Professional Documents
Culture Documents
Cognitive Behavioral Therapy for Depression.11
Cognitive Behavioral Therapy for Depression.11
Uploaded by
praveen.med87Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Cognitive Behavioral Therapy for Depression.11
Cognitive Behavioral Therapy for Depression.11
Uploaded by
praveen.med87Copyright:
Available Formats
CLINICAL PRACTICE GUIDELINES
Cognitive Behavioral Therapy for Depression
Manaswi Gautam, Adarsh Tripathi1, Deepanjali Deshmukh2, Manisha Gaur3
Consultant Psychiatrist Gautam Hospital and Research Center, Jaipur, 3Consultant Psychologist, Gaur Mental Health Clinic,
Downloaded from http://journals.lww.com/indianjpsychiatry by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4
Ajmer, Rajasthan, 1Department of Psychiatry, King George’s Medical University, Lucknow, Uttar Pradesh, 2MGM Medical
XMi0hCywCX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC4/OAVpDDa8KKGKV0Ymy+78= on 03/18/2024
College, Aurangabad, Maharashtra, India
INTRODUCTION EVIDENCE BASE FOR COGNITIVE
BEHAVIORAL THERAPY IN DEPRESSION
Depressive disorders are one of the most common
psychiatric disorders that occur in people of all ages Cognitive behavioral therapy (CBT) is one of the most
across all world regions. Although it may present at any evidence‑based psychological interventions for the
age however adolescence to early adults is the most treatment of several psychiatric disorders such as
common age of onset, and females are affected two depression, anxiety disorders, somatoform disorder, and
times more in comparison to the males. Depressive substance use disorder. The uses are recently extended
disorders can occur as heterogeneous conditions in to psychotic disorders, behavioral medicine, marital
clinical scenario ranging from transient minor symptoms discord, stressful life situations, and many other clinical
to severe and debilitating clinical conditions, causing conditions.
severe social and occupational impairments. Usually,
it presents with constellations of cognitive, emotional, A sufficient number of researches have been conducted
behavioral, physiological, interpersonal, social, and and shown the efficacy of CBT in depressive disorders.
occupational symptoms. The illness can be of various A meta‑analysis of 115 studies has shown that CBT is an
severities, and a significant proportion of the patients effective treatment strategy for depression and combined
can have recurrent illness. Depression is also highly treatment with pharmacotherapy is significantly more
effective than pharmacotherapy alone.[2] Evidence also
comorbid with several psychiatric and medical illnesses
suggests that relapse rate of patient treated with CBT
such as anxiety disorders, substance use, obsessive–
is lower in comparison to the patients treated with
compulsive disorder, diabetes, hypertension, and
pharmacotherapy alone.[3]
cardiovascular illnesses.
Treatment guidelines for the depression suggest that
Major depressive disorders accounted for around 8.2%
psychological interventions are effective and acceptable
global years lived with disability (YLD) in 2010, and it was
strategy for treatment. The psychological interventions
the second leading cause of the YLDs. In addition, they are most commonly used for mild‑to‑moderate depressive
also contribute to the burden of several other disorders episodes. As per the prevailing situations of India
indirectly such as suicide and ischemic heart disease.[1] with regards to significant lesser availability of trained
therapist in most of the places and patients preferences,
Address for correspondence: Dr. Manaswi Gautam,
Director and Consultant Psychiatrist, Gautam Hospital and the pharmacological interventions are offered as
Research Center, Jaipur. the first‑line treatment modalities for treatment of
E‑mail: dr.m.gautam@gmail.com depression.
Received: 12th December, 2019, Accepted: 16th December, 2019,
Publication: 17th January, 2020 This is an open access journal, and articles are distributed under the terms of
the Creative Commons Attribution‑NonCommercial‑ShareAlike 4.0 License,
Access this article online which allows others to remix, tweak, and build upon the work non‑commercially,
as long as appropriate credit is given and the new creations are licensed under
Quick Response Code
the identical terms.
Website:
www.indianjpsychiatry.org For reprints contact: reprints@medknow.com
DOI:
How to cite this article: Gautam M, Tripathi A, Deshmukh D,
Gaur M. Cognitive behavioral therapy for depression. Indian
10.4103/psychiatry.IndianJPsychiatry_772_19
J Psychiatry 2020;62:S223-9.
© 2020 Indian Journal of Psychiatry | Published by Wolters Kluwer - Medknow S223
Gautam, et al.: Guidelines for CBT in depression
Indication for Cognitive behavior therapy as enlisted in THE USE OF COGNITIVE BEHAVIORAL
table 1. THERAPY ACCORDING TO SEVERITY OF
DEPRESSION
CONTRAINDICATIONS FOR COGNITIVE
BEHAVIORAL THERAPY Various trials have shown the benefit of combined treatment
for severe depression.
There is no absolute contraindication to CBT; however, it is
Combined therapy though costlier than monotherapy it
Downloaded from http://journals.lww.com/indianjpsychiatry by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4
often reported that clients with comorbid severe personality
XMi0hCywCX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC4/OAVpDDa8KKGKV0Ymy+78= on 03/18/2024
disorders such as antisocial personality disorders and provides cost‑effectiveness in the form of relapse prevention.
subnormal intelligence are difficult to manage through
CBT. Special training and expertise may be needed for the Number of sessions depends on patient responsiveness.
treatment of these clients.
