo ratings yet
- Materials 09 01Document47 pagesMaterials 09 01Daniel Vergara ArceNo ratings yet
- Predictors of Knowledge and Practice of Exclusive Breastfeeding Among Health Workers in Mwanza City, Northwest TanzaniaDocument8 pagesPredictors of Knowledge and Practice of Exclusive Breastfeeding Among Health Workers in Mwanza City, Northwest TanzaniaDessy WahyuniNo ratings yet
- ROP Operational Guidelines FINAL PDFDocument58 pagesROP Operational Guidelines FINAL PDFRajan ShuklaNo ratings yet
- Child SurvivalDocument5 pagesChild SurvivalArun Kumar SinghNo ratings yet
- INAP Final PDFDocument84 pagesINAP Final PDFDebasish HembramNo ratings yet
- Operational Guidelines For Facility Based IMNCI (F-IMNCI)Document27 pagesOperational Guidelines For Facility Based IMNCI (F-IMNCI)mohammed RAFINo ratings yet
- Business DevelopemntDocument17 pagesBusiness Developemntayan ghoshNo ratings yet
- Family Welfare ProgrammeDocument19 pagesFamily Welfare ProgrammeMahesh Sahu100% (2)
- Integrated Child Development Services PDFDocument17 pagesIntegrated Child Development Services PDFArchana SahuNo ratings yet
- 03 - Review of LiteratureDocument8 pages03 - Review of LiteratureAbishaNo ratings yet
- Monitoring Public Health Nutrition Capacity DevelopmentDocument10 pagesMonitoring Public Health Nutrition Capacity DevelopmentGina RestianaNo ratings yet
- DOH Programs 1Document21 pagesDOH Programs 1Jarred MatesNo ratings yet
- Jurnal AsiDocument15 pagesJurnal AsiAnastasiaNo ratings yet
- IYCF Book Final 30-01-2018Document96 pagesIYCF Book Final 30-01-2018Hafeez SaleemiNo ratings yet
- F Imnci ManualDocument411 pagesF Imnci Manualvinoth1128No ratings yet
- Session 1 MBFHI A Part of Global Strateegy of MBFHIDocument32 pagesSession 1 MBFHI A Part of Global Strateegy of MBFHItitatabujaraNo ratings yet
- Population Control and Related Population Control ProgrammeDocument37 pagesPopulation Control and Related Population Control ProgrammePinki Barman100% (1)
- Participants Manual ImnciDocument228 pagesParticipants Manual Imncishikhar100% (1)
- Are Our Babies Off To A Healthy Start? The State of Implementation of The Global Strategy For Infant and Young Child Feeding in EuropeDocument12 pagesAre Our Babies Off To A Healthy Start? The State of Implementation of The Global Strategy For Infant and Young Child Feeding in EuropeSukma DewiNo ratings yet
- Vdocument - in Clinical Practice Guidelines Einc 2014Document53 pagesVdocument - in Clinical Practice Guidelines Einc 2014Darla Kay de GuzmanNo ratings yet
- Indonesian Community Health Workers: Roles and Challenges in Breastfeeding PromotionDocument29 pagesIndonesian Community Health Workers: Roles and Challenges in Breastfeeding PromotionAyyu SandhiNo ratings yet
- Feasibility of Implementation of Simplified ManageDocument20 pagesFeasibility of Implementation of Simplified Manageرجاء خاطرNo ratings yet
- Effect of Breastfeeding Promotion Interventions On Breastfeeding Rates, With Special Focus On Developing CountriesDocument8 pagesEffect of Breastfeeding Promotion Interventions On Breastfeeding Rates, With Special Focus On Developing Countriesmphil.rameshNo ratings yet
- RCH - IiDocument18 pagesRCH - IiNeha ShalkarNo ratings yet
- Assesment of Infant and Young Child Feeding (IYCF) Practice - Policy and Programs in EthiopiaDocument42 pagesAssesment of Infant and Young Child Feeding (IYCF) Practice - Policy and Programs in Ethiopiatsehaiassefa100% (1)
- Nutritional Status and Feeding Practices of Students Within The Age of 5-12 Years in Masaba Primary School BidaDocument29 pagesNutritional Status and Feeding Practices of Students Within The Age of 5-12 Years in Masaba Primary School Bidaadeoye abassNo ratings yet
- Colostrum Feeding of Neonants of Recently Delivered Women in Home Based Newborn Care in Uttar Pradesh, IndiaDocument8 pagesColostrum Feeding of Neonants of Recently Delivered Women in Home Based Newborn Care in Uttar Pradesh, IndiaajmrdNo ratings yet
