Download as pdf or txt
You might also like
- 4 Corners Gold Rush Lesson PlanDocument3 pages4 Corners Gold Rush Lesson Planapi-267003013No ratings yet
- Dietary Choline For The Lactating Cow. Possible Effects On Milk Fat Synthesis - Erdam, Shaver y VandersallDocument6 pagesDietary Choline For The Lactating Cow. Possible Effects On Milk Fat Synthesis - Erdam, Shaver y Vandersalljamonto5No ratings yet
- Supplementation of Infant Formula With Native InulinDocument6 pagesSupplementation of Infant Formula With Native InulinVictor SouzaNo ratings yet
- Anthropometrical Parameters and Markers of Obesity in RatsDocument9 pagesAnthropometrical Parameters and Markers of Obesity in RatsSammer BurgosNo ratings yet
- Atrovas Dan Feno FibrateDocument9 pagesAtrovas Dan Feno FibrateGalih Antona SinatriaNo ratings yet
- 1472 6882 2 1 PDFDocument7 pages1472 6882 2 1 PDFThiago NunesNo ratings yet
- Hadrová 2012Document11 pagesHadrová 2012leandro mendesNo ratings yet
- 1 s2.0 S002203021100213X MainDocument9 pages1 s2.0 S002203021100213X MainJuniClaudia13No ratings yet
- Short Communication The Absorption of Vitamin E Is Influenced by The Amount of Fat in A Meal and The Food MatrixDocument5 pagesShort Communication The Absorption of Vitamin E Is Influenced by The Amount of Fat in A Meal and The Food Matrixmrbin45No ratings yet
- Arabic GumDocument8 pagesArabic GumMohamed Essam ElraggalNo ratings yet
- 365 1370 1 PBDocument7 pages365 1370 1 PBYayang Ila YuliantiNo ratings yet
- Delgado Et Al 2009Document8 pagesDelgado Et Al 2009tcardosodelgadoNo ratings yet
- Potential Mechanisms of Improvement in Body Weight, Metabolic ProfileDocument8 pagesPotential Mechanisms of Improvement in Body Weight, Metabolic ProfileAG KhanNo ratings yet
- Main DocumantDocument14 pagesMain Documanthddcpf2cq4No ratings yet
- Effects of Pair-Feeding and Growth Hormone Treatment On Obese Transgenic RatsDocument5 pagesEffects of Pair-Feeding and Growth Hormone Treatment On Obese Transgenic RatsThanh LeNo ratings yet
- Mayuri PmsDocument27 pagesMayuri PmsnikuNo ratings yet
- HFD MiceDocument5 pagesHFD Micechar462No ratings yet
- Effect of Pleurotus Tuber-Regium Polysaccharides Supplementation On The Progression of Diabetes Complications in Obese-Diabetic RatsDocument11 pagesEffect of Pleurotus Tuber-Regium Polysaccharides Supplementation On The Progression of Diabetes Complications in Obese-Diabetic RatsAlmaNo ratings yet
- 1 s2.0 S2590286523000149 MainDocument12 pages1 s2.0 S2590286523000149 MainBunga JuliaNo ratings yet
- Quercetin KhasiatDocument6 pagesQuercetin KhasiatTantri AlfionitaNo ratings yet
- 2018 Effects of Pea With Barley and Less Processed Maize On Glycaemic Control in Diabetic Dogs Fabio TeixeiraDocument10 pages2018 Effects of Pea With Barley and Less Processed Maize On Glycaemic Control in Diabetic Dogs Fabio TeixeiramiriamvetNo ratings yet
- Metabolic Analysis of BALB/c Mice (Mus Musculus) Exposed in High Fat and Protein Diet Using Human Diagnostics Test KitsDocument16 pagesMetabolic Analysis of BALB/c Mice (Mus Musculus) Exposed in High Fat and Protein Diet Using Human Diagnostics Test KitsEmotholy LogicalNo ratings yet
