Download as pdf or txt
You might also like
- BI1001268978 - 1800792430MHC12023 - 06062023 - 1421 (1) MaxicareDocument1 pageBI1001268978 - 1800792430MHC12023 - 06062023 - 1421 (1) MaxicareJanet CafrancaNo ratings yet
- A - Level Project Work Insights & ReflectionsDocument3 pagesA - Level Project Work Insights & ReflectionsKou Uraki0% (1)
- Microsoft Invoice 1Document2 pagesMicrosoft Invoice 1Venkateswaran SankarNo ratings yet
- Iphone 11 Imagine PDFDocument2 pagesIphone 11 Imagine PDFJonassy SumaïliNo ratings yet
- Bi1000541546 8100183438MHC12021 10012021 1448Document1 pageBi1000541546 8100183438MHC12021 10012021 1448Yuna SyNo ratings yet
- Detailed Lesson Plan Template Ped701Document6 pagesDetailed Lesson Plan Template Ped701Jordan Cruz67% (9)
- Lumber Case ModelDocument6 pagesLumber Case ModeltheonlypaulNo ratings yet
- 346055215Document5 pages346055215Azhar SkNo ratings yet
- Life Insurance Premium Certificate: (Financial Year 2018-2019)Document1 pageLife Insurance Premium Certificate: (Financial Year 2018-2019)Sugar SugarNo ratings yet
- Mastercool Air Conditioner Service ManualDocument2 pagesMastercool Air Conditioner Service ManualJubril Akinwande100% (1)
- O & M of Sub StationDocument94 pagesO & M of Sub StationAlbert Sekar100% (2)
- Introduction To Fluorescence Techniques: Fluorophores and Their Amine-Reactive DerivativesDocument8 pagesIntroduction To Fluorescence Techniques: Fluorophores and Their Amine-Reactive DerivativesManoj Kumar ChaurasiaNo ratings yet
- Fotocopias Ingles Tema Climate 1º EsoDocument6 pagesFotocopias Ingles Tema Climate 1º EsoMayOrdóñezNo ratings yet
- Bi1000541546 8100183438MHC12021 10012021 1448Document1 pageBi1000541546 8100183438MHC12021 10012021 1448Yuna SyNo ratings yet
- Billing SampleDocument1 pageBilling SampleGlenn DomingoNo ratings yet
- Sun Cellular E-Bill-0171889715-2020-12-27Document6 pagesSun Cellular E-Bill-0171889715-2020-12-27アシイナ 江野No ratings yet
- Net4U Technology Pvt. LTD.: Ss Education Trust, UdaipurDocument1 pageNet4U Technology Pvt. LTD.: Ss Education Trust, UdaipurengineerluvNo ratings yet
- Ht2329i002681770 2Document4 pagesHt2329i002681770 2Chegg tutorsNo ratings yet
- NEDA-Acct#653716583-SOA July2020Document6 pagesNEDA-Acct#653716583-SOA July2020Pe Anthony NoricoNo ratings yet
- Notice of Assessment 2021 03 22 16 13 15 065002Document4 pagesNotice of Assessment 2021 03 22 16 13 15 065002kulbirsinghxxxxNo ratings yet
- RegularBill 1014488620 FINV-0000390050-22Document2 pagesRegularBill 1014488620 FINV-0000390050-22jean TuratsinzeNo ratings yet
- 1-5168703373979 Bm2508i000483611Document9 pages1-5168703373979 Bm2508i000483611simcotrackNo ratings yet
- Your Reliance Communications BillDocument4 pagesYour Reliance Communications BillSachin KumarNo ratings yet
- Screenshot 2023-08-17 at 8.59.53 AMDocument1 pageScreenshot 2023-08-17 at 8.59.53 AMsachin GourNo ratings yet
- BM2329I004951941Document5 pagesBM2329I004951941Divya VidyadharanNo ratings yet
- April-2023-Airtel Broad Band BillDocument1 pageApril-2023-Airtel Broad Band BillBharath KumarNo ratings yet
- Ht2329i003260837 1Document4 pagesHt2329i003260837 1Chegg tutorsNo ratings yet
- In - Selfx India Fashinza Event d2cDocument1 pageIn - Selfx India Fashinza Event d2camanpatniNo ratings yet
- PSO 1047341 Jan-2024 BillDocument92 pagesPSO 1047341 Jan-2024 BillfsarfrazNo ratings yet
