
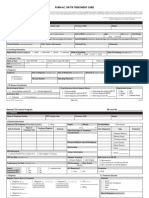
DRTB Treatment Card
DRTB Treatment Card
You might also like
- Merit Is A Must! - A Clinical Clerk's Guide To Oral Revalida EmergenciesDocument177 pagesMerit Is A Must! - A Clinical Clerk's Guide To Oral Revalida Emergencies유미Yoo100% (1)
- TB DOTS TREATMENT BOOKLET Form - 5 - v051320Document6 pagesTB DOTS TREATMENT BOOKLET Form - 5 - v051320Kim PeroNo ratings yet
- Mortality & Death Audit FormatsDocument6 pagesMortality & Death Audit FormatsAnindya Biswas100% (2)
- National TB Control Program Form 7 - Referral FormDocument1 pageNational TB Control Program Form 7 - Referral FormAre Pee EtcNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)narayanasmrithiNo ratings yet
- Kci Vac Therapy Vtiaf UpdatedDocument2 pagesKci Vac Therapy Vtiaf UpdatedHi BeyoNo ratings yet
- TB.-DSTB-FORMDocument6 pagesTB.-DSTB-FORMMaycel DumayaNo ratings yet
- Form 4c v050120Document8 pagesForm 4c v050120talbaruelNo ratings yet
- Form 4b v050120Document4 pagesForm 4b v050120Estarmio ZaficoNo ratings yet
- TB DOTS Form - 4a - v050120Document1 pageTB DOTS Form - 4a - v050120Kim PeroNo ratings yet
- TB DOTS TPT Form - v050120Document2 pagesTB DOTS TPT Form - v050120Kim PeroNo ratings yet
- Form 7 v050120Document2 pagesForm 7 v050120Northern Benguet District-hNo ratings yet
- Form 7 v050120Document2 pagesForm 7 v050120nursing sectionNo ratings yet
- NTP Referral FormDocument2 pagesNTP Referral FormCarl RamosNo ratings yet
- Clinical Treatment PDFDocument1 pageClinical Treatment PDFDanielle YoderNo ratings yet
- Clinical Treatment Form: I DIAGNOSES (Must Be To The Highest Level of Specificity)Document1 pageClinical Treatment Form: I DIAGNOSES (Must Be To The Highest Level of Specificity)Danielle YoderNo ratings yet
- TB DOTS Form - 2b - v030220Document1 pageTB DOTS Form - 2b - v030220Kim PeroNo ratings yet
- DR TB REGISTER A3 SizeDocument5 pagesDR TB REGISTER A3 Sizeabdullee354No ratings yet
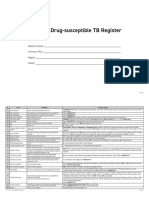
- Form 6a. Drug Susceptible TB RegisterDocument4 pagesForm 6a. Drug Susceptible TB RegisterAllen ChesterNo ratings yet
- Unit TB Register A3Document6 pagesUnit TB Register A3abdullee354No ratings yet
- BwergnwoienbDocument3 pagesBwergnwoienbpobayed154No ratings yet
- Discharge Planning TBDocument2 pagesDischarge Planning TBNurida LatipahNo ratings yet
- Case Investigation Form: DiphtheriaDocument3 pagesCase Investigation Form: DiphtheriaSalihu MustaphaNo ratings yet
- Pre Authorization FormDocument1 pagePre Authorization FormMurugan RamalingamNo ratings yet
- Zika IcifDocument2 pagesZika IcifMarav SymbNo ratings yet
- Printable Version - Approval Reference No - 60247630Document2 pagesPrintable Version - Approval Reference No - 60247630sohaibkhaled5858No ratings yet
- ADR AEFI Reporting FormDocument1 pageADR AEFI Reporting Formgulafsha1No ratings yet
- Emt Physical FormDocument1 pageEmt Physical FormLeeann LopezNo ratings yet
- AuthtoDiscloseProtectedPHI NH 900010Document1 pageAuthtoDiscloseProtectedPHI NH 900010brooklynlowe24No ratings yet
- Appendix 4a - Patient Registration Form GuidanceDocument4 pagesAppendix 4a - Patient Registration Form GuidanceYuwono AriyantoNo ratings yet
- 4a - Patient Registration FormDocument7 pages4a - Patient Registration FormHygiena Kumala SuciNo ratings yet
- CIF DiphDocument2 pagesCIF DiphIvy marie BonNo ratings yet
