Download as pdf or txt
You might also like
- MKS Instruments Level3 56PKGJFGB Aug19Document7 pagesMKS Instruments Level3 56PKGJFGB Aug19Shrikant Mande0% (1)
- SOA-0000000001180nnbbs87 - 1680000202603 - ITEMIZED (1) - UnlockedDocument3 pagesSOA-0000000001180nnbbs87 - 1680000202603 - ITEMIZED (1) - UnlockedWarren David SabarezNo ratings yet
- Your Business Advantage Fundamentals™ Banking: Account SummaryDocument56 pagesYour Business Advantage Fundamentals™ Banking: Account SummaryJuan Koci100% (4)
- Your Business Advantage Relationship Banking: Account SummaryDocument4 pagesYour Business Advantage Relationship Banking: Account SummaryJasmine ONeill50% (2)
- EI Fund Transfer Intnl TT Form V3.0 PDFDocument1 pageEI Fund Transfer Intnl TT Form V3.0 PDFMbamali ChukwunenyeNo ratings yet
- The AMS 0% Interest Payment Plan Agreement: David Hegi JRDocument1 pageThe AMS 0% Interest Payment Plan Agreement: David Hegi JRUnscripted MediaNo ratings yet
- OAG Replacement Sprint ApprovalDocument4 pagesOAG Replacement Sprint ApprovalDAVID JUDRELNo ratings yet
- BLM California 2020 RegistrationDocument17 pagesBLM California 2020 RegistrationWashington ExaminerNo ratings yet
- March BOA Statement 2 PDF 2Document6 pagesMarch BOA Statement 2 PDF 2mdyafi8084No ratings yet
- Miss Silandiso Ndwandwe 212 Kitchener Ave Kensington Johannesburg 2094Document1 pageMiss Silandiso Ndwandwe 212 Kitchener Ave Kensington Johannesburg 2094silandisoaNo ratings yet
- Monthly StatementDocument2 pagesMonthly StatementYuniioor UrbaezNo ratings yet
- Yates Logistics BofA SepDocument7 pagesYates Logistics BofA SepJonathan Seagull LivingstonNo ratings yet
- APRIL-BOA-Statement-2-pdf - 1Document6 pagesAPRIL-BOA-Statement-2-pdf - 1nurulamin00023No ratings yet
- March-BOA-Statement-2-pdf - 2Document6 pagesMarch-BOA-Statement-2-pdf - 2mdyafi8084No ratings yet
- 5.invoice INV-4745Document4 pages5.invoice INV-4745Raheel KaziNo ratings yet
- Estmt - 2024 04 30Document4 pagesEstmt - 2024 04 30elidiafloresNo ratings yet
- Computation 2019Document16 pagesComputation 2019Giri SukumarNo ratings yet
- Terp Asia Construction Corp.: Statement of AccountDocument4 pagesTerp Asia Construction Corp.: Statement of AccountMark Israel DirectoNo ratings yet
- Statement of Account: Summary of Charges and CreditsDocument3 pagesStatement of Account: Summary of Charges and CreditsRonnel TattaoNo ratings yet
- Statement (2) BackupDocument3 pagesStatement (2) BackupgarrettloehrNo ratings yet
- 4_5929218436780528536 (1)Document6 pages4_5929218436780528536 (1)mdyafi8084No ratings yet
- StatementDocument2 pagesStatementgarrettloehrNo ratings yet
- Wells Fargo 200Document5 pagesWells Fargo 200sam ujuNo ratings yet
- Income Tax - Computation - 2021Document26 pagesIncome Tax - Computation - 2021umasankarNo ratings yet
- H One (PVT) LTD 20-21-ExemptDocument164 pagesH One (PVT) LTD 20-21-ExemptShehara GamlathNo ratings yet
- Invoice: Swifserv Customer Services Co. # INV-000020Document1 pageInvoice: Swifserv Customer Services Co. # INV-000020ginaNo ratings yet
- Statement (1) BackupDocument3 pagesStatement (1) Backupgarrettloehr100% (1)
- Welcome To Rogers: Vishn VardhanDocument8 pagesWelcome To Rogers: Vishn Vardhanvaceslavokov100% (1)
- 1242395_20220717001950_computation_2022Document16 pages1242395_20220717001950_computation_2022Jagbandhu MaharanaNo ratings yet
- 2024 01 19 - StatementDocument2 pages2024 01 19 - StatementjanmejaychhetriNo ratings yet
- EAFS009635608ITRTY122021Document9 pagesEAFS009635608ITRTY122021Kevin BesaNo ratings yet
