Download as pdf or txt
You might also like
- The Iaq Investigator's GuideDocument86 pagesThe Iaq Investigator's GuideatenguezNo ratings yet
- Stefano Malinverni A Retrospective Comparison ofDocument8 pagesStefano Malinverni A Retrospective Comparison ofAssessoria da Gerência Geral HEHANo ratings yet
- Driving Pressure–Guided Individualized Positive End-Expiratory Pressure in Abdominal SurgeryDocument9 pagesDriving Pressure–Guided Individualized Positive End-Expiratory Pressure in Abdominal SurgeryhubertandharrietNo ratings yet
- The Effects of Lung Recruitment On The Phase III.26Document9 pagesThe Effects of Lung Recruitment On The Phase III.26Fermin LombardiaNo ratings yet
- Med 9780199600830 Chapter 97Document7 pagesMed 9780199600830 Chapter 97Kiki Sri Rejeki AgisinaNo ratings yet
- Original ResearchDocument8 pagesOriginal ResearchEduardo SoaresNo ratings yet
- Autoflow in SopDocument7 pagesAutoflow in SopBryan MaldonadoNo ratings yet
- Cpap Vs Vni - PasquinaDocument8 pagesCpap Vs Vni - PasquinaMelina AlcaineNo ratings yet
- ResuscitationDocument8 pagesResuscitation85tq5nhsqbNo ratings yet
- VitaminaDocument15 pagesVitaminaCarinka VidañosNo ratings yet
- Atelectasias en ObesosDocument6 pagesAtelectasias en ObesosHernan Dario GuerreroNo ratings yet
- Rway Clearance in The Intensive Care UnitDocument5 pagesRway Clearance in The Intensive Care UnitPAC MINDOMONo ratings yet
- Effects of Lung Expansion Therapy On Lung Function in Patients With Prolonged Mechanical VentilationDocument7 pagesEffects of Lung Expansion Therapy On Lung Function in Patients With Prolonged Mechanical Ventilationcard breatheNo ratings yet
- Effects of Ventilatory Mode During One-Lung Ventilation on Intraoperative and Postoperative Arterial Oxygenation in Thoracic SurgeryDocument5 pagesEffects of Ventilatory Mode During One-Lung Ventilation on Intraoperative and Postoperative Arterial Oxygenation in Thoracic SurgeryhubertandharrietNo ratings yet
- Effect of Patient-Triggered Ventilation On RespiratoryDocument7 pagesEffect of Patient-Triggered Ventilation On RespiratoryBryan MaldonadoNo ratings yet
- Definisi MVDocument7 pagesDefinisi MVArmi ZakaNo ratings yet
- Current Trends in Anesthesia For Esophagectomy 2017Document6 pagesCurrent Trends in Anesthesia For Esophagectomy 2017Ajay Varun ReddyNo ratings yet
- Noninvasive Positive Pressure Ventilation - Successful Outcome in Patients With Acute Lung Injury ARDSDocument6 pagesNoninvasive Positive Pressure Ventilation - Successful Outcome in Patients With Acute Lung Injury ARDSpaulina mancilla ramirezNo ratings yet
- CLN 66 01 107 PDFDocument5 pagesCLN 66 01 107 PDFGloria KartikaNo ratings yet
- Peep y EntrenamientoDocument6 pagesPeep y EntrenamientoCamila Cisternas FloresNo ratings yet
- The ABC of Weaning Failure - A Structured ApproachDocument9 pagesThe ABC of Weaning Failure - A Structured ApproachArul ShanmugamNo ratings yet
- Medical Hypotheses: Jian-Qiao Zheng, Li Du, Lu Zhang, Bin DuDocument4 pagesMedical Hypotheses: Jian-Qiao Zheng, Li Du, Lu Zhang, Bin DuABC DFGHINo ratings yet
- s1013 70252970039 9Document8 pagess1013 70252970039 9ganesh goreNo ratings yet
- Pham - Esophageal ManometryDocument21 pagesPham - Esophageal ManometryAbraham HaneineNo ratings yet
- Volume-Targeted Modes of Modern Neonatal Ventilators: How Stable Is The Delivered Tidal Volume?Document10 pagesVolume-Targeted Modes of Modern Neonatal Ventilators: How Stable Is The Delivered Tidal Volume?DawoodNo ratings yet
