
authorizationLetter (5)
authorizationLetter (5)
You might also like
- Tivato 700 Brochure en 30 010 0046vDocument12 pagesTivato 700 Brochure en 30 010 0046vDewan Shamsul AsifNo ratings yet
- Watson Glaser Critic Think Test-Quest PDFDocument45 pagesWatson Glaser Critic Think Test-Quest PDFSri Ram100% (2)
- Settlement Letter Details 20231121-124647Document2 pagesSettlement Letter Details 20231121-124647ajithdeepa280394No ratings yet
- 782-LS-M-001 A Equipment ListDocument2 pages782-LS-M-001 A Equipment ListSai krishnaNo ratings yet
- Philhealth Patients' Bill: Amount After DiscountDocument27 pagesPhilhealth Patients' Bill: Amount After DiscountPatricia Mae JustinianoNo ratings yet
- KH Price ListDocument135 pagesKH Price Listnikhil_fortisNo ratings yet
- EAFYA HMIS - The Future of MedicareDocument1 pageEAFYA HMIS - The Future of MedicareBigabwa BernardNo ratings yet
- Ebg-275 TH 50Document6 pagesEbg-275 TH 50Sergey ShkolyarenkoNo ratings yet
- HMW-810 T6-Technical Data - ENDocument11 pagesHMW-810 T6-Technical Data - ENjoe613410No ratings yet
- Loma CW3 Checkweigher DatasheetDocument2 pagesLoma CW3 Checkweigher DatasheetTomasNo ratings yet
- This Document Is Valid Only For Budgetary / Estimating Purpose by Company For FeedDocument5 pagesThis Document Is Valid Only For Budgetary / Estimating Purpose by Company For FeedRodrigoNo ratings yet
- CP Hutsa Rama IndonesiaDocument11 pagesCP Hutsa Rama IndonesiaDedi RosandiNo ratings yet
- Aurora: AE MD-144BD SeriesDocument2 pagesAurora: AE MD-144BD SeriesNatalia IniotakiNo ratings yet
- This Document Shall Be Used Only For Reference: Engenharia Ieept/IepsaDocument5 pagesThis Document Shall Be Used Only For Reference: Engenharia Ieept/IepsaRodrigoNo ratings yet
- Normal ChartDocument1 pageNormal ChartcsmootheyNo ratings yet
- Generator Set Data Sheet Hryw 1275 d5 6 Rental EnglishDocument6 pagesGenerator Set Data Sheet Hryw 1275 d5 6 Rental EnglishDexter BothaNo ratings yet
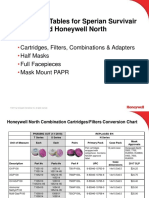
- Survivair To North APR Conversion Chart - Conversion Chart For Legacy Sperian APRDocument8 pagesSurvivair To North APR Conversion Chart - Conversion Chart For Legacy Sperian APRJuan Francisco Toledano GonzalezNo ratings yet
- OPTIR000104Document1 pageOPTIR000104Utkarsh PatilNo ratings yet
- 5.ofis W 30 Ofis WPS 18Document3 pages5.ofis W 30 Ofis WPS 18anandNo ratings yet
- HPCO2 Hose 1-2 Flexible Outlet K-81-1080 - Print - ADDocument1 pageHPCO2 Hose 1-2 Flexible Outlet K-81-1080 - Print - ADzimba marjNo ratings yet
- Img 20221210 0001Document4 pagesImg 20221210 0001prajwalkumar289No ratings yet
- 7.ofis-W-30 - Ofis-Wps-15Document3 pages7.ofis-W-30 - Ofis-Wps-15anandNo ratings yet
- Care UniteDocument6 pagesCare UniteAhmad Gamal Elden MAhanyNo ratings yet
- Foundation Plan: Paai TradersDocument1 pageFoundation Plan: Paai Tradersarnabchoudhury1987No ratings yet
- Sa8800 Compatibility Matrix: Medison Co., Ltd. Product Management DeptDocument14 pagesSa8800 Compatibility Matrix: Medison Co., Ltd. Product Management DeptNelson AltuveNo ratings yet