- Health Center/Clinic/Hospital: Out Patient Department (OPD) RegisterDocument4 pagesHealth Center/Clinic/Hospital: Out Patient Department (OPD) RegisterGetu Tadele100% (2)
- Test Case 3 OASIS - RedactedDocument39 pagesTest Case 3 OASIS - RedactedFernando Galera Jr.No ratings yet
- ESR Verification Form ReviseDocument4 pagesESR Verification Form ReviseRouella DoverteNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Document3 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)forged godNo ratings yet
- ESR Verification Form - Revise-Dina JoyDocument3 pagesESR Verification Form - Revise-Dina Joymawab.rhuNo ratings yet
- CR 1009155289Document2 pagesCR 1009155289Billy AlfonsoNo ratings yet
- Template Registration Form and Consent Form V3 - Final For RPSDocument7 pagesTemplate Registration Form and Consent Form V3 - Final For RPSHamdi PutraNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Document3 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Lavanya LakshmiNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Lakshay JunejaNo ratings yet
- Application Form For HospitalDocument5 pagesApplication Form For HospitalRhodora BenipayoNo ratings yet
- Claim Form of TPL LifeDocument2 pagesClaim Form of TPL LifeYasir MushtaqNo ratings yet
- Health Immunization Clearance Form: Section A: ImmunizationsDocument3 pagesHealth Immunization Clearance Form: Section A: ImmunizationsFaith SetikNo ratings yet
- Reimbursement-Form-16.05.2023 NextcareDocument1 pageReimbursement-Form-16.05.2023 NextcareAbdul Kabiru SalifuNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Bharat BhushanNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)DevNo ratings yet
- Application For Permit To Construct A Health FacilityDocument3 pagesApplication For Permit To Construct A Health FacilityquesterNo ratings yet
- Form 1: Cashless Request Form Iffco Tokio General Insurance Company LimitedDocument2 pagesForm 1: Cashless Request Form Iffco Tokio General Insurance Company LimitedRaju.PalNo ratings yet
- CIF PertussisDocument2 pagesCIF PertussisDan Joseph AguilarNo ratings yet
- 5.sample Case Report CRF Template FormDocument32 pages5.sample Case Report CRF Template FormmilenabogojevskaNo ratings yet
- Guidance Tool For TB Notification in India - FINALDocument92 pagesGuidance Tool For TB Notification in India - FINALYogendra UikeyNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Madhusmita MishraNo ratings yet
- Reliance Health Insurance Pre Authorisation FormDocument4 pagesReliance Health Insurance Pre Authorisation FormM/s MicrotechNo ratings yet
- Attending Physician's Statement For Proposed Insured/OwnerDocument2 pagesAttending Physician's Statement For Proposed Insured/OwnerSincerely ReynNo ratings yet
- Sonam Pre Auth Form 2Document5 pagesSonam Pre Auth Form 2Vishu SinghNo ratings yet
- Health Facilities and Services Regulatory Bureau: Republic of The Philippines Department of HealthDocument3 pagesHealth Facilities and Services Regulatory Bureau: Republic of The Philippines Department of HealthAZGH HOSPITAL /Cyberdyne PhilippinesNo ratings yet
- Certificate of Hospital Treatment - 17062019Document2 pagesCertificate of Hospital Treatment - 17062019Everest HospitalNo ratings yet
- Histopathology Reporting: Guidelines for Surgical CancerFrom EverandHistopathology Reporting: Guidelines for Surgical CancerDavid P. BoyleNo ratings yet
- Diabetes Mellitus and Its Complications in Najaf City, IraqDocument6 pagesDiabetes Mellitus and Its Complications in Najaf City, IraqYaman HassanNo ratings yet
