Download as pdf or txt
You might also like
- DOH ProgramsDocument114 pagesDOH ProgramsAlyssandra Luceno100% (6)
- 1 s2.0 S2666535222000349 MainDocument7 pages1 s2.0 S2666535222000349 Mainشهد موسىNo ratings yet
- The Vaccine Uptake Continuum: Applying Social Science Theory To Shift Vaccine HesitancyDocument5 pagesThe Vaccine Uptake Continuum: Applying Social Science Theory To Shift Vaccine HesitancyKitKath UwUNo ratings yet
- Vaccine HesitancyDocument12 pagesVaccine HesitancyMhd HidayattullahNo ratings yet
- Pediatr Clin North Am 2023 Tabla de ContenidoDocument4 pagesPediatr Clin North Am 2023 Tabla de ContenidocdsaludNo ratings yet
- Refusal of VaccinationDocument22 pagesRefusal of VaccinationElfatih Publishing0% (1)
- Vaccine Sentiments and Under Vaccination Attitudes and Behaviour Around Measles Mumps and Rubella Vaccine MMR in An Australian Cohort Mathew Toll Ang Li All ChapterDocument32 pagesVaccine Sentiments and Under Vaccination Attitudes and Behaviour Around Measles Mumps and Rubella Vaccine MMR in An Australian Cohort Mathew Toll Ang Li All Chaptereileen.laigo375100% (2)
- Vaccine Sentiments and Under Vaccination Attitudes and Behaviour Around Measles Mumps and Rubella Vaccine MMR in An Australian Cohort Mathew Toll Ang Li Ebook Full ChapterDocument32 pagesVaccine Sentiments and Under Vaccination Attitudes and Behaviour Around Measles Mumps and Rubella Vaccine MMR in An Australian Cohort Mathew Toll Ang Li Ebook Full Chapterjohn.sanmiguel190100% (6)
- 3. Understanding vaccine evaluation and safety as an approach to addresing parental concernsDocument6 pages3. Understanding vaccine evaluation and safety as an approach to addresing parental concernsguillermo benavidesNo ratings yet
- Final Presentation Vaccine Vision PDFDocument25 pagesFinal Presentation Vaccine Vision PDFapi-551647623No ratings yet
- Kelompok 12 - Article SummaryDocument22 pagesKelompok 12 - Article SummaryRahma HumairahNo ratings yet
- Wariness of VaccinesDocument45 pagesWariness of VaccinesNational Press FoundationNo ratings yet
- Final Chap 1 2Document19 pagesFinal Chap 1 2Avegail BulabogNo ratings yet
- WHO EURO 2021 2281 42036 57837 EngDocument77 pagesWHO EURO 2021 2281 42036 57837 EngRomeo TevesNo ratings yet
- Addressing Vaccine Hesitancy RDocument73 pagesAddressing Vaccine Hesitancy RShalini BaggaNo ratings yet
- Vaccine Sentiments and Under Vaccination Attitudes and Behaviour Around Measles Mumps and Rubella Vaccine MMR in An Australian Cohort Mathew Toll Ang Li Full Chapter PDFDocument34 pagesVaccine Sentiments and Under Vaccination Attitudes and Behaviour Around Measles Mumps and Rubella Vaccine MMR in An Australian Cohort Mathew Toll Ang Li Full Chapter PDFdimkasoeun100% (4)
- Full download Vaccine sentiments and under-vaccination: Attitudes and behaviour around Measles, Mumps, and Rubella vaccine (MMR) in an Australian cohort Mathew Toll & Ang Li file pdf all chapter on 2024Document44 pagesFull download Vaccine sentiments and under-vaccination: Attitudes and behaviour around Measles, Mumps, and Rubella vaccine (MMR) in an Australian cohort Mathew Toll & Ang Li file pdf all chapter on 2024vedanaayl100% (1)