Booster sessions might be required at the intervals of the
Patient with severe depression with psychosis and/or 1–12th month as per the clinical need.
suicidality might be difficult to manage with CBT alone
and need medications and other treatment before A model for reference is given in table 3
considering CBT. Organicity should be ruled out using
clinical evaluation and relevant investigations, as and The general outline of CBT for depression has been
when required. discussed in table 4
COGNITIVE MODEL FOR DEPRESSION
There are many advantages of CBT in depression as given
in table 2
Cognitive theory conceptualizes that people are not
influenced by the events rather the view they take of the
CHOICE OF TREATMENT SETTINGS
events. It essentially means that individual differences in
the maladaptive thinking process and negative appraisal
CBT can be done on an Out Patient Department (OPD) basis
of the life events lead to the development of dysfunctional
with regular planned sessions. Each session lasts for
cognitive reactions. This cognitive dysfunction is in turn is
about 45 min–1 h depending on the suitability for both
responsible for the rest of the symptoms in affective and
patients and therapists. In specific situations, the CBT can
behavioral domains.
be delivered in inpatient settings along with treatment as
usual such as adjuvant treatment in severe depression, high
Aaron beck proposed a cognitive model of depression, and
risk for self‑harm or suicidal patients, patients with multiple it is detailed in Figure 1. Cognitive dysfunctions are of the
medical or psychiatric comorbidities and in patients following categories.
hospitalized due to social reasons. • Schema ‑ stable internal structure of information usually
formed during early life, also include core belief about
ASSESSMENT AND EVALUATION FOR THE self
THERAPY • information processing and intermediate belief are
usually interpreted as rules of living and usually
A detail diagnostic assessment is needed for the assessment expressed in terms of “if and then” sentences
of psychopathology, premorbid personality, diagnosis, • Automatic thoughts ‑ proximally related to everyday
severity, presence of suicidal ideations, and comorbidities. events and in depression, often reflects cognitive triad,
Baseline assessment of severity using a brief scale will be i.e., negative view of oneself, world, and future.
helpful in mutual understanding of severity before starting
therapy and also to track the progress. Clients during Negative cognitive triad of depression as given beck is as
depressive illness often fail to recognize early improvement following:
and undermine any positive change. Objective rating scale • I am helpless (helplessness)
hence helps in pointing out the progress and can also help in • The future is bleak (hopelessness)
determining agenda during therapy process. Beck Depression • I am worthless (worthlessness).
Inventory (A. T. Beck, Steer, and Brown, 1996), the Depression
Anxiety Stress Scales (Lovibond and Lovibond, 1995), CHOICE OF THE PATIENT
Montgomery‑Asberg Depression Rating Scale, Hamilton
Rating Scale for Depression are useful rating scales for this Patient‑related factors that facilitated response are
purpose. The assessment for CBT in depression is, however, 1. Psychological mindedness of patients: Patients who
different from diagnostic assessment. are able to understand and label their feelings and
S224 Indian Journal of Psychiatry, Volume 62 (Supplement 2), January 2020
Gautam, et al.: Guidelines for CBT in depression
Some common symptoms and associated automatic
thoughts are given in table 5.
Impact on functioning
it is important to know the extent and effect of depression
on the overall functioning and interpersonal relationships.
Downloaded from http://journals.lww.com/indianjpsychiatry by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4
Coping strategies
XMi0hCywCX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC4/OAVpDDa8KKGKV0Ymy+78= on 03/18/2024
Sometimes patients with depression might have adapted
a coping strategies which make them feel good for short
duration (e.g., alcohol consumption) but might be unhealthy
in long term.
Figure 1: Cognitive behavioral therapy model of depression Onset of current symptoms
Patient’s perception about the situation at the onset
emotions generally respond better to CBT. Although of symptoms might provide useful information about
some patients in the course of treatment learn those underlying cognitive distortions.
skills during treatment
2. Intellectual level of the patient might also affect the Background information
overall effectiveness of the treatment Detailed history of patient is necessary, including patients
3. Willingness and motivation on the part of patients: premorbid personality.
Although it is not prerequisite, patients who are
motivated to analyze their feelings and ready to The therapist should be able to do the cognitive case
undergo various homework show a better response to conceptualization for the patient as given in Figure 2.
treatment
4. Patient preference is single most important factor: MANAGING TREATMENT
After initial assessment of the patient those who prefer
psychological treatment can be offered CBT alone or in An outline of the breakup of typical session of CBT is given
combination depending on type of depression in table 6.
5. Those with mild to moderate depression CBT can be
recommended as a first line of treatment Starting treatment
6. Patients with severe depression might need First treatment interview has mainly four objectives:
combination of both CBT and medications (and or 1. To establish a warm collaborative therapeutic alliance
other treatments) 2. To list specific problem set and associated goals
7. Special situations such as children and adolescents, 3. To psycho‑educate patient regarding the cognitive
pregnancy, lactation, female in fertile age group model and vicious cycle that maintains the depression
planning for pregnancy, medical comorbidities 4. Give the patient idea about further treatment
8. Inability to tolerate psychopharmacological treatment procedures.
9. The presence of significant psychosocial factors,
intrapsychic conflicts, and interpersonal difficulties. CBT can be explained in the following headings
a. Starting treatment
Therapist related factors b. Behavioral interventions
1. Availability of cognitive behavioral therapist/ c. Working with negative automatic thoughts
psychiatrist d. Ending session.
