Download as pdf or txt
You might also like
- Management of Post Facial Paralysis Synkinesis 1St Edition Babak Azizzadeh MD Facs Full ChapterDocument67 pagesManagement of Post Facial Paralysis Synkinesis 1St Edition Babak Azizzadeh MD Facs Full Chaptercatherine.green419100% (6)
- Chapter 35 Health PhysicsDocument10 pagesChapter 35 Health PhysicsMegNo ratings yet
- 2 SinovialsarcomaDocument6 pages2 Sinovialsarcomacindy315No ratings yet
- Tumores OdontogenicosDocument8 pagesTumores OdontogenicosMeditador OficialNo ratings yet
- Primary Desmoplastic Small-Round-Cell Tumor of The Ovary: Casereports Open AccessDocument4 pagesPrimary Desmoplastic Small-Round-Cell Tumor of The Ovary: Casereports Open AccessNehemias MD GuevaraNo ratings yet
- Melanocytic Lesions of The ConjunctivaDocument8 pagesMelanocytic Lesions of The ConjunctivaR.m. IrsanNo ratings yet
- Follicular Dendritic Cell Sarcoma of The Tonssilar About A CaseDocument4 pagesFollicular Dendritic Cell Sarcoma of The Tonssilar About A CaseInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Traditional Serrated Adenoma - Libre PathologyDocument3 pagesTraditional Serrated Adenoma - Libre PathologyfadoNo ratings yet
- Hennessey 2013Document4 pagesHennessey 2013FarihinternaNo ratings yet
- Spectrum of FDG Uptake in Large ( 10 CM) Esophageal LeiomyomasDocument4 pagesSpectrum of FDG Uptake in Large ( 10 CM) Esophageal LeiomyomasYacine Tarik AizelNo ratings yet
- Update On Nasopharyngeal Carcinoma: Ó Humana 2007Document6 pagesUpdate On Nasopharyngeal Carcinoma: Ó Humana 2007Zakia AjaNo ratings yet
- Alveolar Soft Part SarcomaDocument20 pagesAlveolar Soft Part SarcomaAffan Akbar TalamiNo ratings yet
- ArticuloDocument9 pagesArticuloGabriel Pachas AlvaradoNo ratings yet
- Reconstruction of Groin Defects Following Radical Inguinal Lymphadenectomy: An Evidence Based ReviewDocument9 pagesReconstruction of Groin Defects Following Radical Inguinal Lymphadenectomy: An Evidence Based ReviewamdreyNo ratings yet
- Adenoma Colonoscopy JournalDocument8 pagesAdenoma Colonoscopy JournalHesaNo ratings yet
- Cytological Diagnostic Features of Late Breast Implant Seromas: From Reactive To Anaplastic Large Cell LymphomaDocument20 pagesCytological Diagnostic Features of Late Breast Implant Seromas: From Reactive To Anaplastic Large Cell Lymphomajhon vNo ratings yet
- Rakovich Solitary Fibrous Tumour of The Pleura A Case Report 2010Document2 pagesRakovich Solitary Fibrous Tumour of The Pleura A Case Report 2010JZNo ratings yet
- Modpathol 201792 ADocument11 pagesModpathol 201792 AMariana UsatiiNo ratings yet
- Secondary Orbital MlanomasDocument5 pagesSecondary Orbital MlanomaskarmayagnaNo ratings yet
- Vitellointestinal Duct Anomalies in InfancyDocument3 pagesVitellointestinal Duct Anomalies in InfancyRonjavafantillanNo ratings yet
- Odontogenic Malignancies: Lee J. Slater, DDS, MSDocument16 pagesOdontogenic Malignancies: Lee J. Slater, DDS, MSlaljadeff12No ratings yet
- Omental RhabdoDocument4 pagesOmental RhabdoDaisuke KiritoNo ratings yet
- Medular PseudoangiosarcomaDocument5 pagesMedular PseudoangiosarcomaUriel Benito Cabañas RodriguezNo ratings yet
- Adenocarcinoma of The Urinary Bladder: Resident Short ReviewsDocument5 pagesAdenocarcinoma of The Urinary Bladder: Resident Short ReviewserikafebriyanarNo ratings yet
- Persistent Cloaca Persistence of The ChallengeDocument7 pagesPersistent Cloaca Persistence of The ChallengekaremiaNo ratings yet
- Pleomorphic Adenoma of A Minor Salivary Gland-Report of A CaseDocument3 pagesPleomorphic Adenoma of A Minor Salivary Gland-Report of A CasePriya BabyNo ratings yet