- Dietary Protein Oscillation Effects On Feed IntakeDocument13 pagesDietary Protein Oscillation Effects On Feed IntakeParaschiva PîțuNo ratings yet
- Antidiabetic Effect of Fermented (Millet) Supplement in Alloxan Induced Hyperglycemic Wistar RatsDocument4 pagesAntidiabetic Effect of Fermented (Millet) Supplement in Alloxan Induced Hyperglycemic Wistar Ratsmaster apotNo ratings yet
- 1 s2.0 S0022030212002044 MainDocument19 pages1 s2.0 S0022030212002044 MainFriska YulandaNo ratings yet
- Nutrient Metabolism ClaDocument9 pagesNutrient Metabolism ClaEmanuel CotoNo ratings yet
- 10. Glycemic Index and Glycemic Load 8 Nov 2018-2Document41 pages10. Glycemic Index and Glycemic Load 8 Nov 2018-2Ichlasia Ainul FitriNo ratings yet
- Obesity - 2012 - Sampey - Cafeteria Diet Is A Robust Model of Human Metabolic Syndrome With Liver and Adipose InflammationDocument10 pagesObesity - 2012 - Sampey - Cafeteria Diet Is A Robust Model of Human Metabolic Syndrome With Liver and Adipose InflammationRodrigoNo ratings yet
- Fructans of Jerusalem ArtichokesDocument7 pagesFructans of Jerusalem ArtichokesAsmaa OtifyNo ratings yet
- Dietary Choline Supplementation On Growth PerformanceDocument8 pagesDietary Choline Supplementation On Growth PerformanceIsarosaeNo ratings yet
- Suplementação RPHistinaDocument14 pagesSuplementação RPHistinaleandro mendesNo ratings yet
- 1 s2.0 S0022030214005190 MainDocument11 pages1 s2.0 S0022030214005190 MainsiskaNo ratings yet
- Curcuma y MetforminaDocument8 pagesCurcuma y MetforminaJorge Luis Plasencia CubaNo ratings yet
- Effect of Transgalactooligosaccharides On The Composit - 1999 - The American JouDocument12 pagesEffect of Transgalactooligosaccharides On The Composit - 1999 - The American JouJoão PedroNo ratings yet
- Track 3 Eating Patterns and Behaviour P63Document15 pagesTrack 3 Eating Patterns and Behaviour P63Yuriko AndreNo ratings yet
- Response of C57Bl/6 Mice To A Carbohydrate-Free Diet: Research Open AccessDocument6 pagesResponse of C57Bl/6 Mice To A Carbohydrate-Free Diet: Research Open AccesspopopioNo ratings yet
- International Journal of Research in Biological Sciences: ISSN 2249 - 9687 Original ArticleDocument5 pagesInternational Journal of Research in Biological Sciences: ISSN 2249 - 9687 Original ArticleKannadhasan DassNo ratings yet
- Efecto Regulador de Griffola FrondosaDocument11 pagesEfecto Regulador de Griffola FrondosaPauly Campos OyarzúnNo ratings yet
- HAYVANDocument11 pagesHAYVANUgur DAĞDELENNo ratings yet
- Nutrients 12 01781Document13 pagesNutrients 12 01781Barbara DumasNo ratings yet
- Original ArticlesDocument8 pagesOriginal ArticlesVitalvet ClinicaveterianriaNo ratings yet
- ArticleDocument15 pagesArticlePokku ArifNo ratings yet
- Direct Evidence For The Presence of Human Milk Oligosaccharides in The Circulation of Breastfed InfantsDocument11 pagesDirect Evidence For The Presence of Human Milk Oligosaccharides in The Circulation of Breastfed InfantsHuan VuongNo ratings yet
- Untitled 1Document17 pagesUntitled 1bennyNo ratings yet
