Download as pdf or txt
You might also like
- Sap Basis Administration Handbook Netweaver Edition by Mereddy, RanjitDocument669 pagesSap Basis Administration Handbook Netweaver Edition by Mereddy, Ranjitvardhan.venkatNo ratings yet
- Subhepatic Appendix: An Ectopic Topography Not To Be Disregarded: A Case ReportDocument4 pagesSubhepatic Appendix: An Ectopic Topography Not To Be Disregarded: A Case ReportPawan MishraNo ratings yet
- Jurnal Case ReportDocument3 pagesJurnal Case ReportNining Rhyanie TampubolonNo ratings yet
- Morgagni Hernia Presented As Sudden Dyspnea in 70 Years Old ManDocument7 pagesMorgagni Hernia Presented As Sudden Dyspnea in 70 Years Old ManabuzeadNo ratings yet
- 1 s2.0 S2213576621002050 MainDocument6 pages1 s2.0 S2213576621002050 MainHusnul HanifaNo ratings yet
- MainDocument5 pagesMainajengiracilyNo ratings yet
- Two Cases of Right Congenital Diaphragmatic Herni 2024 International JournalDocument4 pagesTwo Cases of Right Congenital Diaphragmatic Herni 2024 International JournalRonald QuezadaNo ratings yet
- Abdomen FungusDocument7 pagesAbdomen FungusHAMMADNo ratings yet
- A Case of Primary Actinomycosis and Secondary Eumycetoma in Anterior Abdomen Wall - A Case ReportDocument7 pagesA Case of Primary Actinomycosis and Secondary Eumycetoma in Anterior Abdomen Wall - A Case ReportHAMMADNo ratings yet
- Case Report Small Intestinal Diverticulosis: A Rare Cause of Intestinal Perforation RevisitedDocument6 pagesCase Report Small Intestinal Diverticulosis: A Rare Cause of Intestinal Perforation RevisitedYeudiel SuroNo ratings yet
- CDH ReviewDocument12 pagesCDH ReviewDene DeneNo ratings yet
- Surgical ArticleDocument8 pagesSurgical ArticleKevin Leo Lucero AragonesNo ratings yet
- A Colonic Lipoma at The Origin of Acute Intestinal Intussusception in The Adult: A Case ReportDocument3 pagesA Colonic Lipoma at The Origin of Acute Intestinal Intussusception in The Adult: A Case ReportIJAR JOURNALNo ratings yet
- Bladder Diverticulum and SepsisDocument4 pagesBladder Diverticulum and SepsisInternational Medical PublisherNo ratings yet
- Traumatic Diaphragmatic Hernia: Key Words: Trauma, Diaphragm, HerniaDocument3 pagesTraumatic Diaphragmatic Hernia: Key Words: Trauma, Diaphragm, HerniaRangga Duo RamadanNo ratings yet
- Comparison of Transverse and Vertical Skin Incision ForDocument6 pagesComparison of Transverse and Vertical Skin Incision ForHerry SasukeNo ratings yet
- Full Text of - AMC SurgeryDocument407 pagesFull Text of - AMC SurgeryFarah FarahNo ratings yet
- 2.11 SEPTIC ABORTION AND SEPTIC SHOCK. M. Botes PDFDocument4 pages2.11 SEPTIC ABORTION AND SEPTIC SHOCK. M. Botes PDFteteh_thikeuNo ratings yet
- Esophageal EmergenciesDocument15 pagesEsophageal EmergenciesOmar SolisNo ratings yet
- Code - 2216 - Congenital EventrationDocument5 pagesCode - 2216 - Congenital EventrationHumaida Hasan SamiraNo ratings yet
- Surgical ExamDocument302 pagesSurgical ExamHossam SabriNo ratings yet
- Journal of Clinical and Translational Endocrinology: Case ReportsDocument5 pagesJournal of Clinical and Translational Endocrinology: Case ReportsKartikaa YantiiNo ratings yet
