Download as pdf or txt
You might also like
- CHCCCS025Document80 pagesCHCCCS025kul199080% (20)
- MeningoceleDocument33 pagesMeningoceleAnkira Findoro100% (1)
- Os Roent PDFDocument87 pagesOs Roent PDFTJ OberioNo ratings yet
- 10.1016@B978 0 444 64012 3.00003 4Document13 pages10.1016@B978 0 444 64012 3.00003 4loloasbNo ratings yet
- FTD Psychiatric DDDocument11 pagesFTD Psychiatric DDlaraviNo ratings yet
- The Psychiatric Comorbidity of Epilepsy PDFDocument14 pagesThe Psychiatric Comorbidity of Epilepsy PDFTanjung E SumekarNo ratings yet
- CTP NotesDocument8 pagesCTP Notesrupangishah7No ratings yet
- 1311 IjirmsDocument4 pages1311 Ijirmsbayekha04No ratings yet
- 52 Tripathy EtalDocument5 pages52 Tripathy EtaleditorijmrhsNo ratings yet
- Neuromodulation For The Treatment of Prader-Willi Syndrome - A Systematic ReviewDocument9 pagesNeuromodulation For The Treatment of Prader-Willi Syndrome - A Systematic ReviewCristina Sánchez MoralesNo ratings yet
- Bipolaridade e Esclerose MúltiplaDocument4 pagesBipolaridade e Esclerose MúltiplaLucasFelipeRibeiroNo ratings yet
- Moyamoya-Patient-With-Schizophrenia ACPDocument5 pagesMoyamoya-Patient-With-Schizophrenia ACPCatalinaNo ratings yet
- Adult Presentation of Dyke Davidoff Masson Syndrome With Schizoaffective Disorder - A Case Report - EditedDocument5 pagesAdult Presentation of Dyke Davidoff Masson Syndrome With Schizoaffective Disorder - A Case Report - Editedgion.nandNo ratings yet
- Prion Disease: Kelly J. Baldwin, MD Cynthia M. Correll, MDDocument12 pagesPrion Disease: Kelly J. Baldwin, MD Cynthia M. Correll, MDMerari Lugo Ocaña100% (1)
- Fulltext Jmbmi v3 Id1023Document3 pagesFulltext Jmbmi v3 Id1023adinda.larastitiNo ratings yet
- Indicator of Dyscirculatory Encephalopathy in HypothyroidismDocument4 pagesIndicator of Dyscirculatory Encephalopathy in HypothyroidismresearchparksNo ratings yet
- Neurobiology of SchizophreniaDocument11 pagesNeurobiology of SchizophreniaJerry JacobNo ratings yet
- Braga-13 EOAD PSEN1 Clinica de SCADocument3 pagesBraga-13 EOAD PSEN1 Clinica de SCAMARIA MONTSERRAT SOMOZA MONCADANo ratings yet
- The Successful Treatment of DisinhibitioDocument4 pagesThe Successful Treatment of DisinhibitioVicky NotesNo ratings yet
- Enfermedad de Hungtinton, Afectafción de Ganglios de La Base y Síntomas PsiquiátricosDocument7 pagesEnfermedad de Hungtinton, Afectafción de Ganglios de La Base y Síntomas PsiquiátricosLaura VargasNo ratings yet
- Enf de PickDocument11 pagesEnf de PickAnonymous QzobWmNo ratings yet
- Material Extra Sobre EH - Caso ÚnicoDocument10 pagesMaterial Extra Sobre EH - Caso ÚnicoLaura Andrea Roldan SanchezNo ratings yet
- Neurodevelopmental Risk Factors in SchizophreniaDocument9 pagesNeurodevelopmental Risk Factors in SchizophreniatiwiyunNo ratings yet
- Delirious Mania - An Approach To Diagnosis and TreatmentDocument10 pagesDelirious Mania - An Approach To Diagnosis and TreatmentJaviera Paz Guerrero CassanelloNo ratings yet
- Wjarr 2024 1024Document4 pagesWjarr 2024 1024mcvallespinNo ratings yet