- Milan System1Document4 pagesMilan System1ixNo ratings yet
- Articulo 1Document7 pagesArticulo 1Mariuxi CastroNo ratings yet
- Management of The Colonic Volvulus in 2016Document10 pagesManagement of The Colonic Volvulus in 2016alexandraNo ratings yet
- Davanzo Solitary Fibrous Tumor 2018Document9 pagesDavanzo Solitary Fibrous Tumor 2018JZNo ratings yet
- 2019 Histo SubtypeDocument8 pages2019 Histo SubtypemaomaochongNo ratings yet
- nagao2001Document7 pagesnagao2001FernandNo ratings yet
- Pólipos GástricosDocument8 pagesPólipos GástricosRonnie Reyes MartínezNo ratings yet
- Synovial SarcomaDocument24 pagesSynovial SarcomaKezia PaneNo ratings yet
- AmeloblastomaDocument4 pagesAmeloblastomaMarïsa CastellonNo ratings yet
- Extradigital Symplastic Glomus Tumor of The Hand: Report of 2 Cases and Literature ReviewDocument3 pagesExtradigital Symplastic Glomus Tumor of The Hand: Report of 2 Cases and Literature ReviewGabriela Serra del CarpioNo ratings yet
- Git ArticleDocument6 pagesGit ArticlePawan SapkotaNo ratings yet
- RG 256055137Document20 pagesRG 256055137Adel SalehNo ratings yet
- World Journal of Surgical OncologyDocument4 pagesWorld Journal of Surgical OncologyWa Ode Nur AsrawatiNo ratings yet
- Sialolithiasis of The Submandibular Gland: Lberg R. Relationship of Intraoperative Rupture ofDocument4 pagesSialolithiasis of The Submandibular Gland: Lberg R. Relationship of Intraoperative Rupture ofCoryza Gabrie tanNo ratings yet
- Webb 2001Document9 pagesWebb 2001kaarlaamendezNo ratings yet
- Atypical Spitz Tumors: A Diagnostic ChallengeDocument8 pagesAtypical Spitz Tumors: A Diagnostic ChallengeCristi PopescuNo ratings yet
- Fine Needle Aspiration Cytology (FNAC) of GISTDocument7 pagesFine Needle Aspiration Cytology (FNAC) of GISTurfriendanshul100% (1)
- Adrenal Cortical TumorsDocument8 pagesAdrenal Cortical TumorsSabrina whtNo ratings yet
- Sentinel Lymph Node (SLN) Biopsy PDFDocument5 pagesSentinel Lymph Node (SLN) Biopsy PDFMDNo ratings yet
- 1 s2.0 S2210261221006337 MainDocument5 pages1 s2.0 S2210261221006337 MainRubén LimaNo ratings yet
- Squamous Cell Carcinoma and Precursor Lesions: Clinical PathologyDocument22 pagesSquamous Cell Carcinoma and Precursor Lesions: Clinical PathologyMmtandil0412No ratings yet
- Management of Visceral Vascular AnomaliesDocument5 pagesManagement of Visceral Vascular Anomalieswael.elzeneiniNo ratings yet
- Medical WagesDocument5 pagesMedical WagesnusyratNo ratings yet
- Jurnal Lipoma Inggris 1Document9 pagesJurnal Lipoma Inggris 1Yunawan Dwi PuspoNo ratings yet
- Skálová2022 Article UpdateFromThe5thEditionOfTheWo 220408 115830-1-5Document5 pagesSkálová2022 Article UpdateFromThe5thEditionOfTheWo 220408 115830-1-5Rocio CacñahuarayNo ratings yet
- Mod Path Ol 2015131Document17 pagesMod Path Ol 2015131Mariana UsatiiNo ratings yet
- Epithelioid Soft Tissue Tumors PDFDocument11 pagesEpithelioid Soft Tissue Tumors PDFnohemi9No ratings yet
- Spindle Cell LesionsDocument8 pagesSpindle Cell LesionsdrmanishsharmaNo ratings yet
- Small Round Cell Tumors of Soft Tissue and BoneDocument13 pagesSmall Round Cell Tumors of Soft Tissue and BoneAdriana Gabriela Ugarte MacíasNo ratings yet
- A Rare Case of Retroperitoneal and Mesenteric LymphangiomatosisDocument4 pagesA Rare Case of Retroperitoneal and Mesenteric LymphangiomatosisAndra KurniantoNo ratings yet
- Adult Desmoid Tumors: Biology, Management and Ongoing TrialsDocument7 pagesAdult Desmoid Tumors: Biology, Management and Ongoing TrialsGustavo GasperiNo ratings yet
- Sudour Bonnange2014Document3 pagesSudour Bonnange2014Abhishek JunghareNo ratings yet
- Lecture 8 (2)Document7 pagesLecture 8 (2)photo copyhemnNo ratings yet