2. The ability of therapist to form therapeutic alliance
with the patient. Starting treatment
The first treatment interview has four main objectives:
CLINICAL INTERVIEW FOR COGNITIVE 1. To establish a warm, collaborative therapeutic alliance
BEHAVIORAL THERAPY 2. To list specific problems and associated goals, and
select a first problem to tackle
Symptoms and associated cognitions 3. To educate the patient about the cognitive
Negative automatic thoughts both trigger and enhance model, especially the vicious circle that maintains
depression. It might be helpful to identify unhealthy depression
automatic thoughts associated with symptoms of 4. To give the patient first‑hand experience of the focused,
depression. workman‑like, empirical style of CBT.
Indian Journal of Psychiatry, Volume 62 (Supplement 2), January 2020 S225
Gautam, et al.: Guidelines for CBT in depression
These convey two important messages: (1) It is possible Activity Chart
Write in each box, activity performed and depression rating from
to make sense of depression; (2) there is something the 0-100% (0-minimal, 100-maximum)
patient can do about it. These messages directly address Time Monday Tuesday Wednesday Thursday Friday Saturday Sunday
6-7 AM
hopelessness and helplessness. 7-8 AM
8-9 AM* Breakfast, Breakfast Walk, 30% Breakfast Talk Breakfast Breakfast
I. Identifying problems and goals:‑The various problems talk with alone, with son, with alone, with
faced by patients should be included in a list which can wife, 60% 50% friend on 60% everyone
Downloaded from http://journals.lww.com/indianjpsychiatry by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4
40% phone, in family,
XMi0hCywCX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC4/OAVpDDa8KKGKV0Ymy+78= on 03/18/2024
include symptoms of depression or social problems 20% 20%
10-11 PM Hourly What
(e.g., family conflict). Developing this list at the end of rating everyone
from must be
the first session helps in planning treatment goals waking thinking
up till about
time to me
II. Introducing cognitive model of depression:‑ In the first sleep
session at least a basic idea about how our cognitions *example
affect our emotions and behavior is taught to the
patient. The data provided by patient can be used to Planning activities
Once the patient learns to self‑monitor activities each day is
give insight into behaviors
planned in advance.
III. Where to start:‑Common treatment goal is agreed upon
by patient and therapist, therapeutic alliance is of key This helps patients by:
importance in CBT. Appropriate homework assignment 1. This provides a structure and helps with setting
priorities
should be given to patient according to predecided 2. This avoids the need to keep making decisions about
goal. what to do next
3. This changes perception from chaos to manageable
Behavioural interventions tasks
Reducing ruminations 4. This increases the chances that activities will be carried
out
It has been seen that depressed patients spend a
5. This enhances patients’ sense of control.
significant amount of time and attention focusing on their
shortcomings. Making patient aware of those negative A plan for activities is made in such a way that both
ruminations and consciously diverting attention toward pleasure and mastery are balanced (e.g., ironing cloths
followed by listening to music). The tasks which are
certain positive aspects can be taught to patients.
generally avoided by patient can be divided into graded
tasks.
Monitoring activities
Loss of interest in day to day activities is central to the The patient is taught to evaluate each and every day in detail
depression. It has been seen that early behavioral intervention also encouraged to keep the record of unhelpful negative
thoughts regarding tasks.
has been increased sense of autonomy in the patients.
Other important behavioral activities are:‑
Patients are taught to record each and every activity hour 1. Mindfulness meditation: Helps people stay grounded in
by hour on the activity schedule. Each activity is rated 0–10 the present by keeping away from ruminations
for Pleasure (P) and Mastery (M). P ratings indicate how 2. Successive approximation: Breaking larger tasks into
smaller tasks which are easy to accomplish
enjoyable the activity was, and M ratings how much of an
3. Visualizing the best part of the day
achievement it was. Mostly depressed patients feel low on 4. Pleasant activity scheduling.
achievement all the time. Hence, M should be explained as
“achievement how you felt at the time of doing.” Patients Scheduling an activity in near future which one can look on
with mastery and with sense of achievement.
are instructed to rate activities immediately and not
retrospectively. Working with negative automatic thoughts
The main tool for this negative automatic thought
Example of activity schedule is record.
S226 Indian Journal of Psychiatry, Volume 62 (Supplement 2), January 2020
Gautam, et al.: Guidelines for CBT in depression
Thought Record -1 possible, more likely outcomes. Example: “I ll be so
Situation Emotions (Rate Behaviour Physical Automatic upset, i won’t be able to function at all”
(write down 0-100%) reactions thoughts/ • Disqualifying or discounting the positive: The person
exact details images (Identify unreasonably tell oneself that positive experiences,
of specific most important deeds, or qualities do not count. Example: “I cracked
situation) thought)
the examl, but that doesn’t mean I’m competent; It was
Thought Record – 2 a fluke”
• Emotional reasoning: One thinks something must be true
Downloaded from http://journals.lww.com/indianjpsychiatry by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4
Situation Emotions Automatic Evidence Evidence Balanced Rate
XMi0hCywCX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC4/OAVpDDa8KKGKV0Ymy+78= on 03/18/2024
(write down (Rate thoughts/ images for against thought emotion because he/she “feels” (actually believe) it so strongly,
exact details 0-100%) (Identify most automatic automatic now (0- ignoring or discounting evidence to the contrary.
