Download as pdf or txt
You might also like
- Immunization With SARS Coronavirus Vaccines Leads To Pulmonary Immunopathology On Challenge With The SARS VirusDocument13 pagesImmunization With SARS Coronavirus Vaccines Leads To Pulmonary Immunopathology On Challenge With The SARS Virusadan_infowars88% (34)
- Cancer Immunotherapy: An Update: Abul K. Abbas Ucsf Abul - Abbas@ucsf - EduDocument26 pagesCancer Immunotherapy: An Update: Abul K. Abbas Ucsf Abul - Abbas@ucsf - EduHarits AmrullohNo ratings yet
- Altman 2017Document9 pagesAltman 2017Sílvia BastosNo ratings yet
- Fast-Tracked Swine Flu Vaccine Under FireDocument4 pagesFast-Tracked Swine Flu Vaccine Under FireaparnasingNo ratings yet
- Killey, Et Al. 2017 - Long-Lived Immunity To Canine Core Vaccine Antigens in UK Dogs As Assessed by An In-Practice Test KitDocument5 pagesKilley, Et Al. 2017 - Long-Lived Immunity To Canine Core Vaccine Antigens in UK Dogs As Assessed by An In-Practice Test KitFernandoNo ratings yet
- Summaries of Evidence in Support of Proposed Recommendations FinalDocument25 pagesSummaries of Evidence in Support of Proposed Recommendations FinalodyNo ratings yet
- Kennedy 2007Document8 pagesKennedy 2007Sílvia BastosNo ratings yet
- Immunity To Hep CDocument11 pagesImmunity To Hep CChelsey WilsonNo ratings yet
- Fase 3.1Document9 pagesFase 3.1Verliatesya TugasNo ratings yet
- Shedding of Infectious Sars-Cov-2 Despite Vaccination When The Delta Variant Is Prevalent - Wisconsin, July 2021Document9 pagesShedding of Infectious Sars-Cov-2 Despite Vaccination When The Delta Variant Is Prevalent - Wisconsin, July 2021Micheal NicolucciNo ratings yet
- Chappuis, Neonatal Immunity and Immunisation in Early Age. Lesons From Veterinary MedicineDocument5 pagesChappuis, Neonatal Immunity and Immunisation in Early Age. Lesons From Veterinary MedicineNath BixoNo ratings yet
- What Everyone Should Know About VaccinesDocument3 pagesWhat Everyone Should Know About VaccinesNicholay AtanassovNo ratings yet
- Epid 1Document4 pagesEpid 1lakshanNo ratings yet
- Researcharticle Open Access: Faust Et Al. BMC Pediatrics (2019) 19:50Document8 pagesResearcharticle Open Access: Faust Et Al. BMC Pediatrics (2019) 19:50Zahra Faras SukmaNo ratings yet
- Covid JournalDocument8 pagesCovid JournalwilverNo ratings yet
- A One-Time Screening of Newcastle Disease Hi Antibodies Before Slaughter As An Indicator of Vaccine Performance in Broiler ChickensDocument5 pagesA One-Time Screening of Newcastle Disease Hi Antibodies Before Slaughter As An Indicator of Vaccine Performance in Broiler ChickensLin DanNo ratings yet
- Jurnal 1Document9 pagesJurnal 1Riyan TrequartistaNo ratings yet
- Ac and VaccineDocument15 pagesAc and VaccineMayaLunaNo ratings yet
- Free Vaccine GuideDocument21 pagesFree Vaccine Guidesurveytryer2No ratings yet
- Vaccine: Parveen Fathima, Thomas L. Snelling, Robyn A. GibbsDocument6 pagesVaccine: Parveen Fathima, Thomas L. Snelling, Robyn A. GibbsAhmad Harissul IbadNo ratings yet