- Fahr's Disease and Psychiatric Syndromes - A Case SeriesDocument3 pagesFahr's Disease and Psychiatric Syndromes - A Case SeriesubuntumicNo ratings yet
- Pisa Syndrome Source Clin Neuropharmacol SO 2015 Jul Aug 38 4 135 40 (PMIDT26166239)Document6 pagesPisa Syndrome Source Clin Neuropharmacol SO 2015 Jul Aug 38 4 135 40 (PMIDT26166239)dai shujuanNo ratings yet
- Behavioural-Variant Frontotemporal Dementia: An Update: Dementia E Neuropsychologia March 2013Document10 pagesBehavioural-Variant Frontotemporal Dementia: An Update: Dementia E Neuropsychologia March 2013claudiaNo ratings yet
- Conversion Disorder: The Brain's Way of Dealing With Psychological Conflicts. Case Report of A Patient With Non-Epileptic SeizuresDocument7 pagesConversion Disorder: The Brain's Way of Dealing With Psychological Conflicts. Case Report of A Patient With Non-Epileptic SeizuresMaria Von Shaft100% (1)
- 2017 - Ijaims - Psychiatric Comorbidities in Patients With EpilepsyDocument5 pages2017 - Ijaims - Psychiatric Comorbidities in Patients With EpilepsySantosh KumarNo ratings yet
- 1 s2.0 S0140673617312874 MainDocument15 pages1 s2.0 S0140673617312874 MainmeryemNo ratings yet
- Frontotemporaldementia: Nicholas T. Olney,, Salvatore Spina,, Bruce L. MillerDocument36 pagesFrontotemporaldementia: Nicholas T. Olney,, Salvatore Spina,, Bruce L. MillerDaniel MartinezNo ratings yet
- Neurologic Manifestations of Wilson's DiseaseDocument6 pagesNeurologic Manifestations of Wilson's DiseaseBarry SeeboNo ratings yet
- Bipolar Disorder and Epilepsy A Bidirectional Relation Neurobiological Underpinnings Current Hypotheses and Future Research DirectionsDocument14 pagesBipolar Disorder and Epilepsy A Bidirectional Relation Neurobiological Underpinnings Current Hypotheses and Future Research DirectionsRudolph MuliawanNo ratings yet
- Leukodystrophy Paper August 27thDocument7 pagesLeukodystrophy Paper August 27thZorbey TurkalpNo ratings yet
- Author 'S Accepted Manuscript: 10.1016/j.psym.2016.05.005Document40 pagesAuthor 'S Accepted Manuscript: 10.1016/j.psym.2016.05.005jose luisNo ratings yet
- Dementia FrontotemporalDocument24 pagesDementia FrontotemporalTeologia GamalielNo ratings yet
- Schneider-11 HD SimilaresDocument12 pagesSchneider-11 HD SimilaresMARIA MONTSERRAT SOMOZA MONCADANo ratings yet
- Fahr Syndrome PDFDocument9 pagesFahr Syndrome PDFRaluca-Andreea IgnatNo ratings yet
- Roberts Psychiatric 1992Document3 pagesRoberts Psychiatric 1992Drashua AshuaNo ratings yet
- Tab VS DFTDocument15 pagesTab VS DFTAntu NandaNo ratings yet
- Essential Tremor: Clinical PracticeDocument9 pagesEssential Tremor: Clinical PracticeDaniel Torres100% (1)
- A Case of Cycloid Psychotic Disorder: M C F, T S - F, B SDocument2 pagesA Case of Cycloid Psychotic Disorder: M C F, T S - F, B Syeremias setyawanNo ratings yet
- hadjsjDocument6 pageshadjsjadamilzaryNo ratings yet
- A New Familial Adult-Onset Leukodystrophy Manifesting As Cerebellar Ataxia and DementiaDocument9 pagesA New Familial Adult-Onset Leukodystrophy Manifesting As Cerebellar Ataxia and DementiaKristineNo ratings yet
- A Case of Sporadic Creutzfeldt-JakobDocument5 pagesA Case of Sporadic Creutzfeldt-JakobVlad PopescuNo ratings yet