- 9 Estudio en Condiciones Reales de Lactantes Alimentados Con Una Fórmula InfantilDocument10 pages9 Estudio en Condiciones Reales de Lactantes Alimentados Con Una Fórmula InfantilLuisa CruzNo ratings yet
- 3 Ijmpsaug20183Document8 pages3 Ijmpsaug20183TJPRC PublicationsNo ratings yet
- Cacao 1Document5 pagesCacao 1Neri MargaretNo ratings yet
- Brestfeeding 1Document6 pagesBrestfeeding 1Muhamad Khusnu AbdurahmanNo ratings yet
- Effects of Maternal Level of Dietary Cation-Anion Difference Fed To Prepartum Nulliparous Cows On Offspring Acid-Base Balance, Metabolism, and GrowthDocument19 pagesEffects of Maternal Level of Dietary Cation-Anion Difference Fed To Prepartum Nulliparous Cows On Offspring Acid-Base Balance, Metabolism, and GrowthRoney ZimpelNo ratings yet
- Efficacy of Aqueous Leaf Extract of Vernonia Amygdalina On Plasma Lipoprotein and Oxidative Status in Diabetic Rat Models. H. U. NwanjoDocument4 pagesEfficacy of Aqueous Leaf Extract of Vernonia Amygdalina On Plasma Lipoprotein and Oxidative Status in Diabetic Rat Models. H. U. NwanjoNgan HoangNo ratings yet
- 10-Growth and Metabolism of Pacu Juveniles Fed Dietas WithDocument9 pages10-Growth and Metabolism of Pacu Juveniles Fed Dietas WithMarian MeloNo ratings yet
- Duodenal Endoluminal Barrier Sleeve Alters Gut Microbiota of ZDF RatsDocument28 pagesDuodenal Endoluminal Barrier Sleeve Alters Gut Microbiota of ZDF RatsIngrid MillanNo ratings yet
- 1 Ijapbcraug20171Document6 pages1 Ijapbcraug20171TJPRC PublicationsNo ratings yet
- Ginger PublishedDocument8 pagesGinger PublishedFatimoh AbdulsalamNo ratings yet
- Effect of Wakame On Non Alcoholic Fatty LiverDocument14 pagesEffect of Wakame On Non Alcoholic Fatty LiverCătălina RădulescuNo ratings yet
- Long-Term Intake of Milk Peptides Attenuates Development of Hypertension in Spontaneously Hypertensive RatsDocument10 pagesLong-Term Intake of Milk Peptides Attenuates Development of Hypertension in Spontaneously Hypertensive RatsRecky PatalaNo ratings yet
- Veterinary SciencesDocument16 pagesVeterinary SciencesaryonoNo ratings yet
- Study On The Extension of Shelf-Life by Activation of Inherent Lactoperoxidase System in Raw Cow MilkDocument4 pagesStudy On The Extension of Shelf-Life by Activation of Inherent Lactoperoxidase System in Raw Cow MilkSushil KoiralaNo ratings yet
- J. Dairy Sci. 102:1144-1159: M. Focant, E. Froidmont, Q. Archambeau, Q. C. Dang Van, and Y. LarondelleDocument16 pagesJ. Dairy Sci. 102:1144-1159: M. Focant, E. Froidmont, Q. Archambeau, Q. C. Dang Van, and Y. LarondelleMohammad BurhanudinNo ratings yet
- Influence of Feed Intake On Blood Chemistry Parameters in Kacang GoatsDocument4 pagesInfluence of Feed Intake On Blood Chemistry Parameters in Kacang GoatsHazim Azmi Al-QadryNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 10: ObstetricsFrom EverandComplementary and Alternative Medical Lab Testing Part 10: ObstetricsNo ratings yet
- MASB7 Construction Contract7Document3 pagesMASB7 Construction Contract7hyraldNo ratings yet
- Wagner and Traud ArticleDocument13 pagesWagner and Traud Articlegrimaguil100% (1)
- PSP Assignment1Document25 pagesPSP Assignment1B BasitNo ratings yet