- PJV E7T0071.ipt: Part NumberDocument1 pagePJV E7T0071.ipt: Part NumberSaravanan KNo ratings yet
- Lemon Green H Pro 001-01 Logo TMTDocument1 pageLemon Green H Pro 001-01 Logo TMTCarlos Nolasco NolascoNo ratings yet
- Aurora: AE MD-144BD SeriesDocument2 pagesAurora: AE MD-144BD SeriesProEnergy solarNo ratings yet
- Fotoforo WelchAllynDocument10 pagesFotoforo WelchAllynDuban GuerreroNo ratings yet
- SCHEDULE OF INPATIENT TARIFF WITH EFFECTIVE FROM JayanagarDocument2 pagesSCHEDULE OF INPATIENT TARIFF WITH EFFECTIVE FROM JayanagarBOYA MOHANNo ratings yet
- Matrix 1" Nickel Three Way Ball Valve: FeaturesDocument2 pagesMatrix 1" Nickel Three Way Ball Valve: Featuresmbk appsNo ratings yet
- HDW-535 T5: Generating RatesDocument11 pagesHDW-535 T5: Generating RatesJoanCarlesLLopysNo ratings yet
- Model: GFW-100 T5Document15 pagesModel: GFW-100 T5Dhrubajyoti Bora100% (1)
- Model: HFW-200 T5Document13 pagesModel: HFW-200 T5Zaw Htet AungNo ratings yet
- Landed CostDocument17 pagesLanded Costswapnil khokeNo ratings yet
- Medical Insurance Plan - Claim: (Please Complete in Capital Letters - One Claim Per Currency)Document7 pagesMedical Insurance Plan - Claim: (Please Complete in Capital Letters - One Claim Per Currency)Denia MirandaNo ratings yet
- 3Q 36D Duri0897120240320rln01Document7 pages3Q 36D Duri0897120240320rln01bleck897No ratings yet
- This Document Shall Be Used Only For Reference: Engenharia Ieept/IepsaDocument5 pagesThis Document Shall Be Used Only For Reference: Engenharia Ieept/IepsaRodrigoNo ratings yet
- MKWD Annual Procurement Plan 2022Document55 pagesMKWD Annual Procurement Plan 2022Roland AnaumNo ratings yet
- Cessna Standard Repair ListDocument44 pagesCessna Standard Repair ListKJ Dhiman100% (1)
- Excel Engineering College (Autonomous) : Application For The End Semester Examinations - Nov / Dec - 2023Document1 pageExcel Engineering College (Autonomous) : Application For The End Semester Examinations - Nov / Dec - 2023mandalsanoj544No ratings yet
- HFW 100 T5 SoundproofDocument15 pagesHFW 100 T5 SoundproofkarimNo ratings yet
- Letter of Intent: V5 Global Services Private LimitedDocument3 pagesLetter of Intent: V5 Global Services Private LimitedRamesh ReddyNo ratings yet
- Tax Invoice, Credit and Debit Notes, E-Way Bill 01 - Class Notes - Udesh Regular - Group 1Document12 pagesTax Invoice, Credit and Debit Notes, E-Way Bill 01 - Class Notes - Udesh Regular - Group 1Uday TomarNo ratings yet
- AHU Let 2014Document2 pagesAHU Let 2014MICAH JEDAHNo ratings yet
- Excel Engineering College (Autonomous) : Application For The End Semester Examinations - May - 2023Document1 pageExcel Engineering College (Autonomous) : Application For The End Semester Examinations - May - 2023mandalsanoj544No ratings yet
- Budgeting Capital Expenditure + Operational EXPENDITURE Air AmbulanceDocument6 pagesBudgeting Capital Expenditure + Operational EXPENDITURE Air AmbulancesofyanNo ratings yet
- Tu Vung Han Han Tong HopDocument1 pageTu Vung Han Han Tong HopduyvuNo ratings yet