- Neuroimaging in Bipolar DisorderDocument13 pagesNeuroimaging in Bipolar DisorderAngie GiraldoNo ratings yet
- Edwards Mark J Why Functional Neurological Disorder IsDocument11 pagesEdwards Mark J Why Functional Neurological Disorder IsSiddika PanjwaniNo ratings yet
- DELIRIUMDocument9 pagesDELIRIUMCaio AlvesNo ratings yet
- A Case of Psychosis Due To Fahr S Syndrome And.19Document3 pagesA Case of Psychosis Due To Fahr S Syndrome And.19VYNo ratings yet
- Creutzfeldt JakobDocument15 pagesCreutzfeldt JakobNicolas RodriguezNo ratings yet
- Case 40-2021 - A 9-Year-Old - Enf - MoyamoyaDocument10 pagesCase 40-2021 - A 9-Year-Old - Enf - MoyamoyaJuan C. Salazar PajaresNo ratings yet
- Bipolar AJMG 2003Document9 pagesBipolar AJMG 2003Gerald Lagi NgantukNo ratings yet
- Review of Hereditary and Acquired Rare ChoreasDocument24 pagesReview of Hereditary and Acquired Rare ChoreasleaNo ratings yet
- PIIS0885392412001224Document12 pagesPIIS0885392412001224Catinca DobroghiiNo ratings yet
- Neurobiology of Bipolar DisorderDocument9 pagesNeurobiology of Bipolar DisorderJerry JacobNo ratings yet
- Neuroimage: Clinical: SciencedirectDocument9 pagesNeuroimage: Clinical: SciencedirectMostafa FakhriNo ratings yet
- Greyson Alexander JNMD 2018Document4 pagesGreyson Alexander JNMD 2018Tibor AbaiNo ratings yet
- Case Report-Traducción LauraDocument4 pagesCase Report-Traducción LauraPablo GuzmánNo ratings yet
- Uncovering The Lifespan Neurobehavioral Comorbidities of EpilepsyDocument30 pagesUncovering The Lifespan Neurobehavioral Comorbidities of EpilepsydhruvaNo ratings yet
- GeneticsDocument10 pagesGeneticsapi-3835615No ratings yet
- Subacute Sclerosing Panencephalitis A Clinical and Pathological Study - 101 108Document7 pagesSubacute Sclerosing Panencephalitis A Clinical and Pathological Study - 101 108Bhanu PratapNo ratings yet
- Neurometabolic Hereditary Diseases of AdultsFrom EverandNeurometabolic Hereditary Diseases of AdultsAlessandro P. BurlinaNo ratings yet
- Magnetic Resonance Imaging: Key Points: CT ImagingDocument5 pagesMagnetic Resonance Imaging: Key Points: CT ImagingadamilzaryNo ratings yet
- Magnetic Resonance Imaging: Key Points: CT ImagingDocument7 pagesMagnetic Resonance Imaging: Key Points: CT ImagingadamilzaryNo ratings yet
- Magnetic Resonance Imaging: Key Points: CT ImagingDocument8 pagesMagnetic Resonance Imaging: Key Points: CT ImagingadamilzaryNo ratings yet
- Magnetic Resonance Imaging: Key Points: CT ImagingDocument8 pagesMagnetic Resonance Imaging: Key Points: CT ImagingadamilzaryNo ratings yet
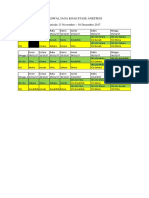
- Jadwal Jaga Koas Stase Anestesi Periode 13 November - 10 Desember 2017Document1 pageJadwal Jaga Koas Stase Anestesi Periode 13 November - 10 Desember 2017adamilzaryNo ratings yet
- University of Saint Louis Tuguegarao City, Philippines: Maternal and Child Health NursingDocument69 pagesUniversity of Saint Louis Tuguegarao City, Philippines: Maternal and Child Health NursingErica Veluz LuyunNo ratings yet
