
HIV RESISTANCE SURVEY FOLLOWING DOLUTEGRAVIR BASED REGIMENS
HIV RESISTANCE SURVEY FOLLOWING DOLUTEGRAVIR BASED REGIMENS
You might also like
- International Journal of Infectious Diseases: SciencedirectDocument5 pagesInternational Journal of Infectious Diseases: SciencedirectMuh Syukriadi AnsarNo ratings yet
- The Role of a Pharmacist in the Analysis of Adherence Rates and Associated Factors in HIV-Patients Registered on Centralized Chronic Medicines Dispensing and Distribution (CCMDD) Programme in the Public Sector in South AfricaDocument11 pagesThe Role of a Pharmacist in the Analysis of Adherence Rates and Associated Factors in HIV-Patients Registered on Centralized Chronic Medicines Dispensing and Distribution (CCMDD) Programme in the Public Sector in South AfricaSabrina JonesNo ratings yet
- Viruses 14 02208Document16 pagesViruses 14 02208jhonny12321No ratings yet
- The HIV Care Continuum and HIV-1 Drug Resistance Among Female Sex Workers: A Key Population in Guinea-BissauDocument11 pagesThe HIV Care Continuum and HIV-1 Drug Resistance Among Female Sex Workers: A Key Population in Guinea-Bissautomasarino74No ratings yet
- Journal of Clinical Tuberculosis and Other Mycobacterial DiseasesDocument16 pagesJournal of Clinical Tuberculosis and Other Mycobacterial DiseasesIlna RamadhaniNo ratings yet
- Understanding The Gaps in DR TB Care Casc - 2020 - Journal of Clinical TuberculoDocument16 pagesUnderstanding The Gaps in DR TB Care Casc - 2020 - Journal of Clinical TuberculoKarina ChristantoNo ratings yet
- Therapeutic Drug Monitoring in Human Immunodeficiency Virus/Acquired Immunodeficiency SyndromeDocument3 pagesTherapeutic Drug Monitoring in Human Immunodeficiency Virus/Acquired Immunodeficiency SyndromeFransiskus Samuel RenaldiNo ratings yet
- s42269 022 00961 3Document9 pagess42269 022 00961 3Cliff Daniel DIANZOLE MOUNKANANo ratings yet
- Detectable Viral Load and Human Immuno Deficiency Drug ResistanceDocument11 pagesDetectable Viral Load and Human Immuno Deficiency Drug ResistanceFelistus KanjiraNo ratings yet
- Long-Acting Antiretrovirals: A New Era For The Management and Prevention of HIV InfectionDocument13 pagesLong-Acting Antiretrovirals: A New Era For The Management and Prevention of HIV InfectionRobles Murillo Carlos Eduardo Augusto 1FNo ratings yet
- Piaa 030Document10 pagesPiaa 030Suryadi LimardiNo ratings yet
- Effects of Adherence To Antiretroviral Therapy On Body Mass Index, Immunological and Virological Status of Nigerians Living With HIV/AIDSDocument4 pagesEffects of Adherence To Antiretroviral Therapy On Body Mass Index, Immunological and Virological Status of Nigerians Living With HIV/AIDSDavidNo ratings yet
- Journal Pone 0245498Document36 pagesJournal Pone 0245498Aklilu FelekeNo ratings yet
- Comparison of The Efficacy and Safety of 2 Different Antiretroviral Regimens in Tertiary Care Hospital: A Retrospective Observational StudyDocument5 pagesComparison of The Efficacy and Safety of 2 Different Antiretroviral Regimens in Tertiary Care Hospital: A Retrospective Observational StudyNarendranath SNo ratings yet
- Hiv 13 1111Document8 pagesHiv 13 1111Cliff Daniel DIANZOLE MOUNKANANo ratings yet
- Isoniazid Prophylaxis Highly Effective But UnderutDocument2 pagesIsoniazid Prophylaxis Highly Effective But Underutemilianoarteagagarcia11No ratings yet
- Adhearence GechoDocument9 pagesAdhearence Gechosinte beyuNo ratings yet
