Download as pdf or txt
You might also like
- Infectious Diseases - Gorbach & Bartlett, 3E (2004)Document2,559 pagesInfectious Diseases - Gorbach & Bartlett, 3E (2004)Mădălina SuciuNo ratings yet
- Drug Study: Beta-Lactmase-Producing Strains of S. Aureus, or by Piperacillin Tazobactam SusceptibleDocument2 pagesDrug Study: Beta-Lactmase-Producing Strains of S. Aureus, or by Piperacillin Tazobactam SusceptibleKristine Young83% (6)
- UTI TreatmentDocument3 pagesUTI TreatmentMaria RezitadinaNo ratings yet
- UTI Treatment Algorithm - Sharp Mesa Vista 2Document3 pagesUTI Treatment Algorithm - Sharp Mesa Vista 2Fitri 1997No ratings yet
- Augmenten (Amoxicillin Clavulan)Document2 pagesAugmenten (Amoxicillin Clavulan)Adrianne BazoNo ratings yet
- Cefuroxime Losartan DRUG STUDYDocument7 pagesCefuroxime Losartan DRUG STUDYKiela Therese LabroNo ratings yet
- Classification: Cefditoren, As This Agent May CauseDocument3 pagesClassification: Cefditoren, As This Agent May CauseHavier EsparagueraNo ratings yet
- AppendectomyDocument6 pagesAppendectomyapi-3797941100% (10)
- Paediatric ManualDocument223 pagesPaediatric ManualKyra PoggenpoelNo ratings yet
- Drug AnalysisDocument8 pagesDrug AnalysisDaniel Andre S. SomorayNo ratings yet
- Infection Antimicrobial Medication CardsDocument16 pagesInfection Antimicrobial Medication Cards方郝建No ratings yet
- Name of Drugs, Classification, Dosage & Route Action Indication Side Effects Nursing ResponsibilitiesDocument5 pagesName of Drugs, Classification, Dosage & Route Action Indication Side Effects Nursing ResponsibilitiesAiramCeszDelaCruzNo ratings yet
- Acute Abdominal Pain: DR Naing Naing Oo Senior LecturerDocument28 pagesAcute Abdominal Pain: DR Naing Naing Oo Senior LecturerAbdulrahman NajiNo ratings yet
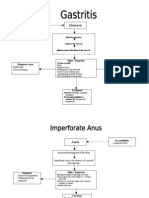
- Gastro PathophysiologyDocument4 pagesGastro PathophysiologyPaul JoloNo ratings yet
- Omep, Ceftriaxone, FurosemideDocument3 pagesOmep, Ceftriaxone, FurosemideThyataira chuaNo ratings yet
- Urinary Tract Infection and Pyelonephritis AIIMS Kalyani 7th SemesterDocument39 pagesUrinary Tract Infection and Pyelonephritis AIIMS Kalyani 7th Semesterrakesh raushanNo ratings yet
- Shivani PDFDocument3 pagesShivani PDFdeepukumarNo ratings yet
- Chapter 36 The Urinary System in GynaecologyDocument19 pagesChapter 36 The Urinary System in Gynaecologypmj050gpNo ratings yet
- By: Clarissa E. Guifaya BSN301/GROUP 3Document17 pagesBy: Clarissa E. Guifaya BSN301/GROUP 3Clarissa GuifayaNo ratings yet
- Drug StudyDocument22 pagesDrug StudySierraSiwaNo ratings yet
- Drug StudyDocument22 pagesDrug StudySierraSiwaNo ratings yet
- Urinary Tract InfectionDocument42 pagesUrinary Tract InfectionhaniNo ratings yet
- Morning Report - PyelonephritisDocument54 pagesMorning Report - PyelonephritisjonNo ratings yet
- The Diagnosis and Treatment of Adult Urinary Tract Infections inDocument22 pagesThe Diagnosis and Treatment of Adult Urinary Tract Infections inPaola Andrea Balsero SalgadoNo ratings yet
- CeftriaxoneDocument5 pagesCeftriaxoneCastillo MikaellaNo ratings yet
- PeritonitisDocument15 pagesPeritonitiscgqphqdrytNo ratings yet
- A Case Study: Nephrolit HiasisDocument19 pagesA Case Study: Nephrolit HiasisCarna BuenconsejoNo ratings yet
- CefalexinDocument1 pageCefalexinVien Demasu-ayNo ratings yet
- Acute Pyelonephritis: Causes/ Risk FactorsDocument6 pagesAcute Pyelonephritis: Causes/ Risk FactorsShiraishiNo ratings yet
- Appendicitis: Diseases and Conditions: AppendicitisDocument6 pagesAppendicitis: Diseases and Conditions: AppendicitisWen RodsaNo ratings yet