- Clinical Review: Common Skin Infections in ChildrenDocument5 pagesClinical Review: Common Skin Infections in ChildrenkhairaniNo ratings yet
- Yetmgeta Abdella 2018Document11 pagesYetmgeta Abdella 2018Shafici CqadirNo ratings yet
- Mental Status ExaminationDocument98 pagesMental Status ExaminationFatima 'No ratings yet
- Varicella Immunization CertDocument2 pagesVaricella Immunization CertShaikahamedNo ratings yet
- The OMT Classification of Congenital Anomalies - Michael A. TonkinDocument7 pagesThe OMT Classification of Congenital Anomalies - Michael A. TonkindougortoNo ratings yet
- Abstract Book PVSM2021 FinalDocument374 pagesAbstract Book PVSM2021 FinalnitaNo ratings yet
- Longrichglobal Retail or Maintenance BonusDocument1 pageLongrichglobal Retail or Maintenance BonusdxpfzbbcqvNo ratings yet
- Medical ReportsDocument1 pageMedical Reportsraheemtimo1No ratings yet
- Baroreflex Failure: A Neglected Type of Secondary HypertensionDocument5 pagesBaroreflex Failure: A Neglected Type of Secondary HypertensionMichel HaddadNo ratings yet
- Mamusha PDFDocument72 pagesMamusha PDFFikadu WendmtayeNo ratings yet
- A Study On Impact of Covid - 19 On Indian Pharmaceutical CompaniesDocument9 pagesA Study On Impact of Covid - 19 On Indian Pharmaceutical CompaniesAnonymous CwJeBCAXpNo ratings yet
- 432 eDocument404 pages432 eIJAZ M RAHMANNo ratings yet
- JACC Volume 78, Issue 11 SeptemberDocument122 pagesJACC Volume 78, Issue 11 SeptemberFareesha KhanNo ratings yet
- DivergentesDocument12 pagesDivergentesA LunaNo ratings yet
- Annotated Bibliography of Traditional Medicine Research Carried Out at DMR (LM) During 1965-2011Document271 pagesAnnotated Bibliography of Traditional Medicine Research Carried Out at DMR (LM) During 1965-2011AyeChan AungNo ratings yet
- Part 1 Module First Aid and CPRDocument25 pagesPart 1 Module First Aid and CPRWinter SongNo ratings yet
- Primer: Frozen ShoulderDocument16 pagesPrimer: Frozen ShoulderJose PerezNo ratings yet
- MEDICAL-REIUMBURSEMENT-G O Ms No 74Document19 pagesMEDICAL-REIUMBURSEMENT-G O Ms No 74cgr7880% (5)
- Pericardial Diseases: Dr. Abazie, Ugochi CDocument63 pagesPericardial Diseases: Dr. Abazie, Ugochi CUgochi AbazieNo ratings yet
- Flash CardsDocument793 pagesFlash CardsbtheresakNo ratings yet
- NatureDP 2015 Chronic Obstructive Pulmonary DiseaseDocument21 pagesNatureDP 2015 Chronic Obstructive Pulmonary DiseasePaloma GBNo ratings yet
- Cobas b101 PDFDocument6 pagesCobas b101 PDFGolden Flower ATLMNo ratings yet
- Lai Et Al-2016-Cochrane Database of Systematic ReviewsDocument181 pagesLai Et Al-2016-Cochrane Database of Systematic ReviewsIgnacia VergaraNo ratings yet
- The Principles of The Surgical Management of Gastric CancerDocument5 pagesThe Principles of The Surgical Management of Gastric CancerRobert ChristevenNo ratings yet
- MS2760 HiViral Mediu de Transport KitDocument2 pagesMS2760 HiViral Mediu de Transport KitLidia NarbNo ratings yet
- International Journal of Nursing Studies: Qi Lu, Jan Mårtensson, Yue Zhao, Linda JohanssonDocument8 pagesInternational Journal of Nursing Studies: Qi Lu, Jan Mårtensson, Yue Zhao, Linda JohanssonAbdul HadiNo ratings yet