- Correlates of Protection Against Symptomatic and Asymptomatic Sars-Cov-2 InfectionDocument31 pagesCorrelates of Protection Against Symptomatic and Asymptomatic Sars-Cov-2 InfectionAbasyakira RaihanNo ratings yet
- Squires 2017Document10 pagesSquires 2017Emile CardNo ratings yet
- Distemper en PerrosDocument6 pagesDistemper en PerrosAlexandra GuerreroNo ratings yet
- Nejm VaricellaDocument9 pagesNejm VaricellaadityailhamNo ratings yet
- Extended Interval BNT162b2 Vaccination Enhances Peak Antibody Generation in Older PeopleDocument17 pagesExtended Interval BNT162b2 Vaccination Enhances Peak Antibody Generation in Older PeopleaphrodeNo ratings yet
- COVID 19 An Update For WSAVA Members February 17th 2021Document4 pagesCOVID 19 An Update For WSAVA Members February 17th 2021Lígia RochaNo ratings yet
- FMD Vaccine ImmunityDocument5 pagesFMD Vaccine ImmunityrogerNo ratings yet
- MainDocument20 pagesMainPedro FontaniveNo ratings yet
- Canine Parvovirus Current PerspectiveDocument15 pagesCanine Parvovirus Current PerspectivePrimyntNo ratings yet
- Polio VaccineDocument5 pagesPolio VaccineDyran25No ratings yet
- Varvo VaccinDocument11 pagesVarvo Vaccincatalin Cata16No ratings yet
- Feline Parvovirus Infection and Associated DiseasesDocument6 pagesFeline Parvovirus Infection and Associated Diseasesdandirection749No ratings yet
- Immune Responses To Measles and Mumps Vaccination of Infants at 6, 9, and 12 MonthsDocument10 pagesImmune Responses To Measles and Mumps Vaccination of Infants at 6, 9, and 12 MonthsManiru Aliyu GiganeNo ratings yet
- Schiller JT - 09Document6 pagesSchiller JT - 09Bruno RalhaNo ratings yet
- Varicella Vaccine Effectiveness Over 10 Years in Australia - 2019 - Journal ofDocument6 pagesVaricella Vaccine Effectiveness Over 10 Years in Australia - 2019 - Journal ofNihad MalikzadeNo ratings yet
- Safety and Immunogenicity of A Single Dose, Live-Attenuated Tetravalent Dengue Vaccine Feb 2022Document8 pagesSafety and Immunogenicity of A Single Dose, Live-Attenuated Tetravalent Dengue Vaccine Feb 2022Reinaldi octaNo ratings yet
- Towards An Epitope-Based Human Vaccine For Influenza: Tamar Ben-Yedidia Ruth ArnonDocument7 pagesTowards An Epitope-Based Human Vaccine For Influenza: Tamar Ben-Yedidia Ruth ArnonPCRMANNo ratings yet
- BVDV Term PaperDocument9 pagesBVDV Term Paperaef5190No ratings yet
- MR Bangladesh Jiw024 2016Document8 pagesMR Bangladesh Jiw024 2016RIRA MABRURATINo ratings yet
- Efficacy and Safety of A RecombinantDocument13 pagesEfficacy and Safety of A RecombinantSofyanNo ratings yet
- Articles: BackgroundDocument10 pagesArticles: Backgroundapi-102069217No ratings yet
- Immunogenicity of One-And Two-Dose Regimens of The Ad26.COV2.S COVID-19 Vaccine Candidate in Adult and Aged Rhesus MacaquesDocument36 pagesImmunogenicity of One-And Two-Dose Regimens of The Ad26.COV2.S COVID-19 Vaccine Candidate in Adult and Aged Rhesus MacaquesJared Michael BergerNo ratings yet
- Practical Aspects of Estimation ofDocument3 pagesPractical Aspects of Estimation ofMahjoubNo ratings yet
