Download as pdf or txt
You might also like
- A Risk Assessment For Interlock ExecuationDocument11 pagesA Risk Assessment For Interlock ExecuationZubair Khan100% (1)
- Fpsyt 12 659006Document11 pagesFpsyt 12 659006HgokarolNo ratings yet
- Brainsci 14 00136Document38 pagesBrainsci 14 00136VICTOR JESUS GARCIA HERNANDEZNo ratings yet
- 2021 NF e AutismoDocument7 pages2021 NF e AutismoMarcelo MenezesNo ratings yet
- J Ejpn 2016 07 004Document13 pagesJ Ejpn 2016 07 004Gisele Elise MeninNo ratings yet
- Sleep Phenotypes in Attention Deficit Hyperactivity DisorderDocument35 pagesSleep Phenotypes in Attention Deficit Hyperactivity DisorderPierluigi CongedoNo ratings yet
- NeurofeedbackDocument6 pagesNeurofeedbackVildana BesirevicNo ratings yet
- Sleep-Related Disorders in Children With Attention-Deficit Hyperactivity Disorder: Preliminary Results of A Full Sleep Assessment StudyDocument9 pagesSleep-Related Disorders in Children With Attention-Deficit Hyperactivity Disorder: Preliminary Results of A Full Sleep Assessment StudyPierluigi CongedoNo ratings yet
- Abnormal Sleep Physiology in Children With 15q11.2-13.1 Duplication (Dup15q) SyndromeDocument14 pagesAbnormal Sleep Physiology in Children With 15q11.2-13.1 Duplication (Dup15q) SyndromeAmr Mohamed GalalNo ratings yet
- Friedman 2015Document6 pagesFriedman 2015Mariana SáNo ratings yet
- Fnins 15 747273 PDFDocument10 pagesFnins 15 747273 PDFAndreia SilvaNo ratings yet
- QEEG Spectral and Coherence Assessment of Autistic Children in Three Different Experimental ConditionsDocument19 pagesQEEG Spectral and Coherence Assessment of Autistic Children in Three Different Experimental ConditionsFrontiersNo ratings yet
- Psychiatry Research: A A A A A A A B C D A BDocument6 pagesPsychiatry Research: A A A A A A A B C D A BArlindo Goncalves De Araujo NetoNo ratings yet
- The Sleep Phenotypes of Attention Deficit Hyperactivity Disorder: The Role of Arousal During Sleep and Implications For TreatmentDocument7 pagesThe Sleep Phenotypes of Attention Deficit Hyperactivity Disorder: The Role of Arousal During Sleep and Implications For TreatmentPierluigi CongedoNo ratings yet
- A Review of Fronto-Striatal and Fronto-Cortical Brain Abnormalities in Children and Adults With Attention Deficit Hyperactivity Disorder.Document22 pagesA Review of Fronto-Striatal and Fronto-Cortical Brain Abnormalities in Children and Adults With Attention Deficit Hyperactivity Disorder.Víctor RománNo ratings yet
- DNB Vol35 No1 27Document6 pagesDNB Vol35 No1 27Emir BegagićNo ratings yet
- Aberrant Functional Connectivity of Neural Circuits Associated With Social and Sensorimotor Deficits in Young Children With Autism Spectrum DisorderDocument21 pagesAberrant Functional Connectivity of Neural Circuits Associated With Social and Sensorimotor Deficits in Young Children With Autism Spectrum DisorderTaNiTa TiKaRaNNo ratings yet
- Functional Connectome Mediates The Association BetDocument10 pagesFunctional Connectome Mediates The Association Betccaneccorso1971 ŻukowskaNo ratings yet
- Hurdles PrintedDocument14 pagesHurdles PrintedAlice MaulisovaNo ratings yet
- Sleep Studies in ChildrenDocument12 pagesSleep Studies in ChildrenJHONATAN MATA ARANDANo ratings yet
- tmp7256 TMPDocument11 pagestmp7256 TMPFrontiersNo ratings yet
- 2005 Atypical Sleep Architecture and The Autism PhenotypeDocument13 pages2005 Atypical Sleep Architecture and The Autism PhenotypePsic ClinicaNo ratings yet