- Beyond FurosemideDocument13 pagesBeyond FurosemideHeath HensleyNo ratings yet
- Covalence S1301-M Epoxy Primer: DescriptionDocument4 pagesCovalence S1301-M Epoxy Primer: DescriptionJuan Carlos Contreras CherresNo ratings yet
- CHINT Installation Operation Manual For Inverter of 50-60KTLDocument98 pagesCHINT Installation Operation Manual For Inverter of 50-60KTLr.pimentel.souzaNo ratings yet
- Autoconceito ShavelsonDocument15 pagesAutoconceito ShavelsonJuliana SchwarzNo ratings yet
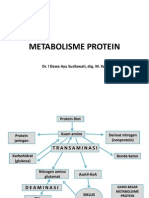
- Metabolisme Protein: Dr. I Dewa Ayu Susilawati, Drg. M. KesDocument31 pagesMetabolisme Protein: Dr. I Dewa Ayu Susilawati, Drg. M. KesMelisa Novitasari100% (2)
- Nine Day Novena of The Holy Face of JesusDocument25 pagesNine Day Novena of The Holy Face of Jesusangutoko benard100% (2)
- Planning and Facilities: Building StorageDocument31 pagesPlanning and Facilities: Building Storagequsai migdadiNo ratings yet
- DPP 02 NTSE BY @class - 10 - MaterialsDocument1 pageDPP 02 NTSE BY @class - 10 - MaterialsShashwat MishraNo ratings yet
- Cp1018 Boric Acid MsdsDocument6 pagesCp1018 Boric Acid MsdsPanneer SelvamNo ratings yet
- Surface Anatomy Lungs Group 2bDocument8 pagesSurface Anatomy Lungs Group 2bapi-323356666No ratings yet
- Heterocyclic Aromatic CompoundsDocument67 pagesHeterocyclic Aromatic CompoundsTuyenHHC100% (1)
- Manual Spray GunDocument6 pagesManual Spray GunSyazwan KhairulNo ratings yet
- Screenshot 2021-12-18 at 2.26.56 PMDocument1 pageScreenshot 2021-12-18 at 2.26.56 PMTanya NguyenNo ratings yet
- Ethics in HRMDocument7 pagesEthics in HRMVinay RamaneNo ratings yet
- What Can Science Tell Us About DeathDocument5 pagesWhat Can Science Tell Us About DeathGG7M1 gervacioNo ratings yet
- Materials Chemistry A: Journal ofDocument7 pagesMaterials Chemistry A: Journal ofFamiloni LayoNo ratings yet
- Expense 12-18 Agustus 2022Document4 pagesExpense 12-18 Agustus 2022Rizal RisqiNo ratings yet
- Rice Sector PACRA - 1604759631Document29 pagesRice Sector PACRA - 1604759631Huzefa SarayiNo ratings yet
- IFU Acticor 439128-F EsDocument143 pagesIFU Acticor 439128-F EsMartin ArrietaNo ratings yet
- Call History 640273efa1d48Document2 pagesCall History 640273efa1d48Krishnapriya GovindNo ratings yet
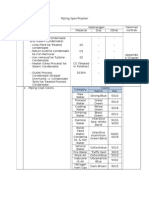
- Piping SpecificationDocument5 pagesPiping SpecificationShandi Hasnul FarizalNo ratings yet
- Feasibility of Screening For Preschool Behavioral and Emotional Problems in Primary Care Using The Early Childhood Screening AssessmentDocument9 pagesFeasibility of Screening For Preschool Behavioral and Emotional Problems in Primary Care Using The Early Childhood Screening AssessmentAhmed RamzyNo ratings yet
- Vespa S 125 3V Ie 150 3V Ie UPUTSTVODocument90 pagesVespa S 125 3V Ie 150 3V Ie UPUTSTVOdoughstoneNo ratings yet
- Mbarang 10102022Document3 pagesMbarang 10102022zeta chenkNo ratings yet
- A Country Boy Quits SchoolDocument4 pagesA Country Boy Quits SchoolJamaica Bianca Baynosa AnguloNo ratings yet
- Over The Counter MedicinesDocument3 pagesOver The Counter MedicinesJhun Echipare100% (3)