of specific important thoughts thoughts 100%) Example: “I know I successfully complete most of my
situation) thought)
tasks, but I still feel like I’ m incompetent”
• Labeling: One puts a fixed, global label on oneself or
Identifying negative automatic thoughts others without considering that the evidence might
Patients learn to record upsetting incidents as soon as more reasonably lead to a less disastrous conclusion.
possible after they occur (delay makes it difficult to recall Example: “I’m a failure. He’s not good enough”
thoughts and feelings accurately). They learn: • Magnification/minimization: When one evaluates
a. To identify unpleasant emotions (e.g., despair, anger, oneself, another person, or a situation, one
guilt), signs that negative thinking is present. Emotions unreasonably magnifies the negative and/or minimizes
are rated for intensity on a 0–100 scale. These the positive. Example: “Getting a C Grade in exams
ratings (though the patient may initially find them proves how mediocre I am. Getting high marks doesn’t
difficult) help to make small changes in emotional state mean I’m smart”
obvious when the search for alternatives to negative • Selective abstraction (also called mental filter): One pays
thoughts begins. This is important since change is rarely undue attention to one’s negative detail instead of
all‑or‑nothing, and small improvements may otherwise seeing the whole picture. Example: “Because I got just
be missed passing marks in one subject in my examinations (which
b. To identify the problem situation. What was the also contained distinctions in other subjects) it means
patient doing or thinking about when the painful I’m not a good student”
emotion occurred (e.g., “waiting at the supermarket • Mind reading: One believes that he/she knows what
checkout,” “worrying about my husband being late others are thinking, failing to consider other, more
home”)? likely possibilities. Example: “He assumes that his boss
c. To identify negative automatic thoughts associated thinks that he is a novice for this assignment”
with the unpleasant emotions. Sessions direct the • Overgeneralization: One makes a negative conclusion
therapist towards asking: “And what went through that goes far beyond the current situation. Example:
your mind at that moment?” Patients become aware of “(Because I felt uncomfortable at the meeting) I don’t
thoughts, images, or implicit meanings that are present have what it takes to be a group leader”
when emotional shifts occur, and record. Belief in each • Personalization: One believes others are behaving
thought is also rated on a 0%–100%. negatively because of him/her, without exploring
alternative explanations for their behavior. Example:
Questioning negative automatic thoughts “The watchman didn’t smile at me because I did
Therapist can help patient to discover dysfunctional something wrong”
automatic thoughts through “guided discovery.” • Imperatives (also called “Should” and “must”
1. What is evidence? statements): One has a precise, fixed idea of how one or
2. What are alternative views? others should behave, and they overestimate how bad
3. What are advantages and disadvantages of this way of it is that these expectations are not met with. Example:
thinking? “It’s terrible that I sneeze as I am a Gym Trainer”
4. What are my thinking biases? • Tunnel vision: One only views the negative aspects of a
situation. Example: “My subordinate can’t do anything
Common cognitive distortions are right. He’s callous, casual and insensitive towards his
• Black– and– white (also called all– or– nothing, polarized, job.”
or dichotomous thinking): Situations viewed in only
two categories instead of on a continuum. Example: “If Testing negative automatic thoughts: What can I do now?
I don’t top the exams. I’m a failure” It is important that cognitive changes that are brought
• Fortune‑telling (also called catastrophizing): Future out by questioning are consolidated by behavior
is predicted negatively without considering other experiments.
Indian Journal of Psychiatry, Volume 62 (Supplement 2), January 2020 S227
Gautam, et al.: Guidelines for CBT in depression
Ending the treatment I. Where did this rule come from? Identifying the source
CBT is time‑limited goal‑directed form of therapy. Hence, of a dysfunctional assumption (e.g., parental criticism)
the patient is made aware about end of treatment in often helps to encourage distance by suggesting that
advance. This can be done through the following stages. its development is understandable, though it may no
1. Dysfunctional assumptions identification longer be relevant or useful
2. Consolidating learning blueprint II. In what ways is the rule unrealistic? Dysfunctional
3. Preparation for the setback. assumptions do not fit the way the world works. They
Downloaded from http://journals.lww.com/indianjpsychiatry by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4
operate by extremes, which are reflected in their
XMi0hCywCX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC4/OAVpDDa8KKGKV0Ymy+78= on 03/18/2024
Dysfunctional assumptions identification language (always/never rather than some of the time;
Once the patient is able to identify negative automatic must/should/ought rather than want/prefer/would
thoughts. Before ending treatment patient patients should like)
be made aware about dysfunctional assumptions. III. In what ways is the rule helpful? Dysfunctional
assumptions are not usually wholly negative in their
effects. For example, perfectionism may lead to
genuine, high‑quality performance. If such advantages
are not recognized and taken into account when
new assumptions are formulated, the patient may be
reluctant to move forward
IV. In what ways is the rule unhelpful? The advantages of
dysfunctional assumptions are normally outweighed by
their costs. Perfectionism leads to rewards, but it also
undermines satisfaction with achievements and stops
people learning from constructive criticism
V. What alternative rule might be more realistic
and helpful? Once the old assumption has been
Figure 2: Case conceptualization for the cognitive model of undermined, it is helpful to formulate an explicit
depression alternative (e.g., “It is good to do things well, but I
am only human‑sometimes I make mistakes”). This
Table 1: Indications for cognitive behavioral provides a new guideline for living, rather than simply
therapy (situations that can call for preferred use of the undermining the old system
psychological interventions) are VI. What needs to be done to consolidate the new rule?