- Geographic Variation in The Prevalence of Attention-Deficit/Hyperactivity Disorder: The Sunny PerspectiveDocument6 pagesGeographic Variation in The Prevalence of Attention-Deficit/Hyperactivity Disorder: The Sunny PerspectiveAndrea ReisNo ratings yet
- Neurostimulation-techniques-to-enhance-sleep-and-improve-cognition-in-agingDocument16 pagesNeurostimulation-techniques-to-enhance-sleep-and-improve-cognition-in-agingPrakash N KNo ratings yet
- Konrad 2006Document9 pagesKonrad 2006jaimeaguilarr97No ratings yet
- Sleep Problems and Disorders Among Adolescents With Persistent and Subthreshold Attention-deficit/Hyperactivity DisordersDocument9 pagesSleep Problems and Disorders Among Adolescents With Persistent and Subthreshold Attention-deficit/Hyperactivity DisordersdentistwaseemNo ratings yet
- Penelitian 2Document9 pagesPenelitian 2dietapNo ratings yet
- Amico F Et Al (2023) A Resting State EEG Study On Depressed Persons With Suicidal Ideation IBRO Neuroscience ReportsDocument7 pagesAmico F Et Al (2023) A Resting State EEG Study On Depressed Persons With Suicidal Ideation IBRO Neuroscience ReportsAlparslan OnderNo ratings yet
- Journal of Sleep Research - 2016 - Lucey - Comparison of A Single Channel EEG Sleep Study To PolysomnographyDocument11 pagesJournal of Sleep Research - 2016 - Lucey - Comparison of A Single Channel EEG Sleep Study To PolysomnographyIoana GuțăNo ratings yet
- Skizofrenia - Agy DinamikaDocument20 pagesSkizofrenia - Agy DinamikaEdl ZsuzsiNo ratings yet
- 2013-Buckley-First Night Effect Analysis in A Cohort of Young Children With ASDDocument4 pages2013-Buckley-First Night Effect Analysis in A Cohort of Young Children With ASDPsic ClinicaNo ratings yet
- Jurnal Psikiatri 03Document20 pagesJurnal Psikiatri 03Ike DekockNo ratings yet
- Biomedical Journal: SciencedirectDocument8 pagesBiomedical Journal: SciencedirectCarlosToledoNo ratings yet
- 2014 Reappraisal of Abnormal EEG Findings in Children With ADHD. On The Relationship Between ADHD and Epileptiform DischargesDocument6 pages2014 Reappraisal of Abnormal EEG Findings in Children With ADHD. On The Relationship Between ADHD and Epileptiform DischargesPiotr BuczkowiczNo ratings yet
- Tdah 1Document8 pagesTdah 1Roberto Alexis Molina CampuzanoNo ratings yet
- Fneur 11 00144Document22 pagesFneur 11 00144ilonaskorinNo ratings yet
- 1 s2.0 S1389945721002380 MainDocument9 pages1 s2.0 S1389945721002380 MainHafizhah AlhusnaNo ratings yet
- Neurophysiological Recordings Improve The Accuracy of 2022 European JournalDocument6 pagesNeurophysiological Recordings Improve The Accuracy of 2022 European Journalcsepulveda10No ratings yet
- TMP DF97Document14 pagesTMP DF97FrontiersNo ratings yet
- Librodeabstracts1 PDFDocument372 pagesLibrodeabstracts1 PDFqalbiNo ratings yet
- Sueño CognicionDocument11 pagesSueño CognicionGonzaloSebastianRojasFaúndezNo ratings yet
- Visualization of EEG Data To Detect ADHD in Children and AdultsDocument5 pagesVisualization of EEG Data To Detect ADHD in Children and AdultsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- EBJ ArticleDocument7 pagesEBJ ArticleKhristle DavidNo ratings yet
- Yanpei Wang Et Al (Ref12)Document10 pagesYanpei Wang Et Al (Ref12)Claudia Calipso Gutiérrez HernándezNo ratings yet
- Wylei Et Al., Hippocampal Basal Ganglia and Olfatory Connectivity Contribute To Cognitive Impairments in PDDocument17 pagesWylei Et Al., Hippocampal Basal Ganglia and Olfatory Connectivity Contribute To Cognitive Impairments in PDUriel BühlerNo ratings yet
- Pi Is 1525505023004006Document10 pagesPi Is 1525505023004006beck-ydNo ratings yet
