Download as pdf or txt
You might also like
- 2012 BLS HCP Exam Binder C and D 01 20 2012Document19 pages2012 BLS HCP Exam Binder C and D 01 20 2012Chandler Bearden100% (2)
- Ils MCQ Paper BTLDocument4 pagesIls MCQ Paper BTLmariamNo ratings yet
- Physiotherapy in General Surgical ConditionDocument7 pagesPhysiotherapy in General Surgical Conditionprofpt98100% (8)
- Walls 8093 CH 01Document7 pagesWalls 8093 CH 01Adriana MartinezNo ratings yet
- COPD Acute Management ABCDEDocument11 pagesCOPD Acute Management ABCDESS100% (1)
- ABCDE Approach To Emergency ManagementDocument20 pagesABCDE Approach To Emergency Managementluq9fifNo ratings yet
- Rapid Sequence Intubation: BackgroundDocument8 pagesRapid Sequence Intubation: Backgroundmarsh86No ratings yet
- Emergency Endotracheal Intubation in Children - UpToDateDocument63 pagesEmergency Endotracheal Intubation in Children - UpToDatedr_comNo ratings yet
- Maxillofacial Trauma: Dr. Azher A. Auda Bds CabsDocument17 pagesMaxillofacial Trauma: Dr. Azher A. Auda Bds CabsHaider F YehyaNo ratings yet
- Rapid Sequence Intubation ReportDocument55 pagesRapid Sequence Intubation Reportlorkan19100% (1)
- Airway ManagementDocument11 pagesAirway Managementmegayani santosoNo ratings yet
- Airway and Ventilatory ManagementDocument8 pagesAirway and Ventilatory ManagementAshen DissanayakaNo ratings yet
- NEJM VICM Viewers ChoiceDocument19 pagesNEJM VICM Viewers ChoiceAnonymous cQWavnNo ratings yet
- Airway Assessment & Management of Primary Trauma SurveyDocument91 pagesAirway Assessment & Management of Primary Trauma SurveyNabighah ZukriNo ratings yet
- Basic Airway Management in AdultsDocument7 pagesBasic Airway Management in AdultsBereket temesgenNo ratings yet
- Acute Stridor in ChildrenDocument6 pagesAcute Stridor in Childrenmob3No ratings yet
- 3 Eecc Care AbcdeDocument12 pages3 Eecc Care AbcdeEduardo GarciaNo ratings yet
- Respiratory PresentationDocument137 pagesRespiratory Presentationakoeljames8543No ratings yet
- The ABCDE ApproachDocument4 pagesThe ABCDE Approachazmar3No ratings yet
- The Decision To IntubateDocument11 pagesThe Decision To Intubatesergio salazarNo ratings yet
- Anafilaxia Uptodate 2024 Anaphylaxis Emergency TreatmentDocument23 pagesAnafilaxia Uptodate 2024 Anaphylaxis Emergency Treatmentdemr1294No ratings yet
- Adult and Paediatric Oral/nasal-Pharyngeal SuctioningDocument13 pagesAdult and Paediatric Oral/nasal-Pharyngeal SuctioningRuby Dela RamaNo ratings yet
- Emergency in DentalDocument6 pagesEmergency in Dentalpuskesmas sedatiNo ratings yet
- ABCDE Approach PDFDocument3 pagesABCDE Approach PDFJohn SmithNo ratings yet
- Basic Airway ManagementDocument24 pagesBasic Airway ManagementFELIPE MEDINANo ratings yet
- Endotracheal TubeDocument19 pagesEndotracheal TubeSarvess Muniandy100% (1)
- Care of The Ventilated ChildDocument5 pagesCare of The Ventilated ChildBrahadheeswaran KannanNo ratings yet
- Airway / Breathing ProtocolsDocument15 pagesAirway / Breathing ProtocolsSbarcea AurelNo ratings yet
- Resuscitation GuidelinesDocument5 pagesResuscitation GuidelinesGemmith GosanesNo ratings yet
- Syncope:: The Most Common Medical Emergency in Dentistry Is Syncope, and The MostDocument3 pagesSyncope:: The Most Common Medical Emergency in Dentistry Is Syncope, and The Mostomar alahmariNo ratings yet
- Opioid Overdose - Acute Management - ABCDE - Geeky MedicsDocument13 pagesOpioid Overdose - Acute Management - ABCDE - Geeky MedicslortifukkuNo ratings yet
