
Using Relaxation and Guided Imagery to Address Pain, Fatigue, and Sleep Disturbances: A Pilot Study
Using Relaxation and Guided Imagery to Address Pain, Fatigue, and Sleep Disturbances: A Pilot Study
You might also like
- Adriaan Louw - Pain Neuroscience Education - Teaching People About Pain - Libgen - LiDocument538 pagesAdriaan Louw - Pain Neuroscience Education - Teaching People About Pain - Libgen - LielfisiooficialNo ratings yet
- AI in SurgeryDocument12 pagesAI in Surgerylakshminivas PingaliNo ratings yet
- Driveline Youth Arm Care ProgramDocument28 pagesDriveline Youth Arm Care Programervo100% (1)
- This Is The Complete Set of PDF Study Guides 2023Document4,356 pagesThis Is The Complete Set of PDF Study Guides 2023learn exams50% (2)
- Nursing Care Plan - Myocardial InfarctionDocument3 pagesNursing Care Plan - Myocardial Infarctionderic80% (10)
- FUNDA ExamDocument6 pagesFUNDA ExamteabagmanNo ratings yet
- FBLA Winners 2015Document20 pagesFBLA Winners 2015Brandon TruongNo ratings yet
- ICU Liberation PosterDocument1 pageICU Liberation PosterhelenaNo ratings yet
- The Effects of The CORE Programme On Pain at Rest, Movement-Induced and Secondary Pain, Active Range of Motion, and Proprioception in Female Office Workers With Chronic Low Back Pa..Document11 pagesThe Effects of The CORE Programme On Pain at Rest, Movement-Induced and Secondary Pain, Active Range of Motion, and Proprioception in Female Office Workers With Chronic Low Back Pa..ilhamNo ratings yet
- Individual Difference Variables and The Effects of Progressive Muscle Relaxation and Analgesic Imagery Interventions On Cancer PainDocument12 pagesIndividual Difference Variables and The Effects of Progressive Muscle Relaxation and Analgesic Imagery Interventions On Cancer PainUswatun HasanahNo ratings yet
- 016unit 3 - Concepts and Challenges in Patient ManagementDocument3 pages016unit 3 - Concepts and Challenges in Patient ManagementSweet HeartNo ratings yet
- Jurnal Relaxation 1Document14 pagesJurnal Relaxation 1muhamad ridzwanNo ratings yet
- CPH 2ND WK NCPDocument5 pagesCPH 2ND WK NCPAyessa Camelle DumileNo ratings yet
- Seven Key Themes in Physical Therapy Advice For Patients Living With Subacromial Shoulder Pain: A Scoping ReviewDocument21 pagesSeven Key Themes in Physical Therapy Advice For Patients Living With Subacromial Shoulder Pain: A Scoping ReviewJacinta SeguraNo ratings yet
- Potts Disease NCP .. JustificationDocument8 pagesPotts Disease NCP .. JustificationMicah SalesNo ratings yet
- Mueller Et Al 2023 Resistance Motor Control and Mindfulness Based Exercises Are Effective For Treating ChronicDocument40 pagesMueller Et Al 2023 Resistance Motor Control and Mindfulness Based Exercises Are Effective For Treating ChronicNiko TrogerNo ratings yet
- Dolor de CuelloDocument9 pagesDolor de CuelloKaren BurgosNo ratings yet
- NCP FormDocument5 pagesNCP FormErika Bea PaculanangNo ratings yet
- Albornoz Cabello2019Document10 pagesAlbornoz Cabello2019Wen-Yu ShinNo ratings yet
- London Final Ch42Document26 pagesLondon Final Ch42kafosidNo ratings yet
- NCPDocument3 pagesNCPShei LaNo ratings yet
- Progressive Muscle RelaxationDhandapanietalDocument13 pagesProgressive Muscle RelaxationDhandapanietalS.N HanifahNo ratings yet
- Demonstrate: Pain Coping TechniquesDocument4 pagesDemonstrate: Pain Coping TechniquesMae Therese B. MAGNO100% (1)
- Impaired MobilityDocument3 pagesImpaired MobilityAbegail QuintoNo ratings yet