- PPL NPL FOSL EGB PWIS INS DSH 008 - C01 - DatasheDocument3 pagesPPL NPL FOSL EGB PWIS INS DSH 008 - C01 - DatashesegunNo ratings yet
- Schematic Diagram: Supply To Labor Accommodation For BP # M/2020/466 Abal GarareesDocument1 pageSchematic Diagram: Supply To Labor Accommodation For BP # M/2020/466 Abal GarareesAnsaf AskyNo ratings yet
- CEEE - Transformadores - SEs - Simplificadas Ago17Document54 pagesCEEE - Transformadores - SEs - Simplificadas Ago17rodineicarraroNo ratings yet
- Cepha Products - API RequirementDocument1 pageCepha Products - API RequirementRAJEEV GIRINo ratings yet
- FLW00008 - Ipd Cycle With Accounting Effect 2Document1 pageFLW00008 - Ipd Cycle With Accounting Effect 2Rafael SampayanNo ratings yet
- 110004774-10 170KV 630dia 1T With CK BaseDocument5 pages110004774-10 170KV 630dia 1T With CK Basetragi oyeNo ratings yet
- C10RL 3 in 1 Color Doppler UltrasoundDocument4 pagesC10RL 3 in 1 Color Doppler UltrasoundLuis Barba DíazNo ratings yet
- General: Part Number: Status: Overview: DescriptionDocument3 pagesGeneral: Part Number: Status: Overview: Descriptionfogok72408No ratings yet
- Mete R: AE CMD-144BDS SeriesDocument2 pagesMete R: AE CMD-144BDS SeriesWyn Power CorpNo ratings yet
- SPZ6000 Schematic NewDocument1 pageSPZ6000 Schematic Newavrata79No ratings yet
- Self Declaration 2022-23 DyEEDocument1 pageSelf Declaration 2022-23 DyEEprakash reddyNo ratings yet
- (Op Buffer Installation) K 601125Document3 pages(Op Buffer Installation) K 601125Ali DiabNo ratings yet
- Study of Hul and ItcDocument10 pagesStudy of Hul and ItcDark SideNo ratings yet
- Amazon ClothingBillDocument2 pagesAmazon ClothingBillSantosh KumarNo ratings yet
- Zong PresentationDocument13 pagesZong Presentationadnan aamirNo ratings yet
- Himachal Pradesh Rights of Persons With Disabilities Rules, 2019Document42 pagesHimachal Pradesh Rights of Persons With Disabilities Rules, 2019Disability Rights AllianceNo ratings yet
- HickelDocument2 pagesHickelYvonne Carol80% (10)
- Entertainment Industry in IndiaDocument23 pagesEntertainment Industry in IndiaAnjali MishraNo ratings yet
- Tra Confirmation Page 1601eq DecemberDocument1 pageTra Confirmation Page 1601eq Decembernaim indahiNo ratings yet
- Memory QVL For AMD Ryzen 2000 Series Processors PDFDocument21 pagesMemory QVL For AMD Ryzen 2000 Series Processors PDFChris OrtizNo ratings yet
- Do Not Scale: DescriptionDocument6 pagesDo Not Scale: DescriptionPalyyNo ratings yet
- Gizmoz Study CaseDocument4 pagesGizmoz Study CaseInge Monica100% (1)
- Blanding - Westwater Work Session 12-1-09Document2 pagesBlanding - Westwater Work Session 12-1-09Bill KeshlearNo ratings yet
- Simple Interest Worksheet - Maryam FDocument4 pagesSimple Interest Worksheet - Maryam Fapi-464088459No ratings yet
- Amazone CayrosDocument24 pagesAmazone CayrosAnonymous 1XBCMXNo ratings yet
- Directions - (Q. 6-10) Given An Input Line A Machine Generates Passcodes Step by Step FollowingDocument25 pagesDirections - (Q. 6-10) Given An Input Line A Machine Generates Passcodes Step by Step Followinganandhivimala100% (1)