- Sabitson - Appendiks EngDocument17 pagesSabitson - Appendiks Engzeek powerNo ratings yet
- Clin Cas 1Document5 pagesClin Cas 1Dragos Viorel ScripcariuNo ratings yet
- Journal of Research and Practice: SurgeryDocument8 pagesJournal of Research and Practice: SurgeryAthenaeum Scientific PublishersNo ratings yet
- Spontaneous Perforation of A Malignified Corrosive Stricture of The Esophagus and Subsequent Perforation of A Giant Duodenal Stress UlcusDocument4 pagesSpontaneous Perforation of A Malignified Corrosive Stricture of The Esophagus and Subsequent Perforation of A Giant Duodenal Stress UlcusTeodorNo ratings yet
- 1 s2.0 S2210261221012268 MainDocument4 pages1 s2.0 S2210261221012268 Mainzenatihanen123No ratings yet
- Gastric Volvulus Through Morgagni Hernia and Intestinal Diverticulosis in An Adult Patient: A Case ReportDocument5 pagesGastric Volvulus Through Morgagni Hernia and Intestinal Diverticulosis in An Adult Patient: A Case ReportVirginia JawaNo ratings yet
- Appendicitis NCSDocument25 pagesAppendicitis NCSZyrah Ziska ZafraNo ratings yet
- Case Report: Airway Complications From An Esophageal Foreign BodyDocument4 pagesCase Report: Airway Complications From An Esophageal Foreign BodymawarmelatiNo ratings yet
- Jurnal Bedah 2Document5 pagesJurnal Bedah 2nafamaulidinaNo ratings yet
- Sub Diaphragmatic Abscess Leading To Empyema Thoracis in A Case of Perforated Appendix A Rare Case ReportDocument4 pagesSub Diaphragmatic Abscess Leading To Empyema Thoracis in A Case of Perforated Appendix A Rare Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Ectopic Abdominal Pregnancies: About 2 CasesDocument10 pagesEctopic Abdominal Pregnancies: About 2 CasesIJAR JOURNALNo ratings yet
- Rare Small Bowel Carcinoid Tumor A Case ReportDocument5 pagesRare Small Bowel Carcinoid Tumor A Case ReportAthenaeum Scientific PublishersNo ratings yet
- Tarlac State UniversityDocument11 pagesTarlac State UniversityJenica DancilNo ratings yet
- Chilaiditi Syndrom in Child Diagnostic Trap (Case Report)Document6 pagesChilaiditi Syndrom in Child Diagnostic Trap (Case Report)IJAR JOURNALNo ratings yet
- Congenital AnomaliesDocument22 pagesCongenital Anomaliesjessy100% (1)
- Appendicitis: Mark W. Jones Hassam Zulfiqar Jeffrey G. DeppenDocument7 pagesAppendicitis: Mark W. Jones Hassam Zulfiqar Jeffrey G. DeppenAndi HairunNo ratings yet
- Umbilical Hernia Repair MedscapeDocument5 pagesUmbilical Hernia Repair MedscapeVanessa Au YongNo ratings yet
- Article: Cases JournalDocument6 pagesArticle: Cases JournalgheaastridgayatriNo ratings yet
- Corrosive InjuryDocument6 pagesCorrosive InjuryCristian O. Saavedra RodriguezNo ratings yet
- Liver Abscess DissertationDocument4 pagesLiver Abscess DissertationPayForAPaperAtlanta100% (1)
- Acquired Diaphragmatic HerniaDocument8 pagesAcquired Diaphragmatic HerniaAmirul Zakiya BraveryNo ratings yet
- Diagnosing Gastric Volvulus in Chest X-Ray: Report of Three CasesDocument4 pagesDiagnosing Gastric Volvulus in Chest X-Ray: Report of Three CasesSuraj KurmiNo ratings yet