- Planning Assessment Diagnosis Implementation Rationale EvaluationDocument1 pagePlanning Assessment Diagnosis Implementation Rationale Evaluationagathajade23No ratings yet
- Assessment Nursing Diagnosis Analysis Planning Implementation Rationale EvaluationDocument1 pageAssessment Nursing Diagnosis Analysis Planning Implementation Rationale EvaluationAnne Beatriz SantiagoNo ratings yet
- 3 NCP FinalDocument7 pages3 NCP FinalJames PanlaanNo ratings yet
- NCP - Disturbed Sleep PatternDocument3 pagesNCP - Disturbed Sleep PatternKyla CalzadoNo ratings yet
- Effects of Adding A Neurodynamic Mobilization To.5Document9 pagesEffects of Adding A Neurodynamic Mobilization To.5Ana SoaresNo ratings yet
- Cho 2017. Bee venom acupuncture as and adjunctive treatment for Parkinsons diseaseDocument8 pagesCho 2017. Bee venom acupuncture as and adjunctive treatment for Parkinsons diseaseFabiola TrujilloNo ratings yet
- D3kepma2a - Reza Fani Bachtiar - P17210181018Document17 pagesD3kepma2a - Reza Fani Bachtiar - P17210181018mufid dodyNo ratings yet
- Complementary Therapies in Clinical PracticeDocument17 pagesComplementary Therapies in Clinical Practicemufid dodyNo ratings yet
- Complementary Therapies in Clinical PracticeDocument17 pagesComplementary Therapies in Clinical Practicemufid dodyNo ratings yet
- The Impact of A Cognitive Behavioral Pain Management Program On Sleep in Patients With Chronic Pain Results of A Pilot StudyDocument10 pagesThe Impact of A Cognitive Behavioral Pain Management Program On Sleep in Patients With Chronic Pain Results of A Pilot StudyMário Márcio da Matta LopesNo ratings yet
- Nursing Care Plan: Subjective Cues: Goal/objectiveDocument2 pagesNursing Care Plan: Subjective Cues: Goal/objectiveNikka PelayoNo ratings yet
- NCPDocument2 pagesNCPKaren Joyce Costales MagtanongNo ratings yet
- Reliability, Standard Error, and Minimum Detectable Change of Clinical Pressure Pain Threshold Testing in People With and Without Acute Neck PainDocument7 pagesReliability, Standard Error, and Minimum Detectable Change of Clinical Pressure Pain Threshold Testing in People With and Without Acute Neck PaindoctorhealthNo ratings yet
- NCP-Septic Shock (Acute Pain)Document3 pagesNCP-Septic Shock (Acute Pain)Ted anadiloNo ratings yet
- AnestesiDocument16 pagesAnestesiKanesti KamajayaNo ratings yet
- Chen Bi1997Document15 pagesChen Bi1997Psikiatri 76 UndipNo ratings yet
- Nursing Care Plan: Nikolai P. Funcion, FSUU-SNDocument5 pagesNursing Care Plan: Nikolai P. Funcion, FSUU-SNNikolai FuncionNo ratings yet
- Acute Pain Related To Effects of Labor and Delivery ProcessDocument3 pagesAcute Pain Related To Effects of Labor and Delivery ProcessrlinaoNo ratings yet
- Nursing Care PlanDocument5 pagesNursing Care PlanLaceth Joyce T. LASATNo ratings yet
- Appendicitis NCPDocument5 pagesAppendicitis NCPEarl Joseph DezaNo ratings yet
- Appendicitis - NCPDocument5 pagesAppendicitis - NCPEarl Joseph Deza100% (1)
- Neuropathic Pain - Diagnosis & ScreeningDocument15 pagesNeuropathic Pain - Diagnosis & ScreeningdrsantoshkalelearningNo ratings yet
- Architecture Portfolio SilmaDocument30 pagesArchitecture Portfolio Silmasilma subahNo ratings yet
- Lucion, Alyza NCPDocument22 pagesLucion, Alyza NCPAlyza LucionNo ratings yet
- Sheng 2019Document7 pagesSheng 2019carlossilva.ssaNo ratings yet
- NCP NephrolithiasisDocument3 pagesNCP NephrolithiasisMANUEL EMERSONNo ratings yet
- Think Before You Administer: Is Routine Benzodiazepine Premedication Before Endoscopy in Adults Necessary?Document3 pagesThink Before You Administer: Is Routine Benzodiazepine Premedication Before Endoscopy in Adults Necessary?Irak TorresNo ratings yet