- Photodynamic Therapy: Ishaque PK 123680033Document17 pagesPhotodynamic Therapy: Ishaque PK 123680033Vikas VikiNo ratings yet
- Format No. 1-2019-PSS-01 Rev.1Document1 pageFormat No. 1-2019-PSS-01 Rev.1nithinNo ratings yet
- Syrgery Mock 2Document8 pagesSyrgery Mock 2aa.No ratings yet
- Diabetes Mellitus: Meglitinid Es Sglt2 InhibitorsDocument2 pagesDiabetes Mellitus: Meglitinid Es Sglt2 InhibitorsMikha TheAngelzNo ratings yet
- Cl2354 MST Screening Tool 2021Document1 pageCl2354 MST Screening Tool 2021Gogo RouNo ratings yet
- TABLE A14 - Physical Exam Labs and Other DataDocument1 pageTABLE A14 - Physical Exam Labs and Other DataDragutin PetrićNo ratings yet
- Drug Study: (Celecoxib)Document11 pagesDrug Study: (Celecoxib)Princess Brigitte R. PATE�ANo ratings yet
- Asperger's Symptoms in Adults - Diagnosis, Treatment, and More - HOLLANDDocument11 pagesAsperger's Symptoms in Adults - Diagnosis, Treatment, and More - HOLLANDRoxan PacsayNo ratings yet
- Antimicrobial Profiling Research Defense 2Document64 pagesAntimicrobial Profiling Research Defense 2aimanusmangmsuiitphNo ratings yet
- Magnesium Article by Walter Last From Nexus MagazineDocument6 pagesMagnesium Article by Walter Last From Nexus MagazineCarlos SolergibertNo ratings yet
- Prostate Cancer: Palliative Care and Pain ReliefDocument14 pagesProstate Cancer: Palliative Care and Pain ReliefArif Tri Prasetyo HarunNo ratings yet
- Yemen Pharma MCQ Book PDFDocument195 pagesYemen Pharma MCQ Book PDFUsama HameedNo ratings yet
- Vulvar Cancer: Clinical Manifestations, Diagnosis, and PathologyDocument2 pagesVulvar Cancer: Clinical Manifestations, Diagnosis, and PathologyAde YonataNo ratings yet
- Scoliosis: Aka: Idiopathic Scoliosis, Adolescent ScoliosisDocument12 pagesScoliosis: Aka: Idiopathic Scoliosis, Adolescent ScoliosisLei Coloma SissonNo ratings yet
- MODULE 3 MDC SYLLABUS STUDY GUIDE - FinalDocument12 pagesMODULE 3 MDC SYLLABUS STUDY GUIDE - FinalAreesha ANo ratings yet
- Microbiology: Presented by Alyazeed Hussein, BSCDocument64 pagesMicrobiology: Presented by Alyazeed Hussein, BSCT N100% (1)
- PKC AryanDocument62 pagesPKC AryanAryan PurohitNo ratings yet
- Trends in Pharmaceutical IndustryDocument20 pagesTrends in Pharmaceutical IndustryAbdelhamidgmNo ratings yet
- NCM 109 RLE Gyne Ward Case StudyDocument12 pagesNCM 109 RLE Gyne Ward Case StudyRosenda CruzNo ratings yet
- Anti ProtozoaDocument29 pagesAnti ProtozoaIsheanesu MugwisiNo ratings yet
- Adult Health Nursing Ii: Unit Vi: Eye and Ent NursingDocument45 pagesAdult Health Nursing Ii: Unit Vi: Eye and Ent NursingabidaNo ratings yet
- Worksheet CCJM Post OpDocument3 pagesWorksheet CCJM Post Opapi-631170779No ratings yet
- Lab Report NewDocument2 pagesLab Report Newnsdh5v5v5sNo ratings yet
- Applications and Indications of Medical Ozone PDFDocument22 pagesApplications and Indications of Medical Ozone PDFweb3351No ratings yet
- Approach To SOBDocument25 pagesApproach To SOBabdiyare7134No ratings yet
- Pancreatic Diseases: Dr. Norizal Mohd NoorDocument53 pagesPancreatic Diseases: Dr. Norizal Mohd NoorTower AlangNo ratings yet
- Nejmcps 2304844Document6 pagesNejmcps 2304844AntoineNo ratings yet
- (CPG) Acute Myeloid Leukemia National Clinical Practice GuidelinesDocument91 pages(CPG) Acute Myeloid Leukemia National Clinical Practice GuidelinesKai ChuaNo ratings yet























































