- BM2329I014298415Document6 pagesBM2329I014298415Divya VidyadharanNo ratings yet
- Net4u Technology PVT LTD 724777780 PDFDocument1 pageNet4u Technology PVT LTD 724777780 PDFengineerluvNo ratings yet
- CardStatement - 2018 02 08Document6 pagesCardStatement - 2018 02 08data worksNo ratings yet
- Bharat Sanchar Nigam Limited: Invoice For Post Paid ServicesDocument23 pagesBharat Sanchar Nigam Limited: Invoice For Post Paid ServicesVenkataraju BadanapuriNo ratings yet
- Tax Invoice: Neo Structo Construction Pvt. LTDDocument1 pageTax Invoice: Neo Structo Construction Pvt. LTDnithinNo ratings yet
- West City Central School: Statement of AccountDocument4 pagesWest City Central School: Statement of AccountJulie Ann Bruzon GocelaNo ratings yet
- CMP Feb23 02624Document2 pagesCMP Feb23 02624dariusroz9No ratings yet
- Noa-Iit Ob2620220516193754ktiDocument2 pagesNoa-Iit Ob2620220516193754ktiSelva SelvaNo ratings yet
- Bharat Sanchar Nigam Limited: Invoice For Post Paid ServicesDocument23 pagesBharat Sanchar Nigam Limited: Invoice For Post Paid ServicesVenkataraju BadanapuriNo ratings yet
- Sept MobDocument6 pagesSept MobRohit JainNo ratings yet
- Premium Receipt: Personal DetailsDocument1 pagePremium Receipt: Personal DetailssunnybisnoiNo ratings yet
- Reg0000006788994Document2 pagesReg0000006788994Sachin jaswalNo ratings yet
- BM2329I009286404Document5 pagesBM2329I009286404Divya VidyadharanNo ratings yet
- Bm2433i012681094Document2 pagesBm2433i012681094geethakaniNo ratings yet
- Ostrea Mineral - Yellow For FileDocument7 pagesOstrea Mineral - Yellow For FileJaime II LustadoNo ratings yet
- Noa-Iit Ob2620220516204800b91Document2 pagesNoa-Iit Ob2620220516204800b91Tha OoNo ratings yet
- Statement of Account: Summary of Charges and CreditsDocument4 pagesStatement of Account: Summary of Charges and CreditsRitchelle Quijote DelgadoNo ratings yet
- Zprmrnot 22847670 15676911Document1 pageZprmrnot 22847670 15676911Gulshan GavelNo ratings yet
- Terp Asia Construction Corp.: Statement of AccountDocument4 pagesTerp Asia Construction Corp.: Statement of AccountMark Israel DirectoNo ratings yet
- Noa-Iit Ob2320170627071310ufp PDFDocument1 pageNoa-Iit Ob2320170627071310ufp PDFjasper haiNo ratings yet
- Previous Charges: Stephanie Anne PastorDocument4 pagesPrevious Charges: Stephanie Anne PastorDaniel ChuaNo ratings yet
- Tax I CasesDocument119 pagesTax I CasesJANINE MARIE BERNADETTE CASTRONo ratings yet
- Tax InvoiceDocument1 pageTax Invoiceqasim66935No ratings yet
- DateDocument1 pageDateAbhishek SharmaNo ratings yet
- Noa-Iit Ob2620220530013620coDocument1 pageNoa-Iit Ob2620220530013620coChan Yin YenNo ratings yet
- JKTIR00514115Document3 pagesJKTIR00514115Angrys EnjelinaNo ratings yet
- BM2409I000443244Document4 pagesBM2409I000443244shawmailNo ratings yet
- 1-5520045831101 Bm2519i000838170Document10 pages1-5520045831101 Bm2519i000838170hrleoimsNo ratings yet
- 3197 DDDDDocument1 page3197 DDDDAbhishek SharmaNo ratings yet
- Statement of Account: Summary of Charges and CreditsDocument4 pagesStatement of Account: Summary of Charges and CreditsVenice Shayne VillaflorNo ratings yet
- Installation City Bangalore GST No State Karnataka State Code 29Document5 pagesInstallation City Bangalore GST No State Karnataka State Code 29anujonwebNo ratings yet