- Keaslian Penelitian: No. Judul Karya Ilmiah & Penulis Variabel Jenis Penelitian HasilDocument2 pagesKeaslian Penelitian: No. Judul Karya Ilmiah & Penulis Variabel Jenis Penelitian HasilAkhmad Miftahul HudaNo ratings yet
- Interscalene Brachial Plexus Block With Liposomal Bupivacaine Bupivacaine With Perineural Dexamethasone: A Noninferiority TrialDocument14 pagesInterscalene Brachial Plexus Block With Liposomal Bupivacaine Bupivacaine With Perineural Dexamethasone: A Noninferiority TrialCoco ValdanyNo ratings yet
- Effectiveness of Acupuncture For Pain Control After Cesarean Delivery A Randomized Clinical TrialDocument13 pagesEffectiveness of Acupuncture For Pain Control After Cesarean Delivery A Randomized Clinical TrialgigicarvajalNo ratings yet
- M Allows 2017Document3 pagesM Allows 2017Francisco Javier Luza RamosNo ratings yet
- Proprioceptive Neuromuscular Facilitation: Vicky S. WardlawDocument44 pagesProprioceptive Neuromuscular Facilitation: Vicky S. WardlawPraneetha Nouduri100% (1)
- Coury CoopexpoDocument1 pageCoury Coopexpoapi-368156205No ratings yet
- NCP Form 2Document2 pagesNCP Form 2Kate Aenyle AgsoyNo ratings yet
- Nursing Action PlanDocument4 pagesNursing Action PlanScribdTranslationsNo ratings yet
- Langmore Pisegna 2015 Efficacy PDFDocument8 pagesLangmore Pisegna 2015 Efficacy PDFvanyNo ratings yet
- Sedacion Paliativa Al Final de La VidaDocument9 pagesSedacion Paliativa Al Final de La VidaYesica Villalba CerqueraNo ratings yet
- Atlas of Botulinum Toxin Injection: Dosage | Localization | ApplicationFrom EverandAtlas of Botulinum Toxin Injection: Dosage | Localization | ApplicationNo ratings yet
- Craniosacral Therapy: A Beginner's Guide and Overview on Its Use Cases, with an FAQFrom EverandCraniosacral Therapy: A Beginner's Guide and Overview on Its Use Cases, with an FAQNo ratings yet
- EMI Therapy: clinical cases treated and commented step by step (English Edition)From EverandEMI Therapy: clinical cases treated and commented step by step (English Edition)No ratings yet
- Confidential Psychological Evaluation - ExampleDocument3 pagesConfidential Psychological Evaluation - Exampledan8souzaNo ratings yet
- Current Ams GssDocument2 pagesCurrent Ams GssLittle MermaidNo ratings yet
- Person Centred Healthcare-Rolfe's Reflective Model What?Document2 pagesPerson Centred Healthcare-Rolfe's Reflective Model What?api-637456941No ratings yet
- Midterm Exam McaDocument7 pagesMidterm Exam McaBeverly DatuNo ratings yet
- DisasterDocument16 pagesDisasterEricsonMitraNo ratings yet
- Uttarakhand Ayush POLICY 2018Document31 pagesUttarakhand Ayush POLICY 2018Vishy BhatiaNo ratings yet
- Lavell Lane Civil ComplaintDocument12 pagesLavell Lane Civil ComplaintUSA TODAY NetworkNo ratings yet
- Knowledge, Attitude and Practicesamongprimary Care Workers On Infection, Prevention and Control Amidst The Covid-19 PandemicDocument25 pagesKnowledge, Attitude and Practicesamongprimary Care Workers On Infection, Prevention and Control Amidst The Covid-19 PandemicIJAR JOURNALNo ratings yet
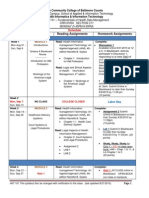
- ScheduleDocument7 pagesScheduleapi-296878004No ratings yet
- The New Global Map of Human BrucellosisDocument9 pagesThe New Global Map of Human BrucellosisNouman Safdar AliNo ratings yet
- Sarcoma NCPDocument8 pagesSarcoma NCPginosanNo ratings yet
- Homeopathic Medicine & Pharmacy 1543Document173 pagesHomeopathic Medicine & Pharmacy 1543maxisinc.inNo ratings yet