- Invanz (Ertapenem)Document2 pagesInvanz (Ertapenem)E100% (1)
- JM Drug Study CaseDocument4 pagesJM Drug Study CaseMilky Lescano LargozaNo ratings yet
- Dipolog Medical Center College Foundation Inc. College of NursingDocument16 pagesDipolog Medical Center College Foundation Inc. College of NursingTiffany AdriasNo ratings yet
- DS - Mod9Document2 pagesDS - Mod9designericlelynsoronioNo ratings yet
- Drug StudyDocument12 pagesDrug StudyJessica Pacris MaramagNo ratings yet
- Generic Name Dosage / Frequency Action Side Effects Nursing ResponsibilityDocument9 pagesGeneric Name Dosage / Frequency Action Side Effects Nursing Responsibilityorhocelo6908No ratings yet
- Olores Drugstudy Cephalothin SodiumDocument7 pagesOlores Drugstudy Cephalothin SodiumTintin KingNo ratings yet
- Rle Rot 4Document3 pagesRle Rot 4Elle RosalesNo ratings yet
- HyperbilirubinemiaDocument10 pagesHyperbilirubinemiachiboogs456100% (1)
- Pancreatitis Group 3 NCM 116Document21 pagesPancreatitis Group 3 NCM 116Diana Jane LauretaNo ratings yet
- JFP - 1986 09 - v23 - I3 - A Case of Chronic AppendicitisDocument2 pagesJFP - 1986 09 - v23 - I3 - A Case of Chronic AppendicitisBilalNo ratings yet
- PyelonephritisDocument10 pagesPyelonephritisalina abu rumi100% (1)
- Evangelista Drug-StudyDocument15 pagesEvangelista Drug-Studydinglasanerica57No ratings yet
- 4 Cefazolin Drug StudyDocument4 pages4 Cefazolin Drug Studyshadow gonzalezNo ratings yet
- Canuuc - Uti May 2017Document31 pagesCanuuc - Uti May 2017Praluki HerliawanNo ratings yet
- Tamoxifen NolvadexDocument1 pageTamoxifen NolvadexAdrianne Bazo100% (1)
- Surgical AbdomenDocument3 pagesSurgical Abdomendude dNo ratings yet
- UTI Disorder PDFDocument23 pagesUTI Disorder PDFMonarahayuNo ratings yet
- Acute Appendicitis: History and ExaminationDocument6 pagesAcute Appendicitis: History and ExaminationPraktek Dokter Umum drjosefdrelsyNo ratings yet
- Does My Patient Need To Be Screened or Treated For A Urinary Tract InfectionDocument4 pagesDoes My Patient Need To Be Screened or Treated For A Urinary Tract Infectiontsiko111No ratings yet
- Cefuroxime Drug StudyDocument3 pagesCefuroxime Drug StudyRem remNo ratings yet
- 5551 13868 1 PBDocument6 pages5551 13868 1 PBNanaNo ratings yet
- Drug Study: Name Mechanism of Action Indication/Contraindication Side Effects Nursing ResponsibilityDocument2 pagesDrug Study: Name Mechanism of Action Indication/Contraindication Side Effects Nursing ResponsibilityJoshua DavantesNo ratings yet
- Dysphagia, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandDysphagia, A Simple Guide To The Condition, Treatment And Related ConditionsRating: 5 out of 5 stars5/5 (1)
- The Perfect Ic Diet Cookbook The Complete Nutrition Guide To Healing Chronic Pelvic Pain And Managing Symptoms Of Interstitial Cystitis With Delectable And Nourishing RecipesFrom EverandThe Perfect Ic Diet Cookbook The Complete Nutrition Guide To Healing Chronic Pelvic Pain And Managing Symptoms Of Interstitial Cystitis With Delectable And Nourishing RecipesNo ratings yet
- Diverticulosis, A Simple Guide to the Condition, Treatment and Related DiseasesFrom EverandDiverticulosis, A Simple Guide to the Condition, Treatment and Related DiseasesRating: 1 out of 5 stars1/5 (1)
- The Perfect Neutropenic Diet Cookbook; The Complete Nutrition Guide To Reinstating Overall Health For General Wellness With Delectable And Nourishing RecipesFrom EverandThe Perfect Neutropenic Diet Cookbook; The Complete Nutrition Guide To Reinstating Overall Health For General Wellness With Delectable And Nourishing RecipesNo ratings yet