- Intrapulmonary Percussion With Autogenic Drainage and Ventilator-Associated Gram-Negative Infection: A Pilot StudyDocument5 pagesIntrapulmonary Percussion With Autogenic Drainage and Ventilator-Associated Gram-Negative Infection: A Pilot StudyJulenda CintarinovaNo ratings yet
- Non-Invasive Positive Pressure Ventilation in Acute Respiratory Failure: Providing Competent CareDocument9 pagesNon-Invasive Positive Pressure Ventilation in Acute Respiratory Failure: Providing Competent CareAndana TrisaviNo ratings yet
- Lung and Diaphragm Protective Ventilation Guided by The EsophagealDocument3 pagesLung and Diaphragm Protective Ventilation Guided by The Esophagealema moralesNo ratings yet
- Systemic and Alveolar Inflammatory Response in the Dependent and Nondependent Lung in Patients Undergoing Lung Resection SurgeryDocument9 pagesSystemic and Alveolar Inflammatory Response in the Dependent and Nondependent Lung in Patients Undergoing Lung Resection SurgeryhubertandharrietNo ratings yet
- Nippv CCDocument13 pagesNippv CCcnvNo ratings yet
- Protective Ventilation During Anaesthesia Reduces Major Postoperative Complications After Lung Cancer SurgeryDocument9 pagesProtective Ventilation During Anaesthesia Reduces Major Postoperative Complications After Lung Cancer SurgeryhubertandharrietNo ratings yet
- Severgnini 2013Document15 pagesSevergnini 2013moraeunwprqphslndfNo ratings yet
- Ventilación Del Pulmón Sano CC Current 20Document5 pagesVentilación Del Pulmón Sano CC Current 20Silvia Lorena Mireles GonzálezNo ratings yet
- Von Goedecke Et Al 2004 Positive Pressure Versus Pressure Support Ventilation at Different Levels of Peep Using TheDocument5 pagesVon Goedecke Et Al 2004 Positive Pressure Versus Pressure Support Ventilation at Different Levels of Peep Using TheDr MunawarNo ratings yet
- Journal of Anesthesia & Clinical ResearchDocument8 pagesJournal of Anesthesia & Clinical ResearchAyu Aprilisa D PutriNo ratings yet
- (03241750 - Acta Medica Bulgarica) Application of Positive End-Expiratory Pressure (PEEP) in Patients During Prolonged Gynecological SurgeryDocument6 pages(03241750 - Acta Medica Bulgarica) Application of Positive End-Expiratory Pressure (PEEP) in Patients During Prolonged Gynecological SurgeryTeodorNo ratings yet
- Speaking ValveDocument6 pagesSpeaking ValveJonssito Griffin Iglesias PerezNo ratings yet
- Jurnal Dari Aak 4Document8 pagesJurnal Dari Aak 4rifqi rizalNo ratings yet
- Novel Forms of Ventilation in Neonates Neurally Adjusted VentilatoryDocument16 pagesNovel Forms of Ventilation in Neonates Neurally Adjusted VentilatorydocsaravananNo ratings yet
- Gonzalez2003 Article AirLeaksDuringMechanicalVentilDocument7 pagesGonzalez2003 Article AirLeaksDuringMechanicalVentilLuis Miguel MartinsNo ratings yet
- Papazian2022 Article PronePositionInMechanicallyVenDocument4 pagesPapazian2022 Article PronePositionInMechanicallyVenA. RaufNo ratings yet
- Ventilation During Lung Resection and Critical Care ComparativeDocument11 pagesVentilation During Lung Resection and Critical Care Comparativeema moralesNo ratings yet
- Mauri 2017 - Optimum Support by High Flow Nasal Cannula in AHRFDocument11 pagesMauri 2017 - Optimum Support by High Flow Nasal Cannula in AHRFgiadungdanamallNo ratings yet
- Hfo 2Document9 pagesHfo 2markus_danusantosoNo ratings yet
- Research: Ido G Bikker, Jasper Van Bommel, Dinis Reis Miranda, Jan Bakker and Diederik GommersDocument6 pagesResearch: Ido G Bikker, Jasper Van Bommel, Dinis Reis Miranda, Jan Bakker and Diederik GommersJavier Enrique Barrera PachecoNo ratings yet