- Prospectus 2022 MD MSDocument8 pagesProspectus 2022 MD MSarun vNo ratings yet
- Emergency Medicine Dissertation TopicsDocument8 pagesEmergency Medicine Dissertation TopicsBuyCollegePaperSingapore100% (1)
- Advancing Palliative Care in The Public Sector - DrRichardLimDocument26 pagesAdvancing Palliative Care in The Public Sector - DrRichardLimmalaysianhospicecouncil6240100% (1)
- Herbal Drug Interactions A Major Safety ConcernDocument5 pagesHerbal Drug Interactions A Major Safety ConcernSuciPutriRahmawaniNo ratings yet
- Total Gallium JB15939XXDocument18 pagesTotal Gallium JB15939XXAsim AliNo ratings yet
- Student Evaluation Tool-Hail UniversityDocument6 pagesStudent Evaluation Tool-Hail UniversityRichard Balacuit MaestradoNo ratings yet
- Age-Related Differences in Hospitalization Rates, Clinical Presentation, and Outcomes Among Older Adults Hospitalized With Influenza-U.S. Influenza Hospitalization Surveillance NetworkDocument8 pagesAge-Related Differences in Hospitalization Rates, Clinical Presentation, and Outcomes Among Older Adults Hospitalized With Influenza-U.S. Influenza Hospitalization Surveillance NetworkTony RobertsNo ratings yet
- Hospital Literature StudyDocument30 pagesHospital Literature StudyIsaac Jeb80% (10)
- Adls Final Research PosterDocument1 pageAdls Final Research Posterapi-453651228No ratings yet
- Nursing AuditDocument3 pagesNursing AuditJoe Shewale0% (1)
- Rewarding Healthcare Executives in A Dispersed Yet Integrated FirmDocument40 pagesRewarding Healthcare Executives in A Dispersed Yet Integrated FirmDragana AvramovskaNo ratings yet
- Acog Practice Bullet In: Tubal Ectopic PregnancyDocument13 pagesAcog Practice Bullet In: Tubal Ectopic PregnancydlucNo ratings yet
- 8 - Anesthesia and Patient SafetyDocument16 pages8 - Anesthesia and Patient SafetyMilazar NigelNo ratings yet





















































































Download as pdf or txt
You might also like
- Adriaan Louw - Pain Neuroscience Education - Teaching People About Pain - Libgen - LiDocument538 pagesAdriaan Louw - Pain Neuroscience Education - Teaching People About Pain - Libgen - LielfisiooficialNo ratings yet
- AI in SurgeryDocument12 pagesAI in Surgerylakshminivas PingaliNo ratings yet
- Driveline Youth Arm Care ProgramDocument28 pagesDriveline Youth Arm Care Programervo100% (1)
- This Is The Complete Set of PDF Study Guides 2023Document4,356 pagesThis Is The Complete Set of PDF Study Guides 2023learn exams50% (2)
- Nursing Care Plan - Myocardial InfarctionDocument3 pagesNursing Care Plan - Myocardial Infarctionderic80% (10)
- FUNDA ExamDocument6 pagesFUNDA ExamteabagmanNo ratings yet
- FBLA Winners 2015Document20 pagesFBLA Winners 2015Brandon TruongNo ratings yet
- ICU Liberation PosterDocument1 pageICU Liberation PosterhelenaNo ratings yet
- The Effects of The CORE Programme On Pain at Rest, Movement-Induced and Secondary Pain, Active Range of Motion, and Proprioception in Female Office Workers With Chronic Low Back Pa..Document11 pagesThe Effects of The CORE Programme On Pain at Rest, Movement-Induced and Secondary Pain, Active Range of Motion, and Proprioception in Female Office Workers With Chronic Low Back Pa..ilhamNo ratings yet
- Individual Difference Variables and The Effects of Progressive Muscle Relaxation and Analgesic Imagery Interventions On Cancer PainDocument12 pagesIndividual Difference Variables and The Effects of Progressive Muscle Relaxation and Analgesic Imagery Interventions On Cancer PainUswatun HasanahNo ratings yet