1. Client’s preference As with negative automatic thoughts, re‑evaluation
2. Availability and accessibility of the trained therapist is best made real through experience: Behavioral
3. Special situations like children and adolescents, pregnancy, lactation,
female in fertile age group planning for pregnancy, medical comorbidities,
experiments.
etc.
4. Inability to tolerate psychopharmacological treatments Consolidating learning blueprint
5. The presence of significant psychosocial factors, intrapsychic conflicts, The patient should be able to summarize whatever he has
and interpersonal difficulties
learned throughout the sessions.
Table 2: Advantages of cognitive behavioral therapy in The following questions might help to set the framework:
depression I. How did my problems develop? (unhelpful beliefs
1. It is used to reduce symptoms of depression as an independent treatment and assumptions, the experiences that led to their
or in combination with medications formation, events precipitating onset)
2. It is used to modify the underlying schemas or beliefs that maintain the II. What kept them going? (maintenance factors)
depression
3. It can be used to address various psychosocial problems, for example,
III. What did I learn from therapy that helped? Techniques
marital discord, job stress which can contribute to the symptoms (e.g., activity scheduling) and Ideas (e.g., “I can do
4. Reduce the chances of recurrence something to influence my mood”)
5. Increase the adherence to recommended medical treatment IV. What were my most unhelpful negative thoughts and
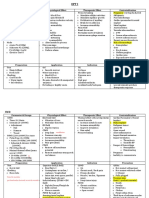
Table 3: The use of cognitive behavioral therapy according to the severity of depression
Type of depression First line Adjunctive Number of sessions
Mild CBT or medication CBT or medication 8–12
Moderate CBT or medication CBT or medication 8–16
Severe Medication or/and Somatic treatment CBT 16 or more
Chronic depression and recurrent depression CBT or medication CBT or medication 16 or more and booster sessions up to 1–2 years
S228 Indian Journal of Psychiatry, Volume 62 (Supplement 2), January 2020
Gautam, et al.: Guidelines for CBT in depression
Table 4: Overview of cognitive behavioral therapy for V. How can I build on what I have learned? (a solid,
depression practical, clearly specified action plan).
1. Mutually agreed on problem definition by therapist and client
2. Goal settings Preparation for the setback
3. Explaining and familiarizing client with five area model of CBT Since depression is recurring illness patient should be made
4. Improving awareness and understanding on one’s cognitive activity and aware about the possibility of relapse.
behavior
5. Modification of thoughts and behavior ‑ using principles of Socratic
I. What might lead to a setback for me? For example,
future losses (e.g., children leaving home) and
Downloaded from http://journals.lww.com/indianjpsychiatry by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4
dialogue, guided discovery, and behavioral experiments/exposure exercise
XMi0hCywCX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC4/OAVpDDa8KKGKV0Ymy+78= on 03/18/2024
6. Application and consolidation of new skills and strategies in therapy stresses (e.g., financial difficulties), i.e., events which
sessions and homework sessions to generalize it across situations impinge on patients’ vulnerabilities and are thus liable
7. Relapse prevention to be interpreted negatively
8. End of the therapy
II. What early warning signs do I need to be alert for?
CBT – Cognitive behavioral therapy
III. Feelings, behaviors, and symptoms that might indicate
the beginning of another depression are identified and
Table 5: Symptoms of depression and associated listed
cognitions IV. If I notice that I am becoming depressed again, what
Serial Symptoms Automatic thoughts should I do? Clear simple instructions, which will make
number sense despite low mood, are needed here. Specific ideas
1 Behavioral: lower I cants do it. It is too much for me and techniques summarized earlier in the blueprint
activity levels
should be referred to.
2 Guilt I am letting everybody down
3 Shame What everyone must be thinking
about me Financial support and sponsorship
Nil.
Table 6: Session structure of cognitive behavioral Conflicts of interest
therapy There are no conflicts of interest.
Serial Component Time (min)
number
REFERENCES
1 Beginning of the session
Mood check 5–10 1. Beck J, Hindman R. Cognitive therapy. In: Sadock B, Sadock V, Ruiz P,
Agenda setting editors. Kaplan & Sadock’s Comprehensive Textbook of Psychiatry.
Reviewing homework New Delhi: Wolter Kluwer India Pvt Ltd.; 2017. p. 2760‑74.
2 Discussion of agenda items/problems 35–40 2. Fennell M. Cognitive behaviour therapy for depressive disorders. In:
Gelder M, Andreasen N, Lopez‑Ibor J, Geddes J, editors. New Oxford
Description of occurrence of specific problem Textbook of Psychiatry. New York: Oxford University Press; 2012.
Elicitation and confirmation of elements of p. 1304‑12.
the cognitive model 3. American Psychiatric Association. Practice Guideline for the Treatment
Collaborative discussion regarding how to of Patients with Major Depressive Disorder. American Psychiatric
approach a problem Association; 2010. Available from: http://psychiatryonline.org/content.asp
x?bookid=28§ionid=1667485.
Rationale for the introduction of intervention 4. Dimidjian S, Hollon SD, Dobson KS, Schmaling KB, Kohlenberg RJ,
Assessment of the efficacy of intervention Addis ME, et al. Randomized trial of behavioral activation, cognitive
Summary by patient therapy, and antidepressant medication in the acute treatment of adults
Collaborative action plan in writing with major depression. J Consult Clin Psychol 2006;74:658‑70.