- Íxl È0Â Pacaâanas Richelleâââ D Ç0 +&5 - Î Mrs. Richelle Distrajo Paca AnasDocument2 pagesÍxl È0Â Pacaâanas Richelleâââ D Ç0 +&5 - Î Mrs. Richelle Distrajo Paca AnasReyno D. Paca-anasNo ratings yet
- Amazon - in - Order 403-6138423-9776333Document1 pageAmazon - in - Order 403-6138423-9776333SanjayNo ratings yet
- May23 MobileDocument7 pagesMay23 Mobilepravin gaNo ratings yet
- Bill On Mobil To Know Your Bill Amount Through Your Registered Mobile Number, Send SMS in Following Format: SMS BILLINFO To 5676708Document1 pageBill On Mobil To Know Your Bill Amount Through Your Registered Mobile Number, Send SMS in Following Format: SMS BILLINFO To 5676708Amit YaduwanshiNo ratings yet
- 0181123303raro : MR Celso Iii Raro 0181123303 + 63 925-710 1880 2,200.00 Nonstop Lte 599Document4 pages0181123303raro : MR Celso Iii Raro 0181123303 + 63 925-710 1880 2,200.00 Nonstop Lte 599hebreojugadobsbmNo ratings yet
- Inbound Regular InvoiceDocument3 pagesInbound Regular InvoiceMutiara RachmawatyNo ratings yet
- J.K. Lasser's Small Business Taxes 2021: Your Complete Guide to a Better Bottom LineFrom EverandJ.K. Lasser's Small Business Taxes 2021: Your Complete Guide to a Better Bottom LineNo ratings yet
- Constitutional Law 1 Case Digests and NotesDocument186 pagesConstitutional Law 1 Case Digests and NotesJordan CruzNo ratings yet
- Inset Training Program Matrix FinalDocument5 pagesInset Training Program Matrix FinalJordan CruzNo ratings yet
- May Activities Letter.pdfDocument6 pagesMay Activities Letter.pdfJordan CruzNo ratings yet
- Room Assignment PartcipantsDocument6 pagesRoom Assignment PartcipantsJordan CruzNo ratings yet
- DM-284-s.-2024-SCHOOL-BASED-TRAINING-OF-TEACHERS-SBTT-ON-THE-MATATAG-CURRICULUMDocument2 pagesDM-284-s.-2024-SCHOOL-BASED-TRAINING-OF-TEACHERS-SBTT-ON-THE-MATATAG-CURRICULUMJordan CruzNo ratings yet
- CLUSTER-3-FIL-EPP-MAPEH-GMRC-ALMARIO-SBTT-ROOM-ASSIGNMENTDocument17 pagesCLUSTER-3-FIL-EPP-MAPEH-GMRC-ALMARIO-SBTT-ROOM-ASSIGNMENTJordan CruzNo ratings yet
- Program Flow Matatag 2024Document4 pagesProgram Flow Matatag 2024Jordan CruzNo ratings yet
- Interface-Meeting-with-Batch-1-SBTOT-LMTDocument36 pagesInterface-Meeting-with-Batch-1-SBTOT-LMTJordan CruzNo ratings yet
- Arts LESSON 2: Nature of Logo: ExpectationsDocument6 pagesArts LESSON 2: Nature of Logo: ExpectationsJordan CruzNo ratings yet
- University of The Philippines Open University Los Baños, Laguna 4031 PhilippinesDocument2 pagesUniversity of The Philippines Open University Los Baños, Laguna 4031 PhilippinesJordan CruzNo ratings yet
- Community of Practice (Cop) : Jordan Mitchell C. Cruz Masters of Arts in Social Science Education (Massed)Document35 pagesCommunity of Practice (Cop) : Jordan Mitchell C. Cruz Masters of Arts in Social Science Education (Massed)Jordan CruzNo ratings yet
- Request Form (Equipment)Document1 pageRequest Form (Equipment)Jordan CruzNo ratings yet
- District 3 Soccer/Football TrainerDocument2 pagesDistrict 3 Soccer/Football TrainerJordan CruzNo ratings yet
- DLL Mapeh 6 Whole YearDocument154 pagesDLL Mapeh 6 Whole YearJordan Cruz100% (1)
- My Ideal LeaderDocument4 pagesMy Ideal LeaderJordan CruzNo ratings yet
- Activity: (If The Space Is Not Enough, You May Use The Blank Space at The Back of This Paper)Document2 pagesActivity: (If The Space Is Not Enough, You May Use The Blank Space at The Back of This Paper)Jordan CruzNo ratings yet