- J of Neuroscience Research - 2022 - Valli - Neuroimaging of Rapid Eye Movement Sleep Behavior Disorder and Its Relation ToDocument20 pagesJ of Neuroscience Research - 2022 - Valli - Neuroimaging of Rapid Eye Movement Sleep Behavior Disorder and Its Relation ToKaramjot SinghNo ratings yet
- Neuropsychological Profile Associated To PKAN in Its Initial Phase A Case Series ReportDocument7 pagesNeuropsychological Profile Associated To PKAN in Its Initial Phase A Case Series ReportNataly CastañedaNo ratings yet
- Visual Attention and Poor Sleep Quality: Amirhussein Abdolalizadeh and Samaneh NabaviDocument12 pagesVisual Attention and Poor Sleep Quality: Amirhussein Abdolalizadeh and Samaneh Nabaviprapti.mohantyNo ratings yet
- Assessment-Guided Neurofeedback For Autistic SpectDocument50 pagesAssessment-Guided Neurofeedback For Autistic Spectminami.heartful.dayNo ratings yet
- Brand 2015Document10 pagesBrand 2015Messias FilhoNo ratings yet
- REM Sleep Behaviour DisorderDocument4 pagesREM Sleep Behaviour DisorderMuhammad Bilal SaifulhaqNo ratings yet
- Biomarker Support For ADHD Diagnosis Based On Event Related Potentials and Scores From An Attention TestDocument9 pagesBiomarker Support For ADHD Diagnosis Based On Event Related Potentials and Scores From An Attention TestGema PSNo ratings yet
- The "when" and "where" of α-synucleinopathies: Insights from REM sleep behavior disorderDocument3 pagesThe "when" and "where" of α-synucleinopathies: Insights from REM sleep behavior disorderSandsackNo ratings yet
- Neural Plasticity - 2023 - Huang - Assessment of Cognitive Function With Sleep Spindle Characteristics in Adults WithDocument26 pagesNeural Plasticity - 2023 - Huang - Assessment of Cognitive Function With Sleep Spindle Characteristics in Adults WithCata Marimon SierraNo ratings yet
- Resting-State EEG Microstates and Power Spectrum IDocument14 pagesResting-State EEG Microstates and Power Spectrum IChu Thị NghiệpNo ratings yet
- EEG Complexity As A Biomarker For Autism Spectrum Disorder RiskDocument16 pagesEEG Complexity As A Biomarker For Autism Spectrum Disorder RiskRafael MartinsNo ratings yet
- 03 - Resting-State Electroencephalographic Oscillations in Patients With Alzheimer's DiseaseDocument7 pages03 - Resting-State Electroencephalographic Oscillations in Patients With Alzheimer's Diseaseheineken2012No ratings yet
- ArchMentHealth232129-3871856 104518Document4 pagesArchMentHealth232129-3871856 104518dkumar_100No ratings yet
- NGS_biothreat_applicationsDocument10 pagesNGS_biothreat_applicationsKrisztián TóthNo ratings yet
- NGSplatforms_metagenomic_blood_pathogensDocument14 pagesNGSplatforms_metagenomic_blood_pathogensKrisztián TóthNo ratings yet
- NGS_in_clinmicrob_genes-13-01566Document24 pagesNGS_in_clinmicrob_genes-13-01566Krisztián TóthNo ratings yet
- mgNGS_clinmicrob_watts2020Document7 pagesmgNGS_clinmicrob_watts2020Krisztián TóthNo ratings yet
- 1-s2.0-S0197458019301083-mainDocument12 pages1-s2.0-S0197458019301083-mainKrisztián TóthNo ratings yet
- WHO Influenza PrimersDocument1 pageWHO Influenza PrimersKrisztián TóthNo ratings yet
- Bulletin: Medical University of InnsbruckDocument5 pagesBulletin: Medical University of InnsbruckKrisztián TóthNo ratings yet
- Cytokines: Names and Numbers You Should Care About: Stephen R. Holdsworth and Poh-Yi GanDocument12 pagesCytokines: Names and Numbers You Should Care About: Stephen R. Holdsworth and Poh-Yi GanKrisztián TóthNo ratings yet
- Opal2000 PDFDocument11 pagesOpal2000 PDFKrisztián TóthNo ratings yet