- Thrift by Smiles, Samuel, 1812-1904Document224 pagesThrift by Smiles, Samuel, 1812-1904Gutenberg.orgNo ratings yet
- Channels of DistributionDocument6 pagesChannels of DistributionLakshmi KrishnaswamyNo ratings yet
- E Ticket Ticketed: Passenger Name Ticket Number Frequent Flyer NoDocument1 pageE Ticket Ticketed: Passenger Name Ticket Number Frequent Flyer NoAshapdeep SinghNo ratings yet
- Invoice Geyser 2Document2 pagesInvoice Geyser 2archisman gayenNo ratings yet
- Case Analysis Chapter 6 VF Brands GlobalDocument5 pagesCase Analysis Chapter 6 VF Brands GlobalNimah Saeed25% (4)
- Activity Report:: Water AuditDocument12 pagesActivity Report:: Water AuditYuvaneswari ParameswaranNo ratings yet
- Goals of Financial ManagementDocument22 pagesGoals of Financial ManagementBhuvanNo ratings yet
- 5G Tower Suburb List August 2019Document10 pages5G Tower Suburb List August 2019Ken Murray0% (2)
- Save The Planet Lesson PlanDocument5 pagesSave The Planet Lesson PlanJessica NicerioNo ratings yet
- ASSIGNMENT3Document2 pagesASSIGNMENT3SandeepNo ratings yet
- Tetra PakDocument5 pagesTetra PakRichardson Holder0% (1)
- India Global LeaderDocument48 pagesIndia Global Leaderhusankar2103No ratings yet
- Devina Singh - EDPM 2023 Assignment 2Document11 pagesDevina Singh - EDPM 2023 Assignment 2Devina SinghNo ratings yet
- Ibrd, Ida, Ifc NotesDocument10 pagesIbrd, Ida, Ifc NotesvmktptNo ratings yet
- Project Profile FoundryDocument12 pagesProject Profile FoundryAkshay VarmaNo ratings yet




















































































Download as pdf or txt
You might also like
- Tivato 700 Brochure en 30 010 0046vDocument12 pagesTivato 700 Brochure en 30 010 0046vDewan Shamsul AsifNo ratings yet
- Watson Glaser Critic Think Test-Quest PDFDocument45 pagesWatson Glaser Critic Think Test-Quest PDFSri Ram100% (2)
- Settlement Letter Details 20231121-124647Document2 pagesSettlement Letter Details 20231121-124647ajithdeepa280394No ratings yet
- 782-LS-M-001 A Equipment ListDocument2 pages782-LS-M-001 A Equipment ListSai krishnaNo ratings yet
- Philhealth Patients' Bill: Amount After DiscountDocument27 pagesPhilhealth Patients' Bill: Amount After DiscountPatricia Mae JustinianoNo ratings yet
- KH Price ListDocument135 pagesKH Price Listnikhil_fortisNo ratings yet
- EAFYA HMIS - The Future of MedicareDocument1 pageEAFYA HMIS - The Future of MedicareBigabwa BernardNo ratings yet
- Ebg-275 TH 50Document6 pagesEbg-275 TH 50Sergey ShkolyarenkoNo ratings yet
- HMW-810 T6-Technical Data - ENDocument11 pagesHMW-810 T6-Technical Data - ENjoe613410No ratings yet
- Loma CW3 Checkweigher DatasheetDocument2 pagesLoma CW3 Checkweigher DatasheetTomasNo ratings yet
- This Document Is Valid Only For Budgetary / Estimating Purpose by Company For FeedDocument5 pagesThis Document Is Valid Only For Budgetary / Estimating Purpose by Company For FeedRodrigoNo ratings yet
- CP Hutsa Rama IndonesiaDocument11 pagesCP Hutsa Rama IndonesiaDedi RosandiNo ratings yet