Download as docx, pdf, or txt
You might also like
- Merit Is A Must! - A Clinical Clerk's Guide To Oral Revalida EmergenciesDocument177 pagesMerit Is A Must! - A Clinical Clerk's Guide To Oral Revalida Emergencies유미Yoo100% (1)
- TB DOTS TREATMENT BOOKLET Form - 5 - v051320Document6 pagesTB DOTS TREATMENT BOOKLET Form - 5 - v051320Kim PeroNo ratings yet
- Mortality & Death Audit FormatsDocument6 pagesMortality & Death Audit FormatsAnindya Biswas100% (2)
- National TB Control Program Form 7 - Referral FormDocument1 pageNational TB Control Program Form 7 - Referral FormAre Pee EtcNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)narayanasmrithiNo ratings yet
- Kci Vac Therapy Vtiaf UpdatedDocument2 pagesKci Vac Therapy Vtiaf UpdatedHi BeyoNo ratings yet
- TB.-DSTB-FORMDocument6 pagesTB.-DSTB-FORMMaycel DumayaNo ratings yet
- Form 4c v050120Document8 pagesForm 4c v050120talbaruelNo ratings yet
- Form 4b v050120Document4 pagesForm 4b v050120Estarmio ZaficoNo ratings yet
- TB DOTS Form - 4a - v050120Document1 pageTB DOTS Form - 4a - v050120Kim PeroNo ratings yet
- TB DOTS TPT Form - v050120Document2 pagesTB DOTS TPT Form - v050120Kim PeroNo ratings yet
- Form 7 v050120Document2 pagesForm 7 v050120Northern Benguet District-hNo ratings yet
- Form 7 v050120Document2 pagesForm 7 v050120nursing sectionNo ratings yet
- NTP Referral FormDocument2 pagesNTP Referral FormCarl RamosNo ratings yet
- Clinical Treatment PDFDocument1 pageClinical Treatment PDFDanielle YoderNo ratings yet
- Clinical Treatment Form: I DIAGNOSES (Must Be To The Highest Level of Specificity)Document1 pageClinical Treatment Form: I DIAGNOSES (Must Be To The Highest Level of Specificity)Danielle YoderNo ratings yet
- TB DOTS Form - 2b - v030220Document1 pageTB DOTS Form - 2b - v030220Kim PeroNo ratings yet
- DR TB REGISTER A3 SizeDocument5 pagesDR TB REGISTER A3 Sizeabdullee354No ratings yet
- Form 6a. Drug Susceptible TB RegisterDocument4 pagesForm 6a. Drug Susceptible TB RegisterAllen ChesterNo ratings yet
- Unit TB Register A3Document6 pagesUnit TB Register A3abdullee354No ratings yet
- BwergnwoienbDocument3 pagesBwergnwoienbpobayed154No ratings yet
- Discharge Planning TBDocument2 pagesDischarge Planning TBNurida LatipahNo ratings yet
- Case Investigation Form: DiphtheriaDocument3 pagesCase Investigation Form: DiphtheriaSalihu MustaphaNo ratings yet
- Pre Authorization FormDocument1 pagePre Authorization FormMurugan RamalingamNo ratings yet
- Zika IcifDocument2 pagesZika IcifMarav SymbNo ratings yet
- Printable Version - Approval Reference No - 60247630Document2 pagesPrintable Version - Approval Reference No - 60247630sohaibkhaled5858No ratings yet
- ADR AEFI Reporting FormDocument1 pageADR AEFI Reporting Formgulafsha1No ratings yet
- Emt Physical FormDocument1 pageEmt Physical FormLeeann LopezNo ratings yet
- AuthtoDiscloseProtectedPHI NH 900010Document1 pageAuthtoDiscloseProtectedPHI NH 900010brooklynlowe24No ratings yet
- Appendix 4a - Patient Registration Form GuidanceDocument4 pagesAppendix 4a - Patient Registration Form GuidanceYuwono AriyantoNo ratings yet
- 4a - Patient Registration FormDocument7 pages4a - Patient Registration FormHygiena Kumala SuciNo ratings yet
- CIF DiphDocument2 pagesCIF DiphIvy marie BonNo ratings yet