- ABCDE Approach PDFDocument3 pagesABCDE Approach PDFIrsan apatisNo ratings yet
- The Decision To Intubate - UpToDateDocument11 pagesThe Decision To Intubate - UpToDateBogdanBudusanNo ratings yet
- Basic Airway Management in Adults - UpToDateDocument28 pagesBasic Airway Management in Adults - UpToDateGia Villavicencio BoniniNo ratings yet
- Airway Management and Common ConditionsDocument34 pagesAirway Management and Common Conditionsrigo montejoNo ratings yet
- Airway ObstructionDocument7 pagesAirway ObstructionnesredeNo ratings yet
- Stridor YousefDocument7 pagesStridor YousefYousef Hassan BazarNo ratings yet
- Airway ObstructionDocument10 pagesAirway ObstructionyoantamaraNo ratings yet
- AiwaryManagement 1Document72 pagesAiwaryManagement 1Giselle EstoquiaNo ratings yet
- Acute Respiratory Distress in Children - Emergency Evaluation and Initial Stabilization - UpToDateDocument29 pagesAcute Respiratory Distress in Children - Emergency Evaluation and Initial Stabilization - UpToDateana salakaiaNo ratings yet
- Postoperative Nursing Care-1Document9 pagesPostoperative Nursing Care-1MegaaNo ratings yet
- Anesthesia NotesDocument25 pagesAnesthesia NotesReddyNo ratings yet
- Pediatrics StridorDocument13 pagesPediatrics StridorEmaNo ratings yet
- Lec.1 General Management of The Patient With Facial InjuriesDocument93 pagesLec.1 General Management of The Patient With Facial InjuriesTeebaNo ratings yet
- Pediatric Respiratory OverviewDocument4 pagesPediatric Respiratory OverviewPaul Saquido CapiliNo ratings yet
- Pachtinger2013 PDFDocument16 pagesPachtinger2013 PDFdpcamposhNo ratings yet
- Concious Sedation PedoDocument29 pagesConcious Sedation Pedodrkamesh100% (1)
- Emergency Assesment and ManagementDocument16 pagesEmergency Assesment and ManagementImas Adelia Al BurdahNo ratings yet
- ABCDE Assessment NoteDocument28 pagesABCDE Assessment NoteHawwa SaifaNo ratings yet
- Volume 1 CorrectedDocument145 pagesVolume 1 Corrected897829No ratings yet
- Proning Self Learning Package 2020 FinalDocument18 pagesProning Self Learning Package 2020 FinalUWIMANA Jean ClaudeNo ratings yet
- Initial Assessment: Yesi Hasneli N, SKP, MnsDocument11 pagesInitial Assessment: Yesi Hasneli N, SKP, MnsPPNI RohulNo ratings yet
- ATLS BasicsDocument6 pagesATLS Basicss129682No ratings yet
- Dzino's SurgeryDocument718 pagesDzino's SurgeryHuram SeremaniNo ratings yet
- Postoperative Nursing ManagementDocument12 pagesPostoperative Nursing ManagementAhmed AliNo ratings yet
- Untitled DocumentDocument12 pagesUntitled DocumentCris Juev Jonathan RecayoNo ratings yet
- Postoperative Care of Oral and Maxillofa PDFDocument10 pagesPostoperative Care of Oral and Maxillofa PDFMashood AhmedNo ratings yet
- RPS - BLS (Dr. Bindo)Document38 pagesRPS - BLS (Dr. Bindo)Krmilla KumillNo ratings yet
- Management of The Unconscious PatientDocument9 pagesManagement of The Unconscious PatientDaramola JuwonNo ratings yet
- Diagnosis and Treatment of Chronic CoughFrom EverandDiagnosis and Treatment of Chronic CoughSang Heon ChoNo ratings yet
- Essentials in Lung TransplantationFrom EverandEssentials in Lung TransplantationAllan R. GlanvilleNo ratings yet
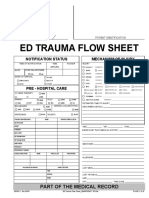
- Ed Trauma Flow Sheet: Part of The Medical RecordDocument6 pagesEd Trauma Flow Sheet: Part of The Medical RecordsafasayedNo ratings yet