- Operational Guide Enhancing Optimal Infant and Young Child Feeding Practices Through The Public Health SystemDocument70 pagesOperational Guide Enhancing Optimal Infant and Young Child Feeding Practices Through The Public Health SystemJennifer Pearson-ParedesNo ratings yet
- Childhood Obesity: Causes and Consequences, Prevention and Management.From EverandChildhood Obesity: Causes and Consequences, Prevention and Management.No ratings yet
- IELTS 3.5 - Speaking Final (Revision)Document3 pagesIELTS 3.5 - Speaking Final (Revision)Tran PhamNo ratings yet
- Resume (Amzar)Document2 pagesResume (Amzar)amzarhaziqNo ratings yet
- Garmin GTX 330 ManualDocument6 pagesGarmin GTX 330 Manualdannyells_danielsNo ratings yet
- Case Digest - Carpio VS Sulu Resources Development CorporationDocument3 pagesCase Digest - Carpio VS Sulu Resources Development Corporationfred rhyan llausasNo ratings yet
- 2021 Association Implementation Report in GeorgiaDocument20 pages2021 Association Implementation Report in GeorgiaElmaddinNo ratings yet
- 5 WPP Marketing Vs Galera 616 Scra 422Document21 pages5 WPP Marketing Vs Galera 616 Scra 422Arlyn MacaloodNo ratings yet
- FINANCIAL LEVERAGE Gentry Motors Inc. A Producer of Turbine Generators Is in This Situation - EBIT...Document2 pagesFINANCIAL LEVERAGE Gentry Motors Inc. A Producer of Turbine Generators Is in This Situation - EBIT...amrin jannatNo ratings yet
- Creating A Digital Strategy For Nonprofits: A Carousel30 White PaperDocument62 pagesCreating A Digital Strategy For Nonprofits: A Carousel30 White PaperCarlos ForasteroNo ratings yet
- 1 - Kri'at ShemaDocument24 pages1 - Kri'at ShemaAvi HoffmanNo ratings yet
- Prehistoric Age in IndiaDocument8 pagesPrehistoric Age in IndiaSatya GopalNo ratings yet
- Credit To Andrew Kroeze and Cole Gordon For This FrameworkDocument8 pagesCredit To Andrew Kroeze and Cole Gordon For This FrameworkAsdgf FdsgfNo ratings yet
- Exit EssayDocument3 pagesExit Essayapi-249961689No ratings yet
- Thank You Letter For Hospitality at Overseas Technical Visit or TrainingDocument8 pagesThank You Letter For Hospitality at Overseas Technical Visit or Training柯泰德 (Ted Knoy)No ratings yet
- Archigram Architecture Without ArchitectDocument8 pagesArchigram Architecture Without Architect�eljet� BlakajNo ratings yet
- Annual Report Library Management System 2020-2021Document144 pagesAnnual Report Library Management System 2020-2021ARUNAVA SAMANTANo ratings yet
- Aivazian, Ge and Qiu - 2005Document15 pagesAivazian, Ge and Qiu - 2005bildyNo ratings yet
- FN 202 Chapter 4Document38 pagesFN 202 Chapter 4BablooNo ratings yet
- Session Xi (Chapter 9) : Ethical Business For MultibusinessDocument17 pagesSession Xi (Chapter 9) : Ethical Business For MultibusinessJemmyEKONo ratings yet
- NTCP AnalysisDocument12 pagesNTCP AnalysisParas KhuranaNo ratings yet
- Honen The Buddhist Saint-Essential Writings and Official BiographyDocument310 pagesHonen The Buddhist Saint-Essential Writings and Official Biography원왕생願往生No ratings yet
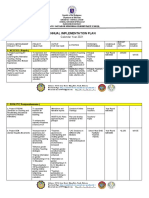
- Annual Implementation Plan: Calendar Year 2021Document5 pagesAnnual Implementation Plan: Calendar Year 2021Guia Marie Diaz BriginoNo ratings yet
- The Long Struggle For A Downtown Central Park: It Is Time For You, The Public, To Speak Once More!Document7 pagesThe Long Struggle For A Downtown Central Park: It Is Time For You, The Public, To Speak Once More!Jamie PittsNo ratings yet
- p3 Business Analysis Case StudyDocument9 pagesp3 Business Analysis Case StudyMangulalNo ratings yet
- BS en Iso 11203-2009Document14 pagesBS en Iso 11203-2009Valentina CoroiNo ratings yet
- Trading Stock Exchange: Presentation On Sip Project ReportDocument20 pagesTrading Stock Exchange: Presentation On Sip Project ReportJayanta 1No ratings yet
- Traditions & Customs of Great BritianDocument3 pagesTraditions & Customs of Great BritianPayvoncu ŞevketNo ratings yet
- Re-Imagining Crotonville:: Epicentre of Ge'S LeadershipDocument7 pagesRe-Imagining Crotonville:: Epicentre of Ge'S LeadershipShalini SarkarNo ratings yet
- Iranian Constitution PDFDocument38 pagesIranian Constitution PDFishana.meadows.23No ratings yet