- Dronkers Et Al 2008 Prevention of Pulmonary Complications After Upper Abdominal Surgery by Preoperative IntensiveDocument9 pagesDronkers Et Al 2008 Prevention of Pulmonary Complications After Upper Abdominal Surgery by Preoperative Intensivechiendy.yNo ratings yet
- Lung Insufflation Capacity in Neuromuscular Disease: Original Research ArticleDocument6 pagesLung Insufflation Capacity in Neuromuscular Disease: Original Research ArticleEzeBorjesNo ratings yet
- 5 KremerDocument6 pages5 KremerFabiola Novita SariNo ratings yet
- Mechanical Ventilator Discontinuation Process: Lingye Chen,, Daniel Gilstrap,, Christopher E. CoxDocument7 pagesMechanical Ventilator Discontinuation Process: Lingye Chen,, Daniel Gilstrap,, Christopher E. CoxGhost11mNo ratings yet
- Influence of The Cuff Pressure On The Swallowing Reflex in Tracheostomized Intensive Care Unit PatientsDocument6 pagesInfluence of The Cuff Pressure On The Swallowing Reflex in Tracheostomized Intensive Care Unit PatientscamiladelgadomNo ratings yet
- Postoperative Noninvasive Ventilation: Samir Jaber, M.D., PH.D., Gerald Chanques, M.D., Boris Jung, M.D.Document9 pagesPostoperative Noninvasive Ventilation: Samir Jaber, M.D., PH.D., Gerald Chanques, M.D., Boris Jung, M.D.lilalala4123No ratings yet
- In Support of Pressure Support: Subrata Sarkar, MD, Steven M. Donn, MDDocument12 pagesIn Support of Pressure Support: Subrata Sarkar, MD, Steven M. Donn, MDSiska LesnussaNo ratings yet
- Clinical Review: Hemodynamic Monitoring in The Intensive Care UnitDocument8 pagesClinical Review: Hemodynamic Monitoring in The Intensive Care Unitmasfak97No ratings yet
- Conventional Chest Physical Therapy For Obstructive Lung DiseaseDocument12 pagesConventional Chest Physical Therapy For Obstructive Lung DiseaseJulieta EvangelistaNo ratings yet
- 13 COM TRADU+ç+âODocument9 pages13 COM TRADU+ç+âOEduardo SoaresNo ratings yet
- Critical Care Clinical Procedures 2023Document38 pagesCritical Care Clinical Procedures 2023nucahersheyskatNo ratings yet
- Como Optimizar La EntubaciónDocument4 pagesComo Optimizar La EntubaciónKaren Aline Gómez CruzNo ratings yet
- Impact of Ventilation Strategies On Pulmonary andDocument9 pagesImpact of Ventilation Strategies On Pulmonary andVictoria San MartinNo ratings yet
- Original Article: Comparison of Echocardiographic Indices Used To Predict Fluid Responsiveness in Ventilated PatientsDocument11 pagesOriginal Article: Comparison of Echocardiographic Indices Used To Predict Fluid Responsiveness in Ventilated Patientszpm70717No ratings yet
- PEEP guided by electrical impedance tomography during one-lung ventilation in elderly patients undergoing thoracoscopic surgeryDocument12 pagesPEEP guided by electrical impedance tomography during one-lung ventilation in elderly patients undergoing thoracoscopic surgeryhubertandharrietNo ratings yet
- Monitoring Mechanical Ventilation Using Ventilator WaveformsFrom EverandMonitoring Mechanical Ventilation Using Ventilator WaveformsNo ratings yet
- Shame and Silence in The Aftermath of War Rape in Bosnia and Herzegovina: 22 Years LaterDocument23 pagesShame and Silence in The Aftermath of War Rape in Bosnia and Herzegovina: 22 Years LaterMomina AbbasiNo ratings yet
- MS Ii MT2Document11 pagesMS Ii MT2Rika MaeNo ratings yet
- PDRRMO LagunaDocument2 pagesPDRRMO LagunaAlexadnerNo ratings yet
- Retinaldetachmentnew WORSDocument51 pagesRetinaldetachmentnew WORSMuthulakshmiNo ratings yet
- Multiple and Mixed Valvular Heart DiseaseDocument13 pagesMultiple and Mixed Valvular Heart DiseaseВенцислав МирчевNo ratings yet