- 016unit 3 - Concepts and Challenges in Patient ManagementDocument3 pages016unit 3 - Concepts and Challenges in Patient ManagementSweet HeartNo ratings yet
- Jurnal Relaxation 1Document14 pagesJurnal Relaxation 1muhamad ridzwanNo ratings yet
- CPH 2ND WK NCPDocument5 pagesCPH 2ND WK NCPAyessa Camelle DumileNo ratings yet
- Seven Key Themes in Physical Therapy Advice For Patients Living With Subacromial Shoulder Pain: A Scoping ReviewDocument21 pagesSeven Key Themes in Physical Therapy Advice For Patients Living With Subacromial Shoulder Pain: A Scoping ReviewJacinta SeguraNo ratings yet
- Potts Disease NCP .. JustificationDocument8 pagesPotts Disease NCP .. JustificationMicah SalesNo ratings yet
- Mueller Et Al 2023 Resistance Motor Control and Mindfulness Based Exercises Are Effective For Treating ChronicDocument40 pagesMueller Et Al 2023 Resistance Motor Control and Mindfulness Based Exercises Are Effective For Treating ChronicNiko TrogerNo ratings yet
- Dolor de CuelloDocument9 pagesDolor de CuelloKaren BurgosNo ratings yet
- NCP FormDocument5 pagesNCP FormErika Bea PaculanangNo ratings yet
- Albornoz Cabello2019Document10 pagesAlbornoz Cabello2019Wen-Yu ShinNo ratings yet
- London Final Ch42Document26 pagesLondon Final Ch42kafosidNo ratings yet
- NCPDocument3 pagesNCPShei LaNo ratings yet
- Progressive Muscle RelaxationDhandapanietalDocument13 pagesProgressive Muscle RelaxationDhandapanietalS.N HanifahNo ratings yet
- Demonstrate: Pain Coping TechniquesDocument4 pagesDemonstrate: Pain Coping TechniquesMae Therese B. MAGNO100% (1)
- Impaired MobilityDocument3 pagesImpaired MobilityAbegail QuintoNo ratings yet
- Planning Assessment Diagnosis Implementation Rationale EvaluationDocument1 pagePlanning Assessment Diagnosis Implementation Rationale Evaluationagathajade23No ratings yet
- Assessment Nursing Diagnosis Analysis Planning Implementation Rationale EvaluationDocument1 pageAssessment Nursing Diagnosis Analysis Planning Implementation Rationale EvaluationAnne Beatriz SantiagoNo ratings yet
- 3 NCP FinalDocument7 pages3 NCP FinalJames PanlaanNo ratings yet
- NCP - Disturbed Sleep PatternDocument3 pagesNCP - Disturbed Sleep PatternKyla CalzadoNo ratings yet
- Effects of Adding A Neurodynamic Mobilization To.5Document9 pagesEffects of Adding A Neurodynamic Mobilization To.5Ana SoaresNo ratings yet
- Cho 2017. Bee venom acupuncture as and adjunctive treatment for Parkinsons diseaseDocument8 pagesCho 2017. Bee venom acupuncture as and adjunctive treatment for Parkinsons diseaseFabiola TrujilloNo ratings yet
- D3kepma2a - Reza Fani Bachtiar - P17210181018Document17 pagesD3kepma2a - Reza Fani Bachtiar - P17210181018mufid dodyNo ratings yet
- Complementary Therapies in Clinical PracticeDocument17 pagesComplementary Therapies in Clinical Practicemufid dodyNo ratings yet
- Complementary Therapies in Clinical PracticeDocument17 pagesComplementary Therapies in Clinical Practicemufid dodyNo ratings yet
- The Impact of A Cognitive Behavioral Pain Management Program On Sleep in Patients With Chronic Pain Results of A Pilot StudyDocument10 pagesThe Impact of A Cognitive Behavioral Pain Management Program On Sleep in Patients With Chronic Pain Results of A Pilot StudyMário Márcio da Matta LopesNo ratings yet
- Nursing Care Plan: Subjective Cues: Goal/objectiveDocument2 pagesNursing Care Plan: Subjective Cues: Goal/objectiveNikka PelayoNo ratings yet
- NCPDocument2 pagesNCPKaren Joyce Costales MagtanongNo ratings yet