- 2024 March As BLandCAAndrewsDocument3 pages2024 March As BLandCAAndrewsmoora7428No ratings yet
- eFPS Payment DetailsDocument3 pageseFPS Payment DetailsPoofNo ratings yet
- Summary of Current Charges Amount (RS.) : Bill Enquiries: 3033 7777 or 377Document4 pagesSummary of Current Charges Amount (RS.) : Bill Enquiries: 3033 7777 or 377far03No ratings yet
- Lgu-Sta. Lucia (August)Document4 pagesLgu-Sta. Lucia (August)Ldrrmo SantaluciailocossurNo ratings yet
- Soa 0000000005216528Document3 pagesSoa 0000000005216528libantinocedrick07No ratings yet
- 3085Document3 pages3085valorantsid00No ratings yet
- Converge Soa - FebDocument3 pagesConverge Soa - Feb64c3612ef4e13f192f009df1No ratings yet
- Soa 0000000007093223Document3 pagesSoa 0000000007093223daisy.gatewaygroupNo ratings yet
- Disbursement Voucher: Mode of Payment Payee AddressDocument5 pagesDisbursement Voucher: Mode of Payment Payee AddressDENNIS SAGUIDNo ratings yet
- SOA Nov Dec2021Document3 pagesSOA Nov Dec2021Don James VillaroNo ratings yet
- Statement of Account: Summary of Charges and CreditsDocument4 pagesStatement of Account: Summary of Charges and CreditsRitchelle Quijote DelgadoNo ratings yet
- Your Reliance Communications Bill: Summary of Current Charges Amount (RS)Document3 pagesYour Reliance Communications Bill: Summary of Current Charges Amount (RS)Dhamotharan ChinnaduraiNo ratings yet
- Lalakay Elementary School: Statement of AccountDocument4 pagesLalakay Elementary School: Statement of AccountERVIN REYESNo ratings yet
- Your Reliance Bill: Summary of Current Charges Amount (RS)Document3 pagesYour Reliance Bill: Summary of Current Charges Amount (RS)shimmmNo ratings yet
- Telus 40042789 2023 03 25Document10 pagesTelus 40042789 2023 03 25Harold KumarNo ratings yet
- Shaheed Taylor 2223 Florey LN Apt. E8 ROSLYN PA 19001: Return Service RequestedDocument3 pagesShaheed Taylor 2223 Florey LN Apt. E8 ROSLYN PA 19001: Return Service Requestedshaheed taylorNo ratings yet
- Soa-000000009005519 1680000326888Document3 pagesSoa-000000009005519 1680000326888Jan R.No ratings yet
- Soa Oct2023Document1 pageSoa Oct2023Anasterio AngchangcoNo ratings yet
- 3106Document4 pages3106valorantsid00No ratings yet
- Your Consolidated Statement: Contact UsDocument4 pagesYour Consolidated Statement: Contact UsBraeylnn bookerNo ratings yet
- Intertech Fluid Power 2019Document38 pagesIntertech Fluid Power 2019Sue StevenNo ratings yet
- FBR CST Assign Contractor 22 Feb 2024Document1 pageFBR CST Assign Contractor 22 Feb 2024Syed TabishNo ratings yet
- SOA-0000000012348926Document3 pagesSOA-0000000012348926Esmedinna CabillagasNo ratings yet
- Invoice: Venture Accounting Pte LTD # VA211344Document2 pagesInvoice: Venture Accounting Pte LTD # VA211344isty5nntNo ratings yet
- Payment Coupon: Contact Information Programs You Are Enrolled inDocument2 pagesPayment Coupon: Contact Information Programs You Are Enrolled inCarl BlackNo ratings yet
- July 2020 - ACCTG CEP 24362280Document2 pagesJuly 2020 - ACCTG CEP 24362280Jayson Berja de LeonNo ratings yet
- New May - 2022-05-31Document8 pagesNew May - 2022-05-3176xzv4kk5vNo ratings yet
- PNC Statement 2023-10-04Document1 pagePNC Statement 2023-10-04jennymark8866No ratings yet
- Invoice Newgate ChurchDocument2 pagesInvoice Newgate Churchhighpacific71No ratings yet
- M/s ABC Trust: BALANCE SHEET As On 31-03-2022Document2 pagesM/s ABC Trust: BALANCE SHEET As On 31-03-2022chiku vermaNo ratings yet