- Pregnancy With Previous LSCS: Vishal Final YearDocument21 pagesPregnancy With Previous LSCS: Vishal Final YearAdit RockNo ratings yet
- Oncology Work Plan For Students 2022-2023Document34 pagesOncology Work Plan For Students 2022-2023Ahmed SaeedNo ratings yet
- Jan Gulliver-Kline - Website BioDocument1 pageJan Gulliver-Kline - Website Bioapi-217498783No ratings yet
- Bladder Catheterisation PDFDocument12 pagesBladder Catheterisation PDFSonish KhatriNo ratings yet
- Antihistamines: Author: Kimberly Mulcahy, Pharmd, Bcps Editor: Claudia Lee, RPH, MDDocument16 pagesAntihistamines: Author: Kimberly Mulcahy, Pharmd, Bcps Editor: Claudia Lee, RPH, MDHassan Ait YachouNo ratings yet
- MPH Program in UP ManilaDocument2 pagesMPH Program in UP ManilaHannah Marquiala PellejoNo ratings yet
- Pasteur Vs Bechamp - An Alternative View of Infectious DiseaseDocument3 pagesPasteur Vs Bechamp - An Alternative View of Infectious DiseaseRadhe GovindaNo ratings yet
- Hydrotherapy Indi ContraDocument71 pagesHydrotherapy Indi Contrateam7MFkkOP YTNo ratings yet
- Anesthesia Management of Pregnant With HELLP Syndrome With Fetal Intrauterine Exitus (#1123666) - 2457074Document3 pagesAnesthesia Management of Pregnant With HELLP Syndrome With Fetal Intrauterine Exitus (#1123666) - 2457074SALMA HANINANo ratings yet
- Listening Skills Practice: The Fear Factor - Exercises: PreparationDocument3 pagesListening Skills Practice: The Fear Factor - Exercises: PreparationAmir AslanNo ratings yet
- The Structure and Function of The Ear and Its Role in Hearing and Balance1Document4 pagesThe Structure and Function of The Ear and Its Role in Hearing and Balance1Khushbakht QureshiNo ratings yet
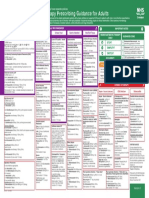
- Empirical Antimicrobial Therapy Prescribing Guidance For AdultsDocument1 pageEmpirical Antimicrobial Therapy Prescribing Guidance For AdultsPsychology TodayNo ratings yet
- MS GCS Cornual Ectopic PregnancyDocument57 pagesMS GCS Cornual Ectopic PregnancyCarelle Faith Serrano AsuncionNo ratings yet
- Prosthodontic Implant DrivenDocument7 pagesProsthodontic Implant DrivenbuccalNo ratings yet
- Ophthalmology Diseases of Eye Ilmu Kesehatan Mata: Putu BudhiastraDocument45 pagesOphthalmology Diseases of Eye Ilmu Kesehatan Mata: Putu BudhiastraPande Indra PremanaNo ratings yet
- Letterstream 2024 2Document76 pagesLetterstream 2024 2swagswogNo ratings yet
- The Scale of Perceived Occupational StressDocument6 pagesThe Scale of Perceived Occupational StressPranay PandeyNo ratings yet
- Nursingcrib Com Nursing Care Plan Congestive Heart Failure PDFDocument2 pagesNursingcrib Com Nursing Care Plan Congestive Heart Failure PDFnadzwa velascoNo ratings yet
- Unit 4 Endoscopy Bronchoscopy LaporosDocument115 pagesUnit 4 Endoscopy Bronchoscopy LaporosAC19UBM035 SOWMIYA.PNo ratings yet
- Anterior Segment Optical Coherence Tomography Angiography Imaging of Conjunctiva and Intrasclera in Treated Primary Open-Angle GlaucomaDocument10 pagesAnterior Segment Optical Coherence Tomography Angiography Imaging of Conjunctiva and Intrasclera in Treated Primary Open-Angle GlaucomaPatzy VasquezNo ratings yet
- Epidemiology and Public HealthDocument21 pagesEpidemiology and Public HealthFatima Sumabat100% (1)
- LC460 Wellbeing in SocietyDocument12 pagesLC460 Wellbeing in Societyayan biswasNo ratings yet
- Effect of Temperature On FrogDocument2 pagesEffect of Temperature On FrogPrerna DubeyNo ratings yet
- ACOG Fetal Maturity Guidelines PDFDocument8 pagesACOG Fetal Maturity Guidelines PDFinayahsyNo ratings yet