- Reliability, Standard Error, and Minimum Detectable Change of Clinical Pressure Pain Threshold Testing in People With and Without Acute Neck PainDocument7 pagesReliability, Standard Error, and Minimum Detectable Change of Clinical Pressure Pain Threshold Testing in People With and Without Acute Neck PaindoctorhealthNo ratings yet
- NCP-Septic Shock (Acute Pain)Document3 pagesNCP-Septic Shock (Acute Pain)Ted anadiloNo ratings yet
- AnestesiDocument16 pagesAnestesiKanesti KamajayaNo ratings yet
- Chen Bi1997Document15 pagesChen Bi1997Psikiatri 76 UndipNo ratings yet
- Nursing Care Plan: Nikolai P. Funcion, FSUU-SNDocument5 pagesNursing Care Plan: Nikolai P. Funcion, FSUU-SNNikolai FuncionNo ratings yet
- Acute Pain Related To Effects of Labor and Delivery ProcessDocument3 pagesAcute Pain Related To Effects of Labor and Delivery ProcessrlinaoNo ratings yet
- Nursing Care PlanDocument5 pagesNursing Care PlanLaceth Joyce T. LASATNo ratings yet
- Appendicitis NCPDocument5 pagesAppendicitis NCPEarl Joseph DezaNo ratings yet
- Appendicitis - NCPDocument5 pagesAppendicitis - NCPEarl Joseph Deza100% (1)
- Neuropathic Pain - Diagnosis & ScreeningDocument15 pagesNeuropathic Pain - Diagnosis & ScreeningdrsantoshkalelearningNo ratings yet
- Architecture Portfolio SilmaDocument30 pagesArchitecture Portfolio Silmasilma subahNo ratings yet
- Lucion, Alyza NCPDocument22 pagesLucion, Alyza NCPAlyza LucionNo ratings yet
- Sheng 2019Document7 pagesSheng 2019carlossilva.ssaNo ratings yet
- NCP NephrolithiasisDocument3 pagesNCP NephrolithiasisMANUEL EMERSONNo ratings yet
- Think Before You Administer: Is Routine Benzodiazepine Premedication Before Endoscopy in Adults Necessary?Document3 pagesThink Before You Administer: Is Routine Benzodiazepine Premedication Before Endoscopy in Adults Necessary?Irak TorresNo ratings yet
- Keaslian Penelitian: No. Judul Karya Ilmiah & Penulis Variabel Jenis Penelitian HasilDocument2 pagesKeaslian Penelitian: No. Judul Karya Ilmiah & Penulis Variabel Jenis Penelitian HasilAkhmad Miftahul HudaNo ratings yet
- Interscalene Brachial Plexus Block With Liposomal Bupivacaine Bupivacaine With Perineural Dexamethasone: A Noninferiority TrialDocument14 pagesInterscalene Brachial Plexus Block With Liposomal Bupivacaine Bupivacaine With Perineural Dexamethasone: A Noninferiority TrialCoco ValdanyNo ratings yet
- Effectiveness of Acupuncture For Pain Control After Cesarean Delivery A Randomized Clinical TrialDocument13 pagesEffectiveness of Acupuncture For Pain Control After Cesarean Delivery A Randomized Clinical TrialgigicarvajalNo ratings yet
- M Allows 2017Document3 pagesM Allows 2017Francisco Javier Luza RamosNo ratings yet
- Proprioceptive Neuromuscular Facilitation: Vicky S. WardlawDocument44 pagesProprioceptive Neuromuscular Facilitation: Vicky S. WardlawPraneetha Nouduri100% (1)
- Coury CoopexpoDocument1 pageCoury Coopexpoapi-368156205No ratings yet
- NCP Form 2Document2 pagesNCP Form 2Kate Aenyle AgsoyNo ratings yet
- Nursing Action PlanDocument4 pagesNursing Action PlanScribdTranslationsNo ratings yet
- Langmore Pisegna 2015 Efficacy PDFDocument8 pagesLangmore Pisegna 2015 Efficacy PDFvanyNo ratings yet
- Sedacion Paliativa Al Final de La VidaDocument9 pagesSedacion Paliativa Al Final de La VidaYesica Villalba CerqueraNo ratings yet
- Atlas of Botulinum Toxin Injection: Dosage | Localization | ApplicationFrom EverandAtlas of Botulinum Toxin Injection: Dosage | Localization | ApplicationNo ratings yet