- Paper RemoladoDocument57 pagesPaper RemoladoJan Michael R. RemoladoNo ratings yet
- A Healthy Community - Time 3Document6 pagesA Healthy Community - Time 3foodfoxaNo ratings yet
- Application 108 Discourse EthicsDocument5 pagesApplication 108 Discourse EthicsAngela Laurilla100% (1)
- Argumentative EssayDocument2 pagesArgumentative Essayjoyce anne GarciaNo ratings yet
- Journal of Clinical Nursing - 2021 - Al - E2 - 80 - 90amer - COVID - E2 - 80 - 9019 Vaccination Intention in The First Year of The Pandemic ADocument25 pagesJournal of Clinical Nursing - 2021 - Al - E2 - 80 - 90amer - COVID - E2 - 80 - 9019 Vaccination Intention in The First Year of The Pandemic AIsac MartinsNo ratings yet
- V VV Vvaccine Accine Accine Accine Accine Safety Safety Safety Safety SafetyDocument12 pagesV VV Vvaccine Accine Accine Accine Accine Safety Safety Safety Safety SafetyJandre ShancezNo ratings yet
- KSLING1Document5 pagesKSLING1Clarita BangunNo ratings yet
- Strategies Intended To Address Vaccine Hesitancy Review of Published Reviews - 2015 - VaccineDocument14 pagesStrategies Intended To Address Vaccine Hesitancy Review of Published Reviews - 2015 - VaccineFadhli Hasif IbrahimNo ratings yet
- 13th R.LDocument9 pages13th R.LWilliam Tac anNo ratings yet
- Restoring Confidence in Vaccines in The COVID-19 Era: Expert Review of VaccinesDocument4 pagesRestoring Confidence in Vaccines in The COVID-19 Era: Expert Review of VaccinesRaquel CostaNo ratings yet
- DocumentDocument2 pagesDocumentsamuelmiracle902No ratings yet
- Improving Knowledge and Power of HCW in BuildingDocument13 pagesImproving Knowledge and Power of HCW in BuildingYONASNo ratings yet
- Countering Vaccine Hesitancy Through Immunization Information Systems A Narrative ReviewDocument20 pagesCountering Vaccine Hesitancy Through Immunization Information Systems A Narrative ReviewAfdal FatoniNo ratings yet
- Review of Related LiteratureDocument18 pagesReview of Related LiteratureAllaiz g.No ratings yet
- CHAPTER 1-WPS OfficeDocument5 pagesCHAPTER 1-WPS OfficeAbdulrahman Abarani AdamNo ratings yet
- The VACCINES Act: Deciphering Vaccine Hesitancy in The Time of COVID-19Document3 pagesThe VACCINES Act: Deciphering Vaccine Hesitancy in The Time of COVID-19A009Karin Kurniati NurfatmahNo ratings yet
- May Be hindered-WPS OfficeDocument7 pagesMay Be hindered-WPS OfficeNorhani PanayamanNo ratings yet
- KAP ImmunizationDocument6 pagesKAP ImmunizationSherwin Buluran100% (1)
- Anti-Vaxxer MovementDocument174 pagesAnti-Vaxxer MovementMark A. FosterNo ratings yet
- Parental Delay or Refusal of Vaccine Doses, Childhood Vaccination Coverage at 24 Months of Age, and The Health Belief ModelDocument12 pagesParental Delay or Refusal of Vaccine Doses, Childhood Vaccination Coverage at 24 Months of Age, and The Health Belief ModelariNo ratings yet
- Degree of Acceptance of Residents Barangay Bibincahan To Vaccination Program of The Philippine GovernmentDocument24 pagesDegree of Acceptance of Residents Barangay Bibincahan To Vaccination Program of The Philippine GovernmentRJ DealcaNo ratings yet