- Batch PurificationDocument1 pageBatch Purificationsams shuvoNo ratings yet
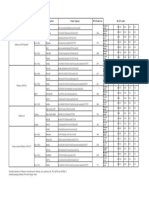
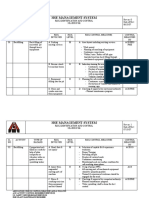
- TTEC Fencing RADocument7 pagesTTEC Fencing RAGeml TrinidadNo ratings yet
- Un ScriptDocument2 pagesUn ScriptPeterClomaJr.No ratings yet
- Denali Partners With Amazon and Providence To Get Oxygen and Vaccines To Employees and Hospitals in IndiaDocument3 pagesDenali Partners With Amazon and Providence To Get Oxygen and Vaccines To Employees and Hospitals in IndiaPR.comNo ratings yet
- Episiotomy ACOGDocument29 pagesEpisiotomy ACOGMike67% (3)
- Cytotoxicity of Different Composite Resins On Human Gingival Fibroblast Cell LinesDocument8 pagesCytotoxicity of Different Composite Resins On Human Gingival Fibroblast Cell LinesLavinia GheorghitaNo ratings yet
- Q2 - 2ND SEM WLP RWS WEEK 1 Day2Document22 pagesQ2 - 2ND SEM WLP RWS WEEK 1 Day2JAVELOSA, YUAN ALDRICH M.No ratings yet
- Final Draft of Moot Court On Transgender Right (Final)Document27 pagesFinal Draft of Moot Court On Transgender Right (Final)aarzoo6khanNo ratings yet
- Used CHN Week 1Document37 pagesUsed CHN Week 1John paolo TiglaoNo ratings yet
- NCM 107 1Document3 pagesNCM 107 1jellybeandumpppNo ratings yet
- GEMMW Graph Theory (GROUP 4)Document6 pagesGEMMW Graph Theory (GROUP 4)Jenn TajanlangitNo ratings yet
- Case Study of PneumoniaDocument8 pagesCase Study of PneumoniaAnne SedanzaNo ratings yet
- Risk Assessment of BackfillingDocument2 pagesRisk Assessment of BackfillingPrasanta ParidaNo ratings yet
- Current Views of Scapular Dyskinesis and Its Possible Clinical RelevanceDocument14 pagesCurrent Views of Scapular Dyskinesis and Its Possible Clinical RelevanceRoshani PNo ratings yet
- Dentistry For General Medicine: - Part 2 - Dental SurgeryDocument52 pagesDentistry For General Medicine: - Part 2 - Dental SurgeryDimitrios PapadopoulosNo ratings yet
- The Immortal Life of Henrietta Lacks PDFDocument2 pagesThe Immortal Life of Henrietta Lacks PDFShashidhar BagewadiNo ratings yet
- Effective Methods of SELF-HYPNOSIS - 2021 How To Hypnotize Yourself With Your Eyes OpenDocument40 pagesEffective Methods of SELF-HYPNOSIS - 2021 How To Hypnotize Yourself With Your Eyes Openlance wong100% (1)
- Tooth Implant Supported Prosthesis: A Literature ReviewDocument8 pagesTooth Implant Supported Prosthesis: A Literature ReviewTung Thanh NguyenNo ratings yet
- Scaohoid Fracture 4Document34 pagesScaohoid Fracture 4Noor Al Zahraa Ali100% (1)
- TEC-030100.2-MET-DoR-003-MAT-TDS-BASF-Concresive 1414Document3 pagesTEC-030100.2-MET-DoR-003-MAT-TDS-BASF-Concresive 1414Eli MatucadNo ratings yet
- GP-IR by Mrithiks.V.GDocument7 pagesGP-IR by Mrithiks.V.GMrithika VNo ratings yet
- RhabdomyolysisDocument15 pagesRhabdomyolysisPriyanka MkNo ratings yet
- Cardiovascular Safety of Naltrexone and Bupropion Therapy Systematic Review and Meta-AnalysesDocument9 pagesCardiovascular Safety of Naltrexone and Bupropion Therapy Systematic Review and Meta-AnalysesPlinio ReisNo ratings yet
- Skinner - Operant Conditioning PDFDocument12 pagesSkinner - Operant Conditioning PDFArnt van HeldenNo ratings yet
- Gonzalez C2 4Document71 pagesGonzalez C2 4tolatillerNo ratings yet
- CHN FinalDocument41 pagesCHN FinalKeziah Marie Chua Santa-AnaNo ratings yet
- 11 14 Case ProformaDocument13 pages11 14 Case Proformaanilbm1976No ratings yet
- Material Safety Data Sheet DynaplugDocument4 pagesMaterial Safety Data Sheet Dynaplugfs1640No ratings yet
- AuditDocument5 pagesAuditPatNo ratings yet