- Craniosacral Therapy: A Beginner's Guide and Overview on Its Use Cases, with an FAQFrom EverandCraniosacral Therapy: A Beginner's Guide and Overview on Its Use Cases, with an FAQNo ratings yet
- EMI Therapy: clinical cases treated and commented step by step (English Edition)From EverandEMI Therapy: clinical cases treated and commented step by step (English Edition)No ratings yet
- Confidential Psychological Evaluation - ExampleDocument3 pagesConfidential Psychological Evaluation - Exampledan8souzaNo ratings yet
- Current Ams GssDocument2 pagesCurrent Ams GssLittle MermaidNo ratings yet
- Person Centred Healthcare-Rolfe's Reflective Model What?Document2 pagesPerson Centred Healthcare-Rolfe's Reflective Model What?api-637456941No ratings yet
- Midterm Exam McaDocument7 pagesMidterm Exam McaBeverly DatuNo ratings yet
- DisasterDocument16 pagesDisasterEricsonMitraNo ratings yet
- Uttarakhand Ayush POLICY 2018Document31 pagesUttarakhand Ayush POLICY 2018Vishy BhatiaNo ratings yet
- Lavell Lane Civil ComplaintDocument12 pagesLavell Lane Civil ComplaintUSA TODAY NetworkNo ratings yet
- Knowledge, Attitude and Practicesamongprimary Care Workers On Infection, Prevention and Control Amidst The Covid-19 PandemicDocument25 pagesKnowledge, Attitude and Practicesamongprimary Care Workers On Infection, Prevention and Control Amidst The Covid-19 PandemicIJAR JOURNALNo ratings yet
- ScheduleDocument7 pagesScheduleapi-296878004No ratings yet
- The New Global Map of Human BrucellosisDocument9 pagesThe New Global Map of Human BrucellosisNouman Safdar AliNo ratings yet
- Sarcoma NCPDocument8 pagesSarcoma NCPginosanNo ratings yet
- Homeopathic Medicine & Pharmacy 1543Document173 pagesHomeopathic Medicine & Pharmacy 1543maxisinc.inNo ratings yet
- Prospectus 2022 MD MSDocument8 pagesProspectus 2022 MD MSarun vNo ratings yet
- Emergency Medicine Dissertation TopicsDocument8 pagesEmergency Medicine Dissertation TopicsBuyCollegePaperSingapore100% (1)
- Advancing Palliative Care in The Public Sector - DrRichardLimDocument26 pagesAdvancing Palliative Care in The Public Sector - DrRichardLimmalaysianhospicecouncil6240100% (1)
- Herbal Drug Interactions A Major Safety ConcernDocument5 pagesHerbal Drug Interactions A Major Safety ConcernSuciPutriRahmawaniNo ratings yet
- Total Gallium JB15939XXDocument18 pagesTotal Gallium JB15939XXAsim AliNo ratings yet
- Student Evaluation Tool-Hail UniversityDocument6 pagesStudent Evaluation Tool-Hail UniversityRichard Balacuit MaestradoNo ratings yet
- Age-Related Differences in Hospitalization Rates, Clinical Presentation, and Outcomes Among Older Adults Hospitalized With Influenza-U.S. Influenza Hospitalization Surveillance NetworkDocument8 pagesAge-Related Differences in Hospitalization Rates, Clinical Presentation, and Outcomes Among Older Adults Hospitalized With Influenza-U.S. Influenza Hospitalization Surveillance NetworkTony RobertsNo ratings yet
- Hospital Literature StudyDocument30 pagesHospital Literature StudyIsaac Jeb80% (10)
- Adls Final Research PosterDocument1 pageAdls Final Research Posterapi-453651228No ratings yet
- Nursing AuditDocument3 pagesNursing AuditJoe Shewale0% (1)
- Rewarding Healthcare Executives in A Dispersed Yet Integrated FirmDocument40 pagesRewarding Healthcare Executives in A Dispersed Yet Integrated FirmDragana AvramovskaNo ratings yet
- Acog Practice Bullet In: Tubal Ectopic PregnancyDocument13 pagesAcog Practice Bullet In: Tubal Ectopic PregnancydlucNo ratings yet
- 8 - Anesthesia and Patient SafetyDocument16 pages8 - Anesthesia and Patient SafetyMilazar NigelNo ratings yet