- Aurora: AE MD-144BD SeriesDocument2 pagesAurora: AE MD-144BD SeriesNatalia IniotakiNo ratings yet
- This Document Shall Be Used Only For Reference: Engenharia Ieept/IepsaDocument5 pagesThis Document Shall Be Used Only For Reference: Engenharia Ieept/IepsaRodrigoNo ratings yet
- Normal ChartDocument1 pageNormal ChartcsmootheyNo ratings yet
- Generator Set Data Sheet Hryw 1275 d5 6 Rental EnglishDocument6 pagesGenerator Set Data Sheet Hryw 1275 d5 6 Rental EnglishDexter BothaNo ratings yet
- Survivair To North APR Conversion Chart - Conversion Chart For Legacy Sperian APRDocument8 pagesSurvivair To North APR Conversion Chart - Conversion Chart For Legacy Sperian APRJuan Francisco Toledano GonzalezNo ratings yet
- OPTIR000104Document1 pageOPTIR000104Utkarsh PatilNo ratings yet
- 5.ofis W 30 Ofis WPS 18Document3 pages5.ofis W 30 Ofis WPS 18anandNo ratings yet
- HPCO2 Hose 1-2 Flexible Outlet K-81-1080 - Print - ADDocument1 pageHPCO2 Hose 1-2 Flexible Outlet K-81-1080 - Print - ADzimba marjNo ratings yet
- Img 20221210 0001Document4 pagesImg 20221210 0001prajwalkumar289No ratings yet
- 7.ofis-W-30 - Ofis-Wps-15Document3 pages7.ofis-W-30 - Ofis-Wps-15anandNo ratings yet
- Care UniteDocument6 pagesCare UniteAhmad Gamal Elden MAhanyNo ratings yet
- Foundation Plan: Paai TradersDocument1 pageFoundation Plan: Paai Tradersarnabchoudhury1987No ratings yet
- Sa8800 Compatibility Matrix: Medison Co., Ltd. Product Management DeptDocument14 pagesSa8800 Compatibility Matrix: Medison Co., Ltd. Product Management DeptNelson AltuveNo ratings yet
- PJV E7T0071.ipt: Part NumberDocument1 pagePJV E7T0071.ipt: Part NumberSaravanan KNo ratings yet
- Lemon Green H Pro 001-01 Logo TMTDocument1 pageLemon Green H Pro 001-01 Logo TMTCarlos Nolasco NolascoNo ratings yet
- Aurora: AE MD-144BD SeriesDocument2 pagesAurora: AE MD-144BD SeriesProEnergy solarNo ratings yet
- Fotoforo WelchAllynDocument10 pagesFotoforo WelchAllynDuban GuerreroNo ratings yet
- SCHEDULE OF INPATIENT TARIFF WITH EFFECTIVE FROM JayanagarDocument2 pagesSCHEDULE OF INPATIENT TARIFF WITH EFFECTIVE FROM JayanagarBOYA MOHANNo ratings yet
- Matrix 1" Nickel Three Way Ball Valve: FeaturesDocument2 pagesMatrix 1" Nickel Three Way Ball Valve: Featuresmbk appsNo ratings yet
- HDW-535 T5: Generating RatesDocument11 pagesHDW-535 T5: Generating RatesJoanCarlesLLopysNo ratings yet
- Model: GFW-100 T5Document15 pagesModel: GFW-100 T5Dhrubajyoti Bora100% (1)
- Model: HFW-200 T5Document13 pagesModel: HFW-200 T5Zaw Htet AungNo ratings yet
- Landed CostDocument17 pagesLanded Costswapnil khokeNo ratings yet
- Medical Insurance Plan - Claim: (Please Complete in Capital Letters - One Claim Per Currency)Document7 pagesMedical Insurance Plan - Claim: (Please Complete in Capital Letters - One Claim Per Currency)Denia MirandaNo ratings yet
- 3Q 36D Duri0897120240320rln01Document7 pages3Q 36D Duri0897120240320rln01bleck897No ratings yet
- This Document Shall Be Used Only For Reference: Engenharia Ieept/IepsaDocument5 pagesThis Document Shall Be Used Only For Reference: Engenharia Ieept/IepsaRodrigoNo ratings yet