- Chest Tube ThoracostomyDocument5 pagesChest Tube Thoracostomy2M SANCHEZ, CYLESNo ratings yet
- Adult Intussusception A Case ReportDocument4 pagesAdult Intussusception A Case ReportRahmanssNo ratings yet
- Journal Homepage: - : IntroductionDocument7 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- Laparoscopic Repair of Delayed Traumatic Diaphragmatic Hernia With MeshDocument3 pagesLaparoscopic Repair of Delayed Traumatic Diaphragmatic Hernia With MeshFelix JeoNo ratings yet
- 1 PBDocument9 pages1 PBMariiaNo ratings yet
- The Diaphragm - Thoracic IncisionsDocument36 pagesThe Diaphragm - Thoracic IncisionsMustafa SafaaNo ratings yet
- Extra Pelvic Endometriosis: Double Ileal and Ileo-Caecal Localization Revealed by Acute Small Bowel Obstruction, A Clinical CaseDocument9 pagesExtra Pelvic Endometriosis: Double Ileal and Ileo-Caecal Localization Revealed by Acute Small Bowel Obstruction, A Clinical CaseIJAR JOURNALNo ratings yet
- Enarm Train Quiz WoaDocument231 pagesEnarm Train Quiz WoaJohon Lou MartinezNo ratings yet
- IJGM 51504 Pseudomyxoma Peritonei A Clinical Case of This Poorly Under - 030314 PDFDocument5 pagesIJGM 51504 Pseudomyxoma Peritonei A Clinical Case of This Poorly Under - 030314 PDFjhon heriansyahNo ratings yet
- Brunner's Gland Adenoma: Case ReportDocument3 pagesBrunner's Gland Adenoma: Case ReportasclepiuspdfsNo ratings yet
- CDH Modern MXDocument11 pagesCDH Modern MXphobicmdNo ratings yet
- Congenital Asymptomatic Diaphragmatic Hernias in Adults: A Case SeriesDocument8 pagesCongenital Asymptomatic Diaphragmatic Hernias in Adults: A Case SeriesRangga Duo RamadanNo ratings yet
- 1 s2.0 S1743919113000307 Main PDFDocument5 pages1 s2.0 S1743919113000307 Main PDFkunkkonkNo ratings yet
- Infertility Secondary To An Infected Hydrocele A Case ReportDocument2 pagesInfertility Secondary To An Infected Hydrocele A Case ReportSara AhmedNo ratings yet
- APPENDICITISDocument4 pagesAPPENDICITISalyanadayritNo ratings yet
- Post-cholecystectomy Bile Duct InjuryFrom EverandPost-cholecystectomy Bile Duct InjuryVinay K. KapoorNo ratings yet
- ALLPS SurgeryDocument10 pagesALLPS SurgeryAndres Neira QuezadaNo ratings yet
- Adult Intestinal TransplantationDocument14 pagesAdult Intestinal TransplantationAndres Neira QuezadaNo ratings yet
- The Best Closure Technique Without Mesh in ElectivDocument7 pagesThe Best Closure Technique Without Mesh in ElectivAndres Neira QuezadaNo ratings yet
- Nutricion PerioperatoriaDocument11 pagesNutricion PerioperatoriaAndres Neira QuezadaNo ratings yet
- NOM Trauma HepaticoDocument6 pagesNOM Trauma HepaticoAndres Neira QuezadaNo ratings yet
- Nissen Fundoplication - StatPearls - NCBI BookshelfDocument9 pagesNissen Fundoplication - StatPearls - NCBI BookshelfAndres Neira QuezadaNo ratings yet
- BUTJMS APPRAISALOFCOMPANIESANDALLIEDMATTERSACT2020 OdeyindeDocument12 pagesBUTJMS APPRAISALOFCOMPANIESANDALLIEDMATTERSACT2020 OdeyindeOyin AyoNo ratings yet