- Suitability of Individual and Bulk Milk Samples To Investigate The Humoral Immune Response To Lumpy Skin Disease Vaccination by ELISADocument7 pagesSuitability of Individual and Bulk Milk Samples To Investigate The Humoral Immune Response To Lumpy Skin Disease Vaccination by ELISAshital shermaleNo ratings yet
- Investigation of The Antiviral Effect of PDFDocument4 pagesInvestigation of The Antiviral Effect of PDFDita Adi PrasetyoNo ratings yet
- Canine Parvovirus Current Perspective PDFDocument15 pagesCanine Parvovirus Current Perspective PDFmalinasoareNo ratings yet
- Parvovirus Infection in DomesticDocument14 pagesParvovirus Infection in Domesticabhi.tangolliNo ratings yet
- Canine DistemperDocument18 pagesCanine DistemperJ Elver SilvaNo ratings yet
- 3 OTTO Biologicals - Notes (B PHarm III) - Fri 01st at 1800Hrs - (Swine-Fever Vac (Live, Prepared in Cell - Vet) - Oct 2021Document5 pages3 OTTO Biologicals - Notes (B PHarm III) - Fri 01st at 1800Hrs - (Swine-Fever Vac (Live, Prepared in Cell - Vet) - Oct 2021Bigabwa BernardNo ratings yet
- VaccineDocument7 pagesVaccineRong LiuNo ratings yet
- Article 1Document6 pagesArticle 1AMILA SYAZLINANo ratings yet
- 1-s2.0-S0167587719305884-mainDocument8 pages1-s2.0-S0167587719305884-mainwizzydoNo ratings yet
- Updateoncanineparvoviral Enteritis: Elisa M. MazzaferroDocument19 pagesUpdateoncanineparvoviral Enteritis: Elisa M. MazzaferroAlfian Yusak MuzakiNo ratings yet
- New Rabies Vaccines For Use in Humans: Hildegund C. J. ErtlDocument11 pagesNew Rabies Vaccines For Use in Humans: Hildegund C. J. Ertldewi najiraNo ratings yet
- Javma-Javma 2000 217 1021Document4 pagesJavma-Javma 2000 217 1021ara.lv007No ratings yet
- Long Term Persistence of Ige Anti-Influenza Virus Antibodies in Pediatric and Adult Serum Post Vaccination With Influenza Virus VaccineDocument6 pagesLong Term Persistence of Ige Anti-Influenza Virus Antibodies in Pediatric and Adult Serum Post Vaccination With Influenza Virus VaccineDesti EryaniNo ratings yet
- Midtlyng 2016Document23 pagesMidtlyng 2016Lê NgânNo ratings yet
- DECREASED BREADTH OF THE ANTIBODY RESPONSE TO THE SPIKE PROTEIN OF SARS-CoV-2 AFTER REPEATED VACCINATION - 2021.08.12.21261952v2.full PDFDocument27 pagesDECREASED BREADTH OF THE ANTIBODY RESPONSE TO THE SPIKE PROTEIN OF SARS-CoV-2 AFTER REPEATED VACCINATION - 2021.08.12.21261952v2.full PDFJohnNo ratings yet
- A. Brief Resume of Intended WorkDocument6 pagesA. Brief Resume of Intended WorkRabi DhakalNo ratings yet
- Mycobacteria BPTDocument26 pagesMycobacteria BPTbpt2No ratings yet
- Science 2007 Breakthrough of The Year Human Genetic VariationDocument2 pagesScience 2007 Breakthrough of The Year Human Genetic VariationCraig RaflaNo ratings yet
- Laboratory Test For Student Industrial WDocument54 pagesLaboratory Test For Student Industrial WCarol SoiNo ratings yet
- STS Finals RDocument8 pagesSTS Finals RFerlice JusayNo ratings yet
- Pest Management Science - 2019 - Lu - Transcriptomic Profiling of Effects of Emamectin Benzoate On The Pine Wood NematodeDocument11 pagesPest Management Science - 2019 - Lu - Transcriptomic Profiling of Effects of Emamectin Benzoate On The Pine Wood NematodeTomás Afonso CavacoNo ratings yet