- MKWD Annual Procurement Plan 2022Document55 pagesMKWD Annual Procurement Plan 2022Roland AnaumNo ratings yet
- Cessna Standard Repair ListDocument44 pagesCessna Standard Repair ListKJ Dhiman100% (1)
- Excel Engineering College (Autonomous) : Application For The End Semester Examinations - Nov / Dec - 2023Document1 pageExcel Engineering College (Autonomous) : Application For The End Semester Examinations - Nov / Dec - 2023mandalsanoj544No ratings yet
- HFW 100 T5 SoundproofDocument15 pagesHFW 100 T5 SoundproofkarimNo ratings yet
- Letter of Intent: V5 Global Services Private LimitedDocument3 pagesLetter of Intent: V5 Global Services Private LimitedRamesh ReddyNo ratings yet
- Tax Invoice, Credit and Debit Notes, E-Way Bill 01 - Class Notes - Udesh Regular - Group 1Document12 pagesTax Invoice, Credit and Debit Notes, E-Way Bill 01 - Class Notes - Udesh Regular - Group 1Uday TomarNo ratings yet
- AHU Let 2014Document2 pagesAHU Let 2014MICAH JEDAHNo ratings yet
- Excel Engineering College (Autonomous) : Application For The End Semester Examinations - May - 2023Document1 pageExcel Engineering College (Autonomous) : Application For The End Semester Examinations - May - 2023mandalsanoj544No ratings yet
- Budgeting Capital Expenditure + Operational EXPENDITURE Air AmbulanceDocument6 pagesBudgeting Capital Expenditure + Operational EXPENDITURE Air AmbulancesofyanNo ratings yet
- Tu Vung Han Han Tong HopDocument1 pageTu Vung Han Han Tong HopduyvuNo ratings yet
- PPL NPL FOSL EGB PWIS INS DSH 008 - C01 - DatasheDocument3 pagesPPL NPL FOSL EGB PWIS INS DSH 008 - C01 - DatashesegunNo ratings yet
- Schematic Diagram: Supply To Labor Accommodation For BP # M/2020/466 Abal GarareesDocument1 pageSchematic Diagram: Supply To Labor Accommodation For BP # M/2020/466 Abal GarareesAnsaf AskyNo ratings yet
- CEEE - Transformadores - SEs - Simplificadas Ago17Document54 pagesCEEE - Transformadores - SEs - Simplificadas Ago17rodineicarraroNo ratings yet
- Cepha Products - API RequirementDocument1 pageCepha Products - API RequirementRAJEEV GIRINo ratings yet
- FLW00008 - Ipd Cycle With Accounting Effect 2Document1 pageFLW00008 - Ipd Cycle With Accounting Effect 2Rafael SampayanNo ratings yet
- 110004774-10 170KV 630dia 1T With CK BaseDocument5 pages110004774-10 170KV 630dia 1T With CK Basetragi oyeNo ratings yet
- C10RL 3 in 1 Color Doppler UltrasoundDocument4 pagesC10RL 3 in 1 Color Doppler UltrasoundLuis Barba DíazNo ratings yet
- General: Part Number: Status: Overview: DescriptionDocument3 pagesGeneral: Part Number: Status: Overview: Descriptionfogok72408No ratings yet
- Mete R: AE CMD-144BDS SeriesDocument2 pagesMete R: AE CMD-144BDS SeriesWyn Power CorpNo ratings yet
- SPZ6000 Schematic NewDocument1 pageSPZ6000 Schematic Newavrata79No ratings yet
- Self Declaration 2022-23 DyEEDocument1 pageSelf Declaration 2022-23 DyEEprakash reddyNo ratings yet
- (Op Buffer Installation) K 601125Document3 pages(Op Buffer Installation) K 601125Ali DiabNo ratings yet