- Tata Technologies Limited: Corporate Identity Number: U72200PN1994PLC013313Document436 pagesTata Technologies Limited: Corporate Identity Number: U72200PN1994PLC013313RoshanNo ratings yet
- Esah 3.1Document34 pagesEsah 3.1maurice86100% (1)
- 02 Wage RegisterDocument7 pages02 Wage RegisterShritej nirmalNo ratings yet
- GEOGRAPHY GRADE 10 TERM 3 WEEK 5 LESSON 5 15 JulyDocument6 pagesGEOGRAPHY GRADE 10 TERM 3 WEEK 5 LESSON 5 15 JulyshanolkersNo ratings yet
- AlienDog A4 FreeDocument10 pagesAlienDog A4 FreeCarlaNo ratings yet
- UAP Transfer FormDocument1 pageUAP Transfer FormAThaddeusAntonio100% (1)
- All Over India IBR Candidate List - CBB AuthorisationDocument6 pagesAll Over India IBR Candidate List - CBB Authorisationsanjay joshiNo ratings yet
- Evonik Energy Services India - An IntroductionDocument11 pagesEvonik Energy Services India - An IntroductionvbharathiNo ratings yet
- Au Abhi 31-MarchDocument2 pagesAu Abhi 31-MarchShubhra Kanti GopeNo ratings yet
- Audit of Investment - 2Document4 pagesAudit of Investment - 2Juvy Dimaano0% (1)
- SKYLANDERS SWAP Force Xbox One GAME MANUALDocument14 pagesSKYLANDERS SWAP Force Xbox One GAME MANUALsamverbiskyNo ratings yet
- Adobe Scan 03 Dec 2022Document2 pagesAdobe Scan 03 Dec 2022Om DubeyNo ratings yet
- Architect Acts 2016 PDFDocument92 pagesArchitect Acts 2016 PDFKelingwgongNo ratings yet
- Postpaid Monthly Statement: 1151.14 ImmediatelyDocument4 pagesPostpaid Monthly Statement: 1151.14 Immediatelymaha37devNo ratings yet
- Grand Priory HistoryDocument54 pagesGrand Priory HistoryChilcos FlavianNo ratings yet
- Mbof912d Assignment 1 PDFDocument8 pagesMbof912d Assignment 1 PDFArneet SarnaNo ratings yet
- Enakmen Rizab Melayu 1930Document19 pagesEnakmen Rizab Melayu 1930IzzahJannahNo ratings yet
- Vocabulary 7 Money and ShoppingDocument2 pagesVocabulary 7 Money and ShoppingELENANo ratings yet
- International Arbitration Conference - MNLU Mumbai - 6 December PDFDocument4 pagesInternational Arbitration Conference - MNLU Mumbai - 6 December PDFRCR 75No ratings yet
- Marketing - Individual Assignment - StudentDocument5 pagesMarketing - Individual Assignment - StudentababsenNo ratings yet
- Ownership & OrganizationDocument26 pagesOwnership & Organizationpink_butterfly206No ratings yet
- Performance Audit City of Oaklands Homeless Encampment Management Interventions and ActivitiesDocument102 pagesPerformance Audit City of Oaklands Homeless Encampment Management Interventions and ActivitiesZennie AbrahamNo ratings yet
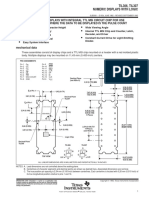
- TIL306, TIL307 Numeric Displays With LogicDocument9 pagesTIL306, TIL307 Numeric Displays With LogicNadjNo ratings yet
- WS - QHSE - S23 - G05 - Cement Head - 3313701 - 07Document17 pagesWS - QHSE - S23 - G05 - Cement Head - 3313701 - 07CiprianHnNo ratings yet
- Business Math Lesson1 Week 3Document6 pagesBusiness Math Lesson1 Week 3REBECCA BRIONES0% (1)
- Problem Areas in Legal EthicsDocument23 pagesProblem Areas in Legal Ethicsybun0% (1)
- LRC TranscriptDocument30 pagesLRC TranscriptPat PowersNo ratings yet
- Detector de Voltaje AmprobeDocument2 pagesDetector de Voltaje AmprobeLionel RamosNo ratings yet