- Practical Research 1 (K)Document17 pagesPractical Research 1 (K)Joshua ValledorNo ratings yet
- 1 Model Analyze Driversofvaccineconfidence 22 March PDFDocument5 pages1 Model Analyze Driversofvaccineconfidence 22 March PDFAsep KusnaliNo ratings yet
- Educate Yourself: Sanofi Pasteur's Fluzone® Vaccine Package InsertDocument2 pagesEducate Yourself: Sanofi Pasteur's Fluzone® Vaccine Package InsertAntonio JesusNo ratings yet
- Wagner 2020Document10 pagesWagner 2020Sue TudtudNo ratings yet
- C ECH en Group ActivityDocument3 pagesC ECH en Group ActivitySebastianNo ratings yet
- The Vaccine Handbook: A Practical Guide for Clinicians, Twelfth EditionFrom EverandThe Vaccine Handbook: A Practical Guide for Clinicians, Twelfth EditionNo ratings yet
- COMUNICATING PUBLIC HEALTH INFORMATION - Mutaz FakeerhDocument11 pagesCOMUNICATING PUBLIC HEALTH INFORMATION - Mutaz Fakeerhmutaz fakeerhNo ratings yet
- Vaccines 10 01402 v2Document13 pagesVaccines 10 01402 v2Neal TorwaneNo ratings yet
- From Package To Protection How Do We Close Global Coverage Gaps To Optimize The Impact of Vaccination 2014 PaperDocument6 pagesFrom Package To Protection How Do We Close Global Coverage Gaps To Optimize The Impact of Vaccination 2014 PaperediNo ratings yet
- Communication and HesitancyDocument3 pagesCommunication and HesitancydalauNo ratings yet
- Anti Vaccination 1Document10 pagesAnti Vaccination 1cooljoker1234No ratings yet
- Chapter 25: Education, Training, and Communication For HPV VaccinesDocument9 pagesChapter 25: Education, Training, and Communication For HPV Vaccineshst939No ratings yet
- Individual Preferences For COVID-19 Vaccination in ChinaDocument17 pagesIndividual Preferences For COVID-19 Vaccination in ChinaAntonio MoncayoNo ratings yet
- Vaccine DevelopmentDocument36 pagesVaccine DevelopmentTio Surya TirtadjajaNo ratings yet
- Anti-Vaccination PresentationDocument16 pagesAnti-Vaccination PresentationOuhaila Safieddine100% (1)
- 1 s2.0 S2667321522000075 MainDocument6 pages1 s2.0 S2667321522000075 MainNeal TorwaneNo ratings yet
- The Nature and Extent of COVID 19 Vaccination Hesitancy in Healthcare WorkersDocument8 pagesThe Nature and Extent of COVID 19 Vaccination Hesitancy in Healthcare WorkersamiryahiaNo ratings yet
- The Awareness Level On The Benefit1Document12 pagesThe Awareness Level On The Benefit1Joshua ValledorNo ratings yet
- Badr DKK 2021Document17 pagesBadr DKK 2021WoogyuNo ratings yet
- Chapter 1 3Document36 pagesChapter 1 3MaximusNo ratings yet
- summary-of-sage-vaccinehesitancy-enDocument5 pagessummary-of-sage-vaccinehesitancy-enCamila AmaralNo ratings yet
- Proposal For Long Term COVID 19 Control - v1.0Document16 pagesProposal For Long Term COVID 19 Control - v1.0bathmayentoopagenNo ratings yet
- Position Paper: Vanderbilt University Hospilal. Nashville. Tennessee, USADocument2 pagesPosition Paper: Vanderbilt University Hospilal. Nashville. Tennessee, USANoreen Udan AlbanoNo ratings yet
- MGA VACCINE NA SAKOP NG NIP: BCG Birth Dose, Hepatitis B Birth Dose, OralDocument3 pagesMGA VACCINE NA SAKOP NG NIP: BCG Birth Dose, Hepatitis B Birth Dose, OralVanessa AbboudNo ratings yet