- Assessment and Stabilization of The Trauma PatientDocument9 pagesAssessment and Stabilization of The Trauma PatientMohamed MansourNo ratings yet
- A Systematic Approach To EMS Cardiac Arrest Management Improves Survival For Out of Hospital Cardiac ArrestDocument29 pagesA Systematic Approach To EMS Cardiac Arrest Management Improves Survival For Out of Hospital Cardiac ArrestMELLYNDA ANASTASYANo ratings yet
- BLS2 ConferenceDocument39 pagesBLS2 Conferencekurt94764No ratings yet
- VENTILATOR MEKANIK DeswitaDocument25 pagesVENTILATOR MEKANIK DeswitaDinda AndrifaNo ratings yet
- Shock DR Sadia Hussain: Assistant Professor Pediatric Medicine King Edward Medical University LahoreDocument22 pagesShock DR Sadia Hussain: Assistant Professor Pediatric Medicine King Edward Medical University LahoreTouseef Ur RehmanNo ratings yet
- Mansilingan Agro Industrial High School Adult CPR: Assessor Say CaregiverDocument3 pagesMansilingan Agro Industrial High School Adult CPR: Assessor Say CaregiverSandeeNo ratings yet
- MODSDocument2 pagesMODSAa AaNo ratings yet
- (Notes) MEDICOLEGAL ASPECTS OF PHYSICAL INJURIESDocument20 pages(Notes) MEDICOLEGAL ASPECTS OF PHYSICAL INJURIESChristian Edward CoronadoNo ratings yet
- National Registry Skill SheetsDocument21 pagesNational Registry Skill SheetsKemzo AbarquezNo ratings yet
- Septic Shock: Dr. Dr. Hori Hariyanto, Span, Kic, KMNDocument89 pagesSeptic Shock: Dr. Dr. Hori Hariyanto, Span, Kic, KMNPander MadonNo ratings yet
- L12 Shock MCQ'sDocument4 pagesL12 Shock MCQ'srida hafeezNo ratings yet
- 1.3 CPR Training ReflectionDocument2 pages1.3 CPR Training ReflectionElliot SynderNo ratings yet
- International Association of Dental Traumatology Guidelines For The Management of Traumatic Dental Injuries - General IntroductionDocument5 pagesInternational Association of Dental Traumatology Guidelines For The Management of Traumatic Dental Injuries - General IntroductionAdil GhauriNo ratings yet
- Zachary Knable Resume 12-23 - No Contact InfoDocument1 pageZachary Knable Resume 12-23 - No Contact Infoapi-644926887No ratings yet
- Use of SALT Triage in A Simulated Mass-Casualty in PDFDocument7 pagesUse of SALT Triage in A Simulated Mass-Casualty in PDFGhani AbdurahimNo ratings yet
- Abg Practice QuizDocument13 pagesAbg Practice QuizPatty Romero0% (1)
- Besafe Sfat QuestionnaireDocument2 pagesBesafe Sfat QuestionnaireQueenie FloresNo ratings yet
- Full Download PDF of Emergency Care (EMT) 13th Edition by Daniel Limmer (Ebook PDF) All ChapterDocument43 pagesFull Download PDF of Emergency Care (EMT) 13th Edition by Daniel Limmer (Ebook PDF) All Chapterdieimewesenu100% (15)
- Penilaian Awal Pasien SyokDocument33 pagesPenilaian Awal Pasien SyokatikaNo ratings yet
- Pals Equip. ChecklistDocument6 pagesPals Equip. ChecklistbalaNo ratings yet
- BLS Provider ManualDocument23 pagesBLS Provider ManualMaya LaPrade100% (3)
- Bls Card 2023Document1 pageBls Card 2023api-719132260No ratings yet
- 011-HSE-L203E-03 Medical Emergency Response PlanDocument17 pages011-HSE-L203E-03 Medical Emergency Response PlanRizky SatriawanNo ratings yet
- Management of Chest Trauma: Corinna Ludwig, Aris KoryllosDocument6 pagesManagement of Chest Trauma: Corinna Ludwig, Aris KoryllosAnonymous G9gfz4No ratings yet
- Shock MTLSDocument31 pagesShock MTLSfasmelakaNo ratings yet
- Emergency RescueDocument24 pagesEmergency RescueSophia TalonNo ratings yet
- Endotracheal Intubation Flow SheetDocument2 pagesEndotracheal Intubation Flow SheetsafasayedNo ratings yet