- Memorandum of Agreement: Beneficiary BenefactorDocument2 pagesMemorandum of Agreement: Beneficiary BenefactorJordan CruzNo ratings yet
- Authority To SellDocument3 pagesAuthority To SellJordan CruzNo ratings yet
- Joint Affidavit-: Affiant AffiantDocument2 pagesJoint Affidavit-: Affiant AffiantJordan CruzNo ratings yet
- AuthorizationDocument1 pageAuthorizationJordan CruzNo ratings yet
- Sample Guide (Business Plan)Document50 pagesSample Guide (Business Plan)Jordan Cruz100% (1)
- Intellectual DisabilityDocument2 pagesIntellectual DisabilityJordan CruzNo ratings yet
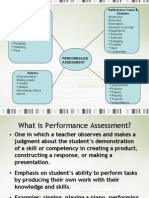
- Process Oriented Performance Based AssessmentDocument29 pagesProcess Oriented Performance Based AssessmentKristel Uy0% (1)
- Short Table of Muscle Control Exercises - The MaxaldingDocument48 pagesShort Table of Muscle Control Exercises - The MaxaldingHugo Mantilla90% (10)
- Chemistry Project 2021-2022Document19 pagesChemistry Project 2021-2022Rudra SathwaraNo ratings yet
- SPS Plans PDFDocument7 pagesSPS Plans PDFSalin ShresthaNo ratings yet
- BOQUILLASDocument2 pagesBOQUILLASEDUARDONo ratings yet
- IPC in Family PlanningDocument12 pagesIPC in Family PlanningHari MurtiNo ratings yet
- The History of The Big Bang TheoryDocument6 pagesThe History of The Big Bang Theorymay ann dimaanoNo ratings yet
- Bio OhDocument3 pagesBio OhEmmaNo ratings yet
- Brochure DM96Document12 pagesBrochure DM96Paul Avelino CallupeNo ratings yet
- Early Alt-RAMEC and Facial Mask Protocol in Class III MalocclusionDocument9 pagesEarly Alt-RAMEC and Facial Mask Protocol in Class III MalocclusionNievecillaNeiraNo ratings yet
- Covalence S1301-M Epoxy Primer: DescriptionDocument4 pagesCovalence S1301-M Epoxy Primer: DescriptionJuan Carlos Contreras CherresNo ratings yet
- PSP Assignment1Document25 pagesPSP Assignment1B BasitNo ratings yet
- Group3 Dilemmac pr6031Document8 pagesGroup3 Dilemmac pr6031api-576539858No ratings yet
- IdealStandard 120m-Frame R0094Document2 pagesIdealStandard 120m-Frame R0094nasser mhannaNo ratings yet
- G10 1st PERIODICAL TEST MAPEH10 TQDocument5 pagesG10 1st PERIODICAL TEST MAPEH10 TQMaricel LajeraNo ratings yet
- General Physics 1: ACTIVITY/ANSWER SHEET: Quarter 2Document1 pageGeneral Physics 1: ACTIVITY/ANSWER SHEET: Quarter 2Kashima KotaroNo ratings yet
- Sago Pudding - Recipes - Poh's KitchenDocument2 pagesSago Pudding - Recipes - Poh's KitchenXuxu TooNo ratings yet
- NeoCryl A-662 MsdsDocument4 pagesNeoCryl A-662 MsdsLeandro EsvizaNo ratings yet
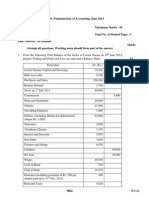
- Capinew Account June13Document7 pagesCapinew Account June13ashwinNo ratings yet
- MASB7 Construction Contract7Document3 pagesMASB7 Construction Contract7hyraldNo ratings yet
- Nanoengineered Silica-Properties PDFDocument18 pagesNanoengineered Silica-Properties PDFkevinNo ratings yet
- Cp1018 Boric Acid MsdsDocument6 pagesCp1018 Boric Acid MsdsPanneer SelvamNo ratings yet
- Science G7 Q2 LP4Document13 pagesScience G7 Q2 LP4Lovely GuintoNo ratings yet
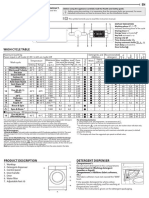
- Whirlpool BIWDWG861484uk enDocument4 pagesWhirlpool BIWDWG861484uk ennadaljoachim77No ratings yet
- Microbial Ecology of Sourdough Fermentations: Diverse or Uniform?Document19 pagesMicrobial Ecology of Sourdough Fermentations: Diverse or Uniform?roadrunner100% (1)