- Health Center/Clinic/Hospital: Out Patient Department (OPD) RegisterDocument4 pagesHealth Center/Clinic/Hospital: Out Patient Department (OPD) RegisterGetu Tadele100% (2)
- Test Case 3 OASIS - RedactedDocument39 pagesTest Case 3 OASIS - RedactedFernando Galera Jr.No ratings yet
- ESR Verification Form ReviseDocument4 pagesESR Verification Form ReviseRouella DoverteNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Document3 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)forged godNo ratings yet
- ESR Verification Form - Revise-Dina JoyDocument3 pagesESR Verification Form - Revise-Dina Joymawab.rhuNo ratings yet
- CR 1009155289Document2 pagesCR 1009155289Billy AlfonsoNo ratings yet
- Template Registration Form and Consent Form V3 - Final For RPSDocument7 pagesTemplate Registration Form and Consent Form V3 - Final For RPSHamdi PutraNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Document3 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Lavanya LakshmiNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Lakshay JunejaNo ratings yet
- Application Form For HospitalDocument5 pagesApplication Form For HospitalRhodora BenipayoNo ratings yet
- Claim Form of TPL LifeDocument2 pagesClaim Form of TPL LifeYasir MushtaqNo ratings yet
- Health Immunization Clearance Form: Section A: ImmunizationsDocument3 pagesHealth Immunization Clearance Form: Section A: ImmunizationsFaith SetikNo ratings yet
- Reimbursement-Form-16.05.2023 NextcareDocument1 pageReimbursement-Form-16.05.2023 NextcareAbdul Kabiru SalifuNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Bharat BhushanNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)DevNo ratings yet
- Application For Permit To Construct A Health FacilityDocument3 pagesApplication For Permit To Construct A Health FacilityquesterNo ratings yet
- Form 1: Cashless Request Form Iffco Tokio General Insurance Company LimitedDocument2 pagesForm 1: Cashless Request Form Iffco Tokio General Insurance Company LimitedRaju.PalNo ratings yet
- CIF PertussisDocument2 pagesCIF PertussisDan Joseph AguilarNo ratings yet
- 5.sample Case Report CRF Template FormDocument32 pages5.sample Case Report CRF Template FormmilenabogojevskaNo ratings yet
- Guidance Tool For TB Notification in India - FINALDocument92 pagesGuidance Tool For TB Notification in India - FINALYogendra UikeyNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Madhusmita MishraNo ratings yet
- Reliance Health Insurance Pre Authorisation FormDocument4 pagesReliance Health Insurance Pre Authorisation FormM/s MicrotechNo ratings yet
- Attending Physician's Statement For Proposed Insured/OwnerDocument2 pagesAttending Physician's Statement For Proposed Insured/OwnerSincerely ReynNo ratings yet
- Sonam Pre Auth Form 2Document5 pagesSonam Pre Auth Form 2Vishu SinghNo ratings yet
- Health Facilities and Services Regulatory Bureau: Republic of The Philippines Department of HealthDocument3 pagesHealth Facilities and Services Regulatory Bureau: Republic of The Philippines Department of HealthAZGH HOSPITAL /Cyberdyne PhilippinesNo ratings yet
- Certificate of Hospital Treatment - 17062019Document2 pagesCertificate of Hospital Treatment - 17062019Everest HospitalNo ratings yet
- Histopathology Reporting: Guidelines for Surgical CancerFrom EverandHistopathology Reporting: Guidelines for Surgical CancerDavid P. BoyleNo ratings yet
- Diabetes Mellitus and Its Complications in Najaf City, IraqDocument6 pagesDiabetes Mellitus and Its Complications in Najaf City, IraqYaman HassanNo ratings yet