- J.K. Lasser's Small Business Taxes 2021: Your Complete Guide to a Better Bottom LineFrom EverandJ.K. Lasser's Small Business Taxes 2021: Your Complete Guide to a Better Bottom LineNo ratings yet
- Indra-QUO-01013-C7P9V6Document1 pageIndra-QUO-01013-C7P9V6juneduval680No ratings yet
- 1529675i47i6uktfuDocument6 pages1529675i47i6uktfujuneduval680No ratings yet
- 2;oqUFHQEOHIFQe;iofhqe;uveuDocument3 pages2;oqUFHQEOHIFQe;iofhqe;uveujuneduval680No ratings yet
- aejrgiyrlwhirDocument6 pagesaejrgiyrlwhirjuneduval680No ratings yet
- OW;RUGHRUOIDocument4 pagesOW;RUGHRUOIjuneduval680No ratings yet
- 130QEULIetfgIWEGLelwicDocument2 pages130QEULIetfgIWEGLelwicjuneduval680No ratings yet
- Aktiviteti I LlogariseDocument1 pageAktiviteti I LlogariseElion MitroNo ratings yet
- INCOME TAXATION SyllabusDocument7 pagesINCOME TAXATION SyllabusmarkbagzNo ratings yet
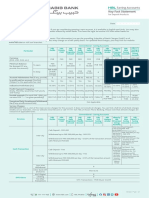
- KFS HBL Conventional Saving Account-SeptemberDocument6 pagesKFS HBL Conventional Saving Account-Septembermaya aliNo ratings yet
- Profel1 AC Activity Assets Part1Document2 pagesProfel1 AC Activity Assets Part1Dizon Ropalito P.No ratings yet
- Salary, Wage, Income: Business MathematicsDocument20 pagesSalary, Wage, Income: Business MathematicsNatasha Dela PeñaNo ratings yet
- C.T.A. Case Nos. 7246 & 7293 - Ateneo de Manila UniversityDocument13 pagesC.T.A. Case Nos. 7246 & 7293 - Ateneo de Manila UniversityFirenze PHNo ratings yet
- C6 - Investment IncentivesDocument26 pagesC6 - Investment Incentivesnabilah natashaNo ratings yet
- Direct Tax Summary NotesDocument88 pagesDirect Tax Summary NotesAlisha LukeNo ratings yet
- Pure VPN Mixed HitDocument8 pagesPure VPN Mixed Hitu9640688No ratings yet
- 2022-23 - Nilgiri School FeesDocument1 page2022-23 - Nilgiri School Feesd_tantubaiNo ratings yet
- Order Types in SAPDocument88 pagesOrder Types in SAPRamesh MNo ratings yet
- Form GST RFD - 11Document3 pagesForm GST RFD - 11Aadarsh KumarNo ratings yet
- January 2024Document8 pagesJanuary 2024Andre BarrazaNo ratings yet
- Make My Trip ICICI Bank Cobranded Credit CardDocument20 pagesMake My Trip ICICI Bank Cobranded Credit Cardprnkagarwal4166No ratings yet
- Grant of PurchaseDocument5 pagesGrant of Purchaseganeshsonone009No ratings yet
- Vishal Project Plastic MoneyDocument25 pagesVishal Project Plastic Moneyharjinder pal singh100% (2)
- AGT-2003999 Lahore Graduate Engineers Training Program Any PlantDocument3 pagesAGT-2003999 Lahore Graduate Engineers Training Program Any PlantHukmran HussainNo ratings yet
- C008 - Shaan Admark Consultant Pvt. L PDFDocument2 pagesC008 - Shaan Admark Consultant Pvt. L PDFAnonymous DWwJfrFLINo ratings yet
- Acc Statement 1120566636663 2023-10-01 2023-10-31 20231215111413Document1 pageAcc Statement 1120566636663 2023-10-01 2023-10-31 20231215111413Agung MaharNo ratings yet
- Sahibandhu FBSpends Oct'23Document1 pageSahibandhu FBSpends Oct'23gaurav sondhiNo ratings yet
- Acct Statement XX2242 23022024Document36 pagesAcct Statement XX2242 23022024Rohan SJNo ratings yet
- 2014e PDFDocument64 pages2014e PDFHenryNo ratings yet
- Tax (Zero Rated Transactions)Document4 pagesTax (Zero Rated Transactions)QuinxNo ratings yet
- Internet Bill MayDocument1 pageInternet Bill MayWasim SayyedNo ratings yet
- Excise DutyDocument12 pagesExcise DutyshreeMaliNo ratings yet
- Chapter 04 Deductions From Gross EstateDocument19 pagesChapter 04 Deductions From Gross EstateNikki Bucatcat0% (1)
- KL2032058130 OF1110 16-Dec-2019Document10 pagesKL2032058130 OF1110 16-Dec-2019Samsung KumarNo ratings yet