- Doble Fase AcuosaDocument18 pagesDoble Fase AcuosaEdgar Ortiz AhumadaNo ratings yet
- IPC Vol1 Refernce Manual LaunchedDocument410 pagesIPC Vol1 Refernce Manual LaunchedAlwan YusufNo ratings yet
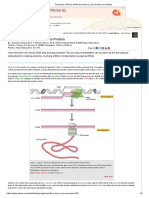
- Translation Dna To Mrna To ProteinDocument5 pagesTranslation Dna To Mrna To ProteinAna MarianaNo ratings yet
- Handout On Digestion, Respiration, Circulation and TransportDocument47 pagesHandout On Digestion, Respiration, Circulation and TransportNisha JodhanNo ratings yet
- Immunotherapy For Lung CancerDocument3 pagesImmunotherapy For Lung CancerPongwirat ChantasoontornNo ratings yet
- Biot 306 - 2017Document4 pagesBiot 306 - 2017shishir kafleNo ratings yet
- Cutril Top Eng 2021Document1 pageCutril Top Eng 2021Дмитрий СиленкоNo ratings yet
- Chromosomal AberrationsDocument15 pagesChromosomal AberrationsFuture TrekingNo ratings yet
- USMLE Vignette Flashcards: Micro, Path and Pharm - SidebysideDocument18 pagesUSMLE Vignette Flashcards: Micro, Path and Pharm - SidebysideMedSchoolStuffNo ratings yet
- Medicinal Study of Zingiberaceae PlantsDocument65 pagesMedicinal Study of Zingiberaceae PlantsPravin NagoreNo ratings yet
- Sip - BignayDocument11 pagesSip - BignayMarissa B DicionNo ratings yet
- IB Biology Hodder MindmapsDocument19 pagesIB Biology Hodder MindmapsFanny50% (2)
- Biotechnology Principles and Processes Revision Notes Cbse Class 12 BiologyDocument7 pagesBiotechnology Principles and Processes Revision Notes Cbse Class 12 Biologyak9268509No ratings yet
- The Intratumoral Bacterial Metataxonomic Signature of Hepatocellular CarcinomaDocument20 pagesThe Intratumoral Bacterial Metataxonomic Signature of Hepatocellular CarcinomaDenisNo ratings yet
- Biology 12 - The Cell - REVIEW WORKSHEET: Name: Block: DateDocument4 pagesBiology 12 - The Cell - REVIEW WORKSHEET: Name: Block: DateMarianne Kristine RayalaNo ratings yet
- Leucemia Limfatica CronicaDocument52 pagesLeucemia Limfatica CronicaAnghel BogdanNo ratings yet
- Coronavirus Simon Cowell: Fears For His SonDocument9 pagesCoronavirus Simon Cowell: Fears For His SonCazzac111No ratings yet
- Chapter 16 Homework Part IIDocument6 pagesChapter 16 Homework Part IIKvn4N6No ratings yet
- Targeting Receptor-Ligand Chemistry For Drug Delivery Across Blood-Brain Barrier in Brain DiseasesDocument15 pagesTargeting Receptor-Ligand Chemistry For Drug Delivery Across Blood-Brain Barrier in Brain DiseasesPrakash NargattiNo ratings yet
- First Detection of Bla TEM, SHV and CTX-M AmongDocument7 pagesFirst Detection of Bla TEM, SHV and CTX-M AmongHamidou OuedraogoNo ratings yet
- AST and Dosing Info Card - FINALDocument2 pagesAST and Dosing Info Card - FINALGAYATHIRINo ratings yet
- Artikel Paulien StokerDocument14 pagesArtikel Paulien StokerkikiNo ratings yet
- PFCRT Gene in Plasmodium Falciparum Field Isolates From Muzaffargarh, PakistanDocument12 pagesPFCRT Gene in Plasmodium Falciparum Field Isolates From Muzaffargarh, PakistanvivaNo ratings yet
- PDF Book UrduDocument4 pagesPDF Book UrduMuhammad KamranNo ratings yet