Planning and discussing a homework and 5. Pampallona S, Bollini P, Tibaldi G, Kupelnick B, Munizza C. Combined
pharmacotherapy and psychological treatment for depression:
how to approach it
A systematic review. Arch Gen Psychiatry 2004;61:714‑9.
3 Feedback to the therapist 1–2 6. Shapiro DA, Barkham M, Rees A, Hardy GE, Reynolds S, Startup M. Effects
of treatment duration and severity of depression on the effectiveness of
cognitive‑behavioral and psychodynamic‑interpersonal psychotherapy.
assumptions? What alternatives did I find to them? J Consult Clin Psychol 1994;62:522‑34.
7. Boyes A. 2012. Available from: https://www.psychologytoday.com/blog/
(summarized in two columns) in‑practice/201212/cognitive‑behavioral‑therapy‑techniques‑work.
Indian Journal of Psychiatry, Volume 62 (Supplement 2), January 2020 S229
You might also like
- Pat Ogden Sensorimotor Therapy PDFDocument16 pagesPat Ogden Sensorimotor Therapy PDFEmili Giralt GuarroNo ratings yet
- Test Bank For Raus Respiratory Care Pharmacology 9th Edition by GardenhireDocument10 pagesTest Bank For Raus Respiratory Care Pharmacology 9th Edition by Gardenhiredavidcunninghampxfcqoanwg100% (23)
- Goldman-Cecil Medicine 26th Edition 2020 (Dragged)Document14 pagesGoldman-Cecil Medicine 26th Edition 2020 (Dragged)rpascua123100% (1)
- Is Mindfulness For Psychosis Harmful? Deconstructing A Myth: EditorialDocument2 pagesIs Mindfulness For Psychosis Harmful? Deconstructing A Myth: EditorialReinhold MuñozNo ratings yet
- C PG For DepressionDocument8 pagesC PG For DepressionGabriela LalaNo ratings yet
- Psychosomatic Disorder SummaryDocument2 pagesPsychosomatic Disorder Summarysaurabh patelNo ratings yet
- CPGfordepressionDocument8 pagesCPGfordepressionGabriela LalaNo ratings yet
- Jurnal 1Document1 pageJurnal 1irfan permanaNo ratings yet
- Cognitive Behavioral Therapy For Depression: Indian Journal of Psychiatry January 2020Document8 pagesCognitive Behavioral Therapy For Depression: Indian Journal of Psychiatry January 2020Nur IlyaniNo ratings yet
- Depression and Psychodynamic Psychotherapy: Special ArticleDocument5 pagesDepression and Psychodynamic Psychotherapy: Special ArticleLuciano RestrepoNo ratings yet
- Deprescribing Antipsychotics A Guide For CliniciansDocument8 pagesDeprescribing Antipsychotics A Guide For CliniciansHei eaNo ratings yet
- CBT in Cancer Patients ST PDFDocument16 pagesCBT in Cancer Patients ST PDFMerve ApaydınNo ratings yet
- Comparing Mindfulness Based Cognitive THDocument5 pagesComparing Mindfulness Based Cognitive THolgasacristan316No ratings yet
- Clinical Practice Guidelines For Psychoeducation.19Document5 pagesClinical Practice Guidelines For Psychoeducation.19Sam InvincibleNo ratings yet
- Narrative Cognitive Behavior Therapy For PsychosisDocument12 pagesNarrative Cognitive Behavior Therapy For PsychosisGanellNo ratings yet
- Cognitive-Behavioral Therapy For DepressionDocument7 pagesCognitive-Behavioral Therapy For DepressionTri Utami HandayaniNo ratings yet
- Cognitive-BehaviouralTherapyinCancerPatients (1) - Brief CBT For CancerDocument23 pagesCognitive-BehaviouralTherapyinCancerPatients (1) - Brief CBT For CancerfitranoenoeNo ratings yet
- Depression and Psychodynamic PsychotherapyDocument5 pagesDepression and Psychodynamic PsychotherapyRija ChoudhryNo ratings yet
- Wuthrich 2013Document8 pagesWuthrich 2013Rafael MoraesNo ratings yet
- Jumping To Conclusions: The Psychology of Delusional ReasoningDocument8 pagesJumping To Conclusions: The Psychology of Delusional ReasoningfranciscoNo ratings yet
- NIH Public Access: Author ManuscriptDocument16 pagesNIH Public Access: Author ManuscriptMuhammad NizarNo ratings yet
- Meta AnalysisDocument15 pagesMeta AnalysisLuciano RestrepoNo ratings yet
- Halford e Brown 2009 - CBT As An Adjunctive Treatment in Chronic Physical IllnessDocument13 pagesHalford e Brown 2009 - CBT As An Adjunctive Treatment in Chronic Physical IllnessRaquel PintoNo ratings yet
- Libro - Psico - Oncología-429-434Document6 pagesLibro - Psico - Oncología-429-434GUILLERMO ANDRÉS ALDANANo ratings yet
- 1 s2.0 S0007091217329677 MainDocument5 pages1 s2.0 S0007091217329677 MainAndy OrtizNo ratings yet
- Psychotherapy: PsychoanalysisDocument3 pagesPsychotherapy: PsychoanalysismohamadNo ratings yet
- Bauer Et Al 2015Document20 pagesBauer Et Al 2015ArjohnaNo ratings yet