- Lesson 1 Drug Classifications Illicit DrugsDocument16 pagesLesson 1 Drug Classifications Illicit DrugsKiyrahNo ratings yet
- Interpretation, Taylor & Francis Publiser, London.: Daftar PustakaDocument3 pagesInterpretation, Taylor & Francis Publiser, London.: Daftar PustakaAnonymous 5K38SwLNo ratings yet
- RNTCPDocument24 pagesRNTCParunjv1234100% (1)
- Panel Outcome Letter Patient Eligible For CHC MGDocument2 pagesPanel Outcome Letter Patient Eligible For CHC MGDivine Mercy Apostolate UKNo ratings yet
- Nueva EtiquetaDocument1 pageNueva EtiquetaAnderson Manuel Marquez NuñezNo ratings yet
- Tata Kelola Klinis: (Clinical Governance)Document38 pagesTata Kelola Klinis: (Clinical Governance)Devi TriyadiNo ratings yet
- Moitoring SheetDocument1 pageMoitoring SheetTrina de LeonNo ratings yet
- Violence Against Women PDFDocument91 pagesViolence Against Women PDFFairyNo ratings yet
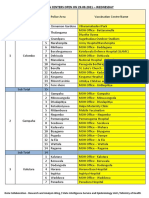
- Vaccination Centers On 29.09.2021Document6 pagesVaccination Centers On 29.09.2021Chanu On CTNo ratings yet
- Health Summative Test q3Document1 pageHealth Summative Test q3Christine Manjares - Oaña100% (1)
- FlyerDocument1 pageFlyersaggittarianNo ratings yet
- Public Health Recommendation For Fully Vaccinated 3-7-21 3 PM CleanDocument5 pagesPublic Health Recommendation For Fully Vaccinated 3-7-21 3 PM CleanJoseph Adinolfi Jr.No ratings yet
- Orientation ReportDocument38 pagesOrientation Reportapi-3698598No ratings yet
- The Role of Research in The Right To Health and The Universal Provision of Health CareDocument5 pagesThe Role of Research in The Right To Health and The Universal Provision of Health CareClaudio Gruber MannNo ratings yet
- PIIS0140673619325243Document2 pagesPIIS0140673619325243blue diamondNo ratings yet
- 2020 2021 Plan Comparison TableDocument161 pages2020 2021 Plan Comparison TableData hi DataNo ratings yet
- Implementing Health PolicyDocument334 pagesImplementing Health PolicyPramod Malik100% (2)
- March 1st WeekDocument101 pagesMarch 1st WeekTalina BinondoNo ratings yet
- ESSAY TOPIC NITA FinalDocument3 pagesESSAY TOPIC NITA FinalwideriNo ratings yet
- Handwashing ProposalDocument2 pagesHandwashing ProposalLevyCastilloNo ratings yet
- Environmental Health Impact Assessment of Development ProjectsDocument34 pagesEnvironmental Health Impact Assessment of Development ProjectsKolthoom AbabnehNo ratings yet
- Nadra Resume Formatted 082609Document8 pagesNadra Resume Formatted 082609amsalaliNo ratings yet
- NHS COVID Pass - Vaccinated: COVID-19 Vaccine Moderna (Booster)Document5 pagesNHS COVID Pass - Vaccinated: COVID-19 Vaccine Moderna (Booster)Grete BirtwistleNo ratings yet
- JSSK DC MHDocument17 pagesJSSK DC MHkailash chand atalNo ratings yet
- Final TPADocument40 pagesFinal TPAkushal87100% (1)
- MA COVID-19 Vaccine PresentationDocument8 pagesMA COVID-19 Vaccine PresentationJohn Waller100% (2)
- Sample Write It Down ShowDocument18 pagesSample Write It Down ShowFree Escort ServiceNo ratings yet
- MEMORANDUM To School Officials 11-15-21Document2 pagesMEMORANDUM To School Officials 11-15-21FOX13 MemphisNo ratings yet