- Photodynamic Therapy: Ishaque PK 123680033Document17 pagesPhotodynamic Therapy: Ishaque PK 123680033Vikas VikiNo ratings yet
- Format No. 1-2019-PSS-01 Rev.1Document1 pageFormat No. 1-2019-PSS-01 Rev.1nithinNo ratings yet
- Syrgery Mock 2Document8 pagesSyrgery Mock 2aa.No ratings yet
- Diabetes Mellitus: Meglitinid Es Sglt2 InhibitorsDocument2 pagesDiabetes Mellitus: Meglitinid Es Sglt2 InhibitorsMikha TheAngelzNo ratings yet
- Cl2354 MST Screening Tool 2021Document1 pageCl2354 MST Screening Tool 2021Gogo RouNo ratings yet
- TABLE A14 - Physical Exam Labs and Other DataDocument1 pageTABLE A14 - Physical Exam Labs and Other DataDragutin PetrićNo ratings yet
- Drug Study: (Celecoxib)Document11 pagesDrug Study: (Celecoxib)Princess Brigitte R. PATE�ANo ratings yet
- Asperger's Symptoms in Adults - Diagnosis, Treatment, and More - HOLLANDDocument11 pagesAsperger's Symptoms in Adults - Diagnosis, Treatment, and More - HOLLANDRoxan PacsayNo ratings yet
- Antimicrobial Profiling Research Defense 2Document64 pagesAntimicrobial Profiling Research Defense 2aimanusmangmsuiitphNo ratings yet
- Magnesium Article by Walter Last From Nexus MagazineDocument6 pagesMagnesium Article by Walter Last From Nexus MagazineCarlos SolergibertNo ratings yet
- Prostate Cancer: Palliative Care and Pain ReliefDocument14 pagesProstate Cancer: Palliative Care and Pain ReliefArif Tri Prasetyo HarunNo ratings yet
- Yemen Pharma MCQ Book PDFDocument195 pagesYemen Pharma MCQ Book PDFUsama HameedNo ratings yet
- Vulvar Cancer: Clinical Manifestations, Diagnosis, and PathologyDocument2 pagesVulvar Cancer: Clinical Manifestations, Diagnosis, and PathologyAde YonataNo ratings yet
- Scoliosis: Aka: Idiopathic Scoliosis, Adolescent ScoliosisDocument12 pagesScoliosis: Aka: Idiopathic Scoliosis, Adolescent ScoliosisLei Coloma SissonNo ratings yet
- MODULE 3 MDC SYLLABUS STUDY GUIDE - FinalDocument12 pagesMODULE 3 MDC SYLLABUS STUDY GUIDE - FinalAreesha ANo ratings yet
- Microbiology: Presented by Alyazeed Hussein, BSCDocument64 pagesMicrobiology: Presented by Alyazeed Hussein, BSCT N100% (1)
- PKC AryanDocument62 pagesPKC AryanAryan PurohitNo ratings yet
- Trends in Pharmaceutical IndustryDocument20 pagesTrends in Pharmaceutical IndustryAbdelhamidgmNo ratings yet
- NCM 109 RLE Gyne Ward Case StudyDocument12 pagesNCM 109 RLE Gyne Ward Case StudyRosenda CruzNo ratings yet
- Anti ProtozoaDocument29 pagesAnti ProtozoaIsheanesu MugwisiNo ratings yet
- Adult Health Nursing Ii: Unit Vi: Eye and Ent NursingDocument45 pagesAdult Health Nursing Ii: Unit Vi: Eye and Ent NursingabidaNo ratings yet
- Worksheet CCJM Post OpDocument3 pagesWorksheet CCJM Post Opapi-631170779No ratings yet
- Lab Report NewDocument2 pagesLab Report Newnsdh5v5v5sNo ratings yet
- Applications and Indications of Medical Ozone PDFDocument22 pagesApplications and Indications of Medical Ozone PDFweb3351No ratings yet
- Approach To SOBDocument25 pagesApproach To SOBabdiyare7134No ratings yet
- Pancreatic Diseases: Dr. Norizal Mohd NoorDocument53 pagesPancreatic Diseases: Dr. Norizal Mohd NoorTower AlangNo ratings yet
- Nejmcps 2304844Document6 pagesNejmcps 2304844AntoineNo ratings yet
- (CPG) Acute Myeloid Leukemia National Clinical Practice GuidelinesDocument91 pages(CPG) Acute Myeloid Leukemia National Clinical Practice GuidelinesKai ChuaNo ratings yet