- Adjunctive Psychotherapy For Bipolar DisorderDocument10 pagesAdjunctive Psychotherapy For Bipolar DisorderAgustin NunezNo ratings yet
- ABPSY 1 Mood DisordesDocument19 pagesABPSY 1 Mood DisordesCarm RiveraNo ratings yet
- Approach To Consultation Psychiatry: Assessment Strategies: John Querques, M.D. Theodore A. Stern, M.DDocument8 pagesApproach To Consultation Psychiatry: Assessment Strategies: John Querques, M.D. Theodore A. Stern, M.DDaniel MartinezNo ratings yet
- New Research in Psychooncology: Current Opinion in Psychiatry April 2008Document6 pagesNew Research in Psychooncology: Current Opinion in Psychiatry April 2008José Carlos Sánchez-RamirezNo ratings yet
- New Research in Psychooncology: Current Opinion in Psychiatry April 2008Document6 pagesNew Research in Psychooncology: Current Opinion in Psychiatry April 2008JoseNo ratings yet
- Alvarado (2017) Psychotherapeutic Treatment Approaches of Anxiety Disorders in The ElderlyDocument8 pagesAlvarado (2017) Psychotherapeutic Treatment Approaches of Anxiety Disorders in The ElderlyLina MartínezNo ratings yet
- Emotions Regulations Recent FindingsDocument7 pagesEmotions Regulations Recent FindingsPaulo GomesNo ratings yet
- SR Inc 1Document9 pagesSR Inc 1DWIINDAHNo ratings yet
- Treating Mental Disorders: Pharmacotherapy PsychotherapyDocument3 pagesTreating Mental Disorders: Pharmacotherapy Psychotherapytheo van hykNo ratings yet
- C6-L2 Privitera, M. y Lyness, J. (2007) - Depression. en Duthie Practice of Geriatrics (4a Edición) .Document3 pagesC6-L2 Privitera, M. y Lyness, J. (2007) - Depression. en Duthie Practice of Geriatrics (4a Edición) .CATALINA MALDONADO GALLEGUILLOSNo ratings yet
- Psychosocial Interventions in Complex Palliative Care Patients, Journal Reading NersDocument7 pagesPsychosocial Interventions in Complex Palliative Care Patients, Journal Reading NersSiti Malkah KamilahNo ratings yet
- Cognitive Behaviour Therapy For DepressionDocument10 pagesCognitive Behaviour Therapy For Depressiondidi monroeNo ratings yet
- Cognition in Mood DisordersDocument3 pagesCognition in Mood DisordersAndreLeonorNo ratings yet
- Psychosocial Approaches To The Treatment of Bipolar DisorderDocument10 pagesPsychosocial Approaches To The Treatment of Bipolar DisorderNera MayaditaNo ratings yet
- Holl On 2002Document39 pagesHoll On 2002Nabella Martha AnisaNo ratings yet
- Unipolar Depressive Disorders: Key PointsDocument7 pagesUnipolar Depressive Disorders: Key PointsBodat BodatsNo ratings yet
- Turkington 2006Document11 pagesTurkington 2006Aditya M.BNo ratings yet
- Pharmalogy ZADocument133 pagesPharmalogy ZASamuel KamocheNo ratings yet
- CN 19 1760Document20 pagesCN 19 1760claudia cortesNo ratings yet
- Current and Emerging Medications For Borderline Personality Disorder Is Pharmacotherapy Alone EnoughDocument16 pagesCurrent and Emerging Medications For Borderline Personality Disorder Is Pharmacotherapy Alone EnoughashtarethNo ratings yet
- Behavioral and Psychological Symptoms of Dementia: J. Cerejeira, L. Lagarto and E. B. Mukaetova-LadinskaDocument21 pagesBehavioral and Psychological Symptoms of Dementia: J. Cerejeira, L. Lagarto and E. B. Mukaetova-LadinskaPutriPasaribuNo ratings yet
- Schema Therapy Fassbinder & ArntzDocument45 pagesSchema Therapy Fassbinder & ArntzNyliam LoyolaNo ratings yet
- Diagnosis and Treatment of Cyclothymia - The "Primacy" of TemperamentDocument8 pagesDiagnosis and Treatment of Cyclothymia - The "Primacy" of Temperamentkazzman56No ratings yet
- 2302 SAMHSA Teen Guidance - FKB PDFDocument62 pages2302 SAMHSA Teen Guidance - FKB PDFPhuc ToNo ratings yet
- MhGAP Intervention Guide For MentalDocument15 pagesMhGAP Intervention Guide For Mentalmags lunaNo ratings yet
- PP + CBTDocument8 pagesPP + CBTLev FyodorNo ratings yet
- Psychoeducation For Severe Mental Illnesses Theory and Practice, Final Seminar PrintDocument22 pagesPsychoeducation For Severe Mental Illnesses Theory and Practice, Final Seminar PrintAnnPSWNo ratings yet
- Treating Somatization: A Multimodal ApproachDocument7 pagesTreating Somatization: A Multimodal ApproachDr. Ranjan KumarNo ratings yet
- Art - Depression and Somatization A Review - Part I.1982Document9 pagesArt - Depression and Somatization A Review - Part I.1982Shadia NaLaNo ratings yet