- Study of Hul and ItcDocument10 pagesStudy of Hul and ItcDark SideNo ratings yet
- Amazon ClothingBillDocument2 pagesAmazon ClothingBillSantosh KumarNo ratings yet
- Zong PresentationDocument13 pagesZong Presentationadnan aamirNo ratings yet
- Himachal Pradesh Rights of Persons With Disabilities Rules, 2019Document42 pagesHimachal Pradesh Rights of Persons With Disabilities Rules, 2019Disability Rights AllianceNo ratings yet
- HickelDocument2 pagesHickelYvonne Carol80% (10)
- Entertainment Industry in IndiaDocument23 pagesEntertainment Industry in IndiaAnjali MishraNo ratings yet
- Tra Confirmation Page 1601eq DecemberDocument1 pageTra Confirmation Page 1601eq Decembernaim indahiNo ratings yet
- Memory QVL For AMD Ryzen 2000 Series Processors PDFDocument21 pagesMemory QVL For AMD Ryzen 2000 Series Processors PDFChris OrtizNo ratings yet
- Do Not Scale: DescriptionDocument6 pagesDo Not Scale: DescriptionPalyyNo ratings yet
- Gizmoz Study CaseDocument4 pagesGizmoz Study CaseInge Monica100% (1)
- Blanding - Westwater Work Session 12-1-09Document2 pagesBlanding - Westwater Work Session 12-1-09Bill KeshlearNo ratings yet
- Simple Interest Worksheet - Maryam FDocument4 pagesSimple Interest Worksheet - Maryam Fapi-464088459No ratings yet
- Amazone CayrosDocument24 pagesAmazone CayrosAnonymous 1XBCMXNo ratings yet
- Directions - (Q. 6-10) Given An Input Line A Machine Generates Passcodes Step by Step FollowingDocument25 pagesDirections - (Q. 6-10) Given An Input Line A Machine Generates Passcodes Step by Step Followinganandhivimala100% (1)
- Thrift by Smiles, Samuel, 1812-1904Document224 pagesThrift by Smiles, Samuel, 1812-1904Gutenberg.orgNo ratings yet
- Channels of DistributionDocument6 pagesChannels of DistributionLakshmi KrishnaswamyNo ratings yet
- E Ticket Ticketed: Passenger Name Ticket Number Frequent Flyer NoDocument1 pageE Ticket Ticketed: Passenger Name Ticket Number Frequent Flyer NoAshapdeep SinghNo ratings yet
- Invoice Geyser 2Document2 pagesInvoice Geyser 2archisman gayenNo ratings yet
- Case Analysis Chapter 6 VF Brands GlobalDocument5 pagesCase Analysis Chapter 6 VF Brands GlobalNimah Saeed25% (4)
- Activity Report:: Water AuditDocument12 pagesActivity Report:: Water AuditYuvaneswari ParameswaranNo ratings yet
- Goals of Financial ManagementDocument22 pagesGoals of Financial ManagementBhuvanNo ratings yet
- 5G Tower Suburb List August 2019Document10 pages5G Tower Suburb List August 2019Ken Murray0% (2)
- Save The Planet Lesson PlanDocument5 pagesSave The Planet Lesson PlanJessica NicerioNo ratings yet
- ASSIGNMENT3Document2 pagesASSIGNMENT3SandeepNo ratings yet
- Tetra PakDocument5 pagesTetra PakRichardson Holder0% (1)
- India Global LeaderDocument48 pagesIndia Global Leaderhusankar2103No ratings yet
- Devina Singh - EDPM 2023 Assignment 2Document11 pagesDevina Singh - EDPM 2023 Assignment 2Devina SinghNo ratings yet
- Ibrd, Ida, Ifc NotesDocument10 pagesIbrd, Ida, Ifc NotesvmktptNo ratings yet
- Project Profile FoundryDocument12 pagesProject Profile FoundryAkshay VarmaNo ratings yet