- HandoutsDocument74 pagesHandoutschayChay gapolNo ratings yet
- Theories of Disease Causation Level200Document5 pagesTheories of Disease Causation Level200Annan Agyekum JoshuaNo ratings yet
- Tigecycline Alone or in CombinationDocument13 pagesTigecycline Alone or in CombinationSanjay NavaleNo ratings yet
- Essay:-''Coronaviruses Are A Family of Viruses Known For Containing Strains That Cause PotentiallyDocument4 pagesEssay:-''Coronaviruses Are A Family of Viruses Known For Containing Strains That Cause PotentiallymuddasirnaddemNo ratings yet
- Lec 5Document16 pagesLec 5Bassam AlgalalyNo ratings yet
- Binda BIO3219 Lab5Document12 pagesBinda BIO3219 Lab5Ronaldo BindaNo ratings yet
- Part IIDocument15 pagesPart IIIan LapidezNo ratings yet
- A Plant Pathologist or A Student Taking Plant Pathology Is Often Asked by Friends or Associates The Following QuestionsDocument21 pagesA Plant Pathologist or A Student Taking Plant Pathology Is Often Asked by Friends or Associates The Following QuestionsMirza ZiaaNo ratings yet
- Cosmetic Contact Lens-Related Corneal Infections in AsiaDocument8 pagesCosmetic Contact Lens-Related Corneal Infections in AsiaAnggitaNo ratings yet
- WHO IVB 15.09 EngDocument59 pagesWHO IVB 15.09 EngAbdul AhadNo ratings yet
- Otitis MediaDocument2 pagesOtitis MediaKoushik Mazumder ShuvoNo ratings yet
- 2022.11.30 - Celeste Solum - Moving in For The KillDocument20 pages2022.11.30 - Celeste Solum - Moving in For The KillJFBrNo ratings yet
- WJG 27 1691Document26 pagesWJG 27 1691Valentina QuinteroNo ratings yet
- Summary OphthalmologyDocument86 pagesSummary Ophthalmologymarina_shawkyNo ratings yet
- Uhuru's Sixteenth Presidential Address On Covid-19Document10 pagesUhuru's Sixteenth Presidential Address On Covid-19The Star KenyaNo ratings yet
- Lab Manual - Sputum - Microscopy (Final)Document117 pagesLab Manual - Sputum - Microscopy (Final)kushwaha.santosh290No ratings yet
- IN893000 v6.0 Clearview PBP2a SA Culture Colony ProducDocument101 pagesIN893000 v6.0 Clearview PBP2a SA Culture Colony ProducRazaz AdilNo ratings yet
- Tubex Test PDFDocument2 pagesTubex Test PDFHenry Philip Sabado Presto100% (1)
- infection 7 (تم حفظه تلقائيا)Document22 pagesinfection 7 (تم حفظه تلقائيا)مرتضى محمد منصورNo ratings yet
- Vaccines of The National Immunization Program of TDocument7 pagesVaccines of The National Immunization Program of T1BSN04 DE GUZMAN, LEMARRY JOYCE V.No ratings yet
- Molecular Biology of The Gene: Chapter ObjectivesDocument17 pagesMolecular Biology of The Gene: Chapter Objectivesirene9tan9ailianNo ratings yet
- Schematic Diagram of Pleural EffusionDocument2 pagesSchematic Diagram of Pleural EffusionJesselle Laserna0% (1)
- The Concept of Public HealthDocument13 pagesThe Concept of Public Healthhamza althariNo ratings yet
- Water Pollution and Human HealthDocument5 pagesWater Pollution and Human HealthPurusottam AgarwalNo ratings yet
- ST George Respiratory QUestionnaireDocument6 pagesST George Respiratory QUestionnaireFranciscoJ.ReynaSepúlvedaNo ratings yet
- What Are Bacteroides ?Document13 pagesWhat Are Bacteroides ?u77No ratings yet
- Reflection: "See The Light at The End of The Tunnel"Document2 pagesReflection: "See The Light at The End of The Tunnel"John Flex SingculanNo ratings yet
- Health and IllnessDocument3 pagesHealth and Illnessfrico13No ratings yet
- Environmental Hazards and Human HealthDocument36 pagesEnvironmental Hazards and Human HealthJohn Mark CelosaNo ratings yet