- 1 Soft TissueDocument41 pages1 Soft TissuefadoNo ratings yet
- Salivary Gland Cancer: From Diagnosis to Tailored TreatmentFrom EverandSalivary Gland Cancer: From Diagnosis to Tailored TreatmentLisa LicitraNo ratings yet
- Assignment 2 Saloni Chaudhary 2019659564Document3 pagesAssignment 2 Saloni Chaudhary 2019659564Saloni ChaudharyNo ratings yet
- Potassium Bisulphate As A Food PreservativeDocument11 pagesPotassium Bisulphate As A Food PreservativeAdam Lang67% (6)
- IIB Sant Pau 2020 WebDocument336 pagesIIB Sant Pau 2020 WebAinhoa GaNo ratings yet
- Anticancer DrugsDocument6 pagesAnticancer DrugsmidhunNo ratings yet
- Psychic DevelopmentDocument13 pagesPsychic DevelopmentCult of Amon Ra100% (2)
- B 10 VRV 2042Document36 pagesB 10 VRV 2042api-283593849No ratings yet
- Chapter 49 Nervous SystemsDocument16 pagesChapter 49 Nervous Systems蔡旻珊No ratings yet
- PMR Examination 2004-2008Document9 pagesPMR Examination 2004-2008chlkhgNo ratings yet
- Ecozone Dichotomous KeyDocument3 pagesEcozone Dichotomous Keyqmtkqz72vhNo ratings yet
- Anti Bacterial and Biofilm Inhibitory Activities of Aegle Marmelos Methanol Leaf ExtractDocument9 pagesAnti Bacterial and Biofilm Inhibitory Activities of Aegle Marmelos Methanol Leaf ExtractIJAR JOURNALNo ratings yet
- BIOL 351 Lab Report IDocument2 pagesBIOL 351 Lab Report IshadowlightfoxNo ratings yet
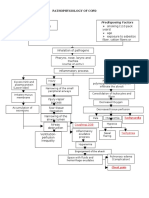
- Streptococcus Pneumonae: Pathophysiology of CopdDocument1 pageStreptococcus Pneumonae: Pathophysiology of CopdDimpal ChoudharyNo ratings yet
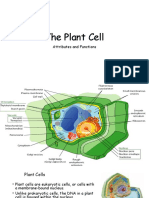
- The Plant CellDocument30 pagesThe Plant CellMichael GentilesNo ratings yet
- Advances in Prostaglandin, Leukotriene, and Other Bioactive Lipid ResearchDocument243 pagesAdvances in Prostaglandin, Leukotriene, and Other Bioactive Lipid ResearchCarmen PopaNo ratings yet
- Memory ProcessesDocument27 pagesMemory ProcessesClarissa LumainNo ratings yet
- Immunosuppressant DrugsDocument8 pagesImmunosuppressant DrugsandruuuNo ratings yet
- What I Can DoDocument4 pagesWhat I Can DoJoana Jean SuymanNo ratings yet
- Pewarisan Sifat Warna Dan Tipe Biji Jagungmanado KuningDocument8 pagesPewarisan Sifat Warna Dan Tipe Biji Jagungmanado KuningZallNo ratings yet
- Insectopia CompendiumDocument53 pagesInsectopia Compendiumnaruto hyuga67% (3)
- Stainning 2019Document29 pagesStainning 2019Almoatazbellah AbdallahNo ratings yet
- Determination of Ibuprofen and Paraben in Pharmaceutical Formulations Using Flowinjection and Derivative SpectrophotometryDocument2 pagesDetermination of Ibuprofen and Paraben in Pharmaceutical Formulations Using Flowinjection and Derivative Spectrophotometrycamelia_ioana_14No ratings yet
- P5P6Sci - Respiratory SystemDocument8 pagesP5P6Sci - Respiratory SystemLevyNo ratings yet
- MODULE-4 Understanding Harmony in The Nature and Existence - WholeDocument9 pagesMODULE-4 Understanding Harmony in The Nature and Existence - WholeTECHNO YASHNo ratings yet
- Effectiveness of Rhizobium Strains On Faba Bean Vicia Fabae L at Gumer District Highland Area of Southern EthiopiaDocument6 pagesEffectiveness of Rhizobium Strains On Faba Bean Vicia Fabae L at Gumer District Highland Area of Southern EthiopiaTarekegn TeferaNo ratings yet
- Human Reproductive SystemDocument5 pagesHuman Reproductive SystemSubatomoNo ratings yet
- نباتاتDocument2 pagesنباتاتhaneen refaeeNo ratings yet
- Chronic Leukemia HerfindalDocument40 pagesChronic Leukemia HerfindalAanshi ShahNo ratings yet
- Umbilical Cord Prolapse: Green-Top Guideline No. 50Document13 pagesUmbilical Cord Prolapse: Green-Top Guideline No. 50Nurul Aimi Abdul RahmanNo ratings yet