- Key Clinical Processes in Intensive Short-Term Dynamic PsychotherapyDocument5 pagesKey Clinical Processes in Intensive Short-Term Dynamic PsychotherapyVictoria AdhityaNo ratings yet
- Mood Disorder Presented by Group 8Document10 pagesMood Disorder Presented by Group 8Tanishque SinghNo ratings yet
- bmj00100 0034Document5 pagesbmj00100 0034Daria TomescuNo ratings yet
- Introduction To Dialectical Behavior Therapy For Psychiatrists and Psychiatry ResidentsDocument11 pagesIntroduction To Dialectical Behavior Therapy For Psychiatrists and Psychiatry ResidentsCarlos Hernan Castañeda RuizNo ratings yet
- The Complete Cast Crown PreparationDocument55 pagesThe Complete Cast Crown Preparationaya ahmed mohamed saadNo ratings yet
- FAMILY NURSING CARE PLAN Template With SCOREDocument1 pageFAMILY NURSING CARE PLAN Template With SCOREJanRovicNo ratings yet
- Maternal Safety Bundle For: Severe Hypertension in PregnancyDocument34 pagesMaternal Safety Bundle For: Severe Hypertension in PregnancyCarlos MayaNo ratings yet
- FHS Medical Nursing BNTDocument3 pagesFHS Medical Nursing BNTssekali stephenNo ratings yet
- PERFORMING STERILE DRESSING CHANGE IN PATIENT WHO UNDERGO EYE and EAR SURGERYDocument4 pagesPERFORMING STERILE DRESSING CHANGE IN PATIENT WHO UNDERGO EYE and EAR SURGERYPolo Gabriel MendiolaNo ratings yet
- EPTI 神NoteDocument6 pagesEPTI 神NoteChow Man HeiNo ratings yet
- Opies Cardiovascular Drugs A Companion To Braunwalds Heart Disease Expert Consult 9Th Edition Bhatt MD MPH Download PDF ChapterDocument52 pagesOpies Cardiovascular Drugs A Companion To Braunwalds Heart Disease Expert Consult 9Th Edition Bhatt MD MPH Download PDF Chaptermary.hanna173100% (4)
- Basic Education Learning Continuity Plan in The Time of COVID-19Document65 pagesBasic Education Learning Continuity Plan in The Time of COVID-19Earls jr Computer100% (1)
- Bariatric SurgeryDocument26 pagesBariatric SurgeryAmyandNo ratings yet
- Ebook 1 - The Truth About Hair LosshDocument16 pagesEbook 1 - The Truth About Hair Losshdoritosmountaindew7No ratings yet
- (Reading 5) Blood and Body Defenses-đã Chuyển ĐổiDocument18 pages(Reading 5) Blood and Body Defenses-đã Chuyển ĐổiTrúc Linh NguyễnNo ratings yet
- The Outcome of Ultrasound Guided Percutaneous Drainage of Liver AbscessDocument6 pagesThe Outcome of Ultrasound Guided Percutaneous Drainage of Liver AbscessIJAR JOURNALNo ratings yet
- Week 7 - Lecture Midterm Test RevisionDocument5 pagesWeek 7 - Lecture Midterm Test RevisionhxNo ratings yet
- Checklist Male GenitaliaDocument3 pagesChecklist Male GenitaliaJessoliver GalvezNo ratings yet
- Drug Study TemplateDocument6 pagesDrug Study TemplateReign RaineNo ratings yet
- DR HaifaDocument28 pagesDR HaifaAlex SamNo ratings yet
- Examination of AbdomenDocument67 pagesExamination of Abdomenvikram kumarNo ratings yet
- Final Guidelines For ICU Admission and Discharge Criteria 23.12.2023Document7 pagesFinal Guidelines For ICU Admission and Discharge Criteria 23.12.2023rumana.kulsum43No ratings yet
- Test Bank For Essentials of Abnormal Psychology 6th Edition DurandDocument13 pagesTest Bank For Essentials of Abnormal Psychology 6th Edition DurandHector Vossler100% (34)
- Hipotermi 9Document4 pagesHipotermi 9wahyuartyningsihNo ratings yet
- Anti InflammatoryDocument39 pagesAnti InflammatoryJosephus Vejano BlancoNo ratings yet
- DocxDocument2 pagesDocxdeepakdohare1011No ratings yet
- Apexbio Glucosure Plus ManualDocument41 pagesApexbio Glucosure Plus ManualAndreea AxinteNo ratings yet
- S17820en PDFDocument433 pagesS17820en PDFsafasayedNo ratings yet
- To Slip Inferior The Result Is A Spondylolisthesis: The Four Grades of Spondylolisthesisare As Follows: °°Document2 pagesTo Slip Inferior The Result Is A Spondylolisthesis: The Four Grades of Spondylolisthesisare As Follows: °°Katrina Vea CalaroNo ratings yet
- Standford Emergency Manual Interactive 2021Document60 pagesStandford Emergency Manual Interactive 2021reinaldo valdes iznagaNo ratings yet
- Contact Dermatitis: Dr. Hanna Jinky AbraganDocument11 pagesContact Dermatitis: Dr. Hanna Jinky AbraganAying De Barras AbraganNo ratings yet
- Pharmacology For Nursing Care 6e Test BankDocument5 pagesPharmacology For Nursing Care 6e Test BankSharon Spence100% (36)
- Chapter 8-The Clinical InterviewDocument2 pagesChapter 8-The Clinical InterviewKent67% (3)