- Malaria Treatment-Seeking Behaviour and Its Associated FactorsDocument34 pagesMalaria Treatment-Seeking Behaviour and Its Associated FactorsDaniel BoibanNo ratings yet
- Knowledge, Attitudes, and Practices (KAP) of Healthcare Workers On Viral Hepatitis B and Its Vaccination in 12 Health Establishments in The Centre Region of CameroonDocument8 pagesKnowledge, Attitudes, and Practices (KAP) of Healthcare Workers On Viral Hepatitis B and Its Vaccination in 12 Health Establishments in The Centre Region of CameroonInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Lester 2010Document8 pagesLester 2010Riska Resty WasitaNo ratings yet
- s12879 021 06459 ZDocument11 pagess12879 021 06459 ZCliff Daniel DIANZOLE MOUNKANANo ratings yet
- Pone 0150849Document12 pagesPone 0150849yeremia imanuelNo ratings yet
- Research Article: Factors Affecting Compliance of Infection Control Measures Among Dental RadiographersDocument11 pagesResearch Article: Factors Affecting Compliance of Infection Control Measures Among Dental RadiographersPRADNJA SURYA PARAMITHANo ratings yet
- Role of Telepharmacy in Pharmacist Counselling To Coronavirus Disease 2019 Patients and Medication Dispensing ErrorsDocument10 pagesRole of Telepharmacy in Pharmacist Counselling To Coronavirus Disease 2019 Patients and Medication Dispensing ErrorsIndra Braja MaespatiNo ratings yet
- 1 s2.0 S2210803316300781 MainDocument8 pages1 s2.0 S2210803316300781 MainGilang Aji P. EmonNo ratings yet
- Dengvaxia VaccineDocument8 pagesDengvaxia VaccineBayek NgekekNo ratings yet
- Management of Antiretroviral Therapy With Boosted Protease Inhibitors-Darunavir/Ritonavir or Darunavir/CobicistatDocument36 pagesManagement of Antiretroviral Therapy With Boosted Protease Inhibitors-Darunavir/Ritonavir or Darunavir/Cobicistatnegru paulNo ratings yet
- Effectiveness of Outreach Clinical Mentoring On Retention in Care and Viral Suppression Among HIV Positive Young Persons On Art in North Central NigeriaDocument8 pagesEffectiveness of Outreach Clinical Mentoring On Retention in Care and Viral Suppression Among HIV Positive Young Persons On Art in North Central NigeriaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Journal Pone 0254890Document16 pagesJournal Pone 0254890muhammmad haris faisalNo ratings yet
- Khawcharoenporn2014 PDFDocument10 pagesKhawcharoenporn2014 PDFsinta belaNo ratings yet
- Comparative Exploration of Patient Related Factors That Influence Adherence To ART Among HIV Patients Attending Jinja Regional Referral Hospital.Document10 pagesComparative Exploration of Patient Related Factors That Influence Adherence To ART Among HIV Patients Attending Jinja Regional Referral Hospital.KIU PUBLICATION AND EXTENSIONNo ratings yet
- Patient-Centered Telehealth Solution For Observed Urine Collections in Substance Use Disorder Care Delivery During COVID-19 and BeyondDocument8 pagesPatient-Centered Telehealth Solution For Observed Urine Collections in Substance Use Disorder Care Delivery During COVID-19 and Beyondvovinda rujianaNo ratings yet
- ART Chapter One SubmissionDocument10 pagesART Chapter One SubmissionbstogarepiNo ratings yet
- Nomogram Model For Predicting The Risk of Multidrug-Resistant Bacteria Infection in Diabetic Foot PatientsDocument12 pagesNomogram Model For Predicting The Risk of Multidrug-Resistant Bacteria Infection in Diabetic Foot PatientsMai BasionyNo ratings yet
- Adherence To Nucleos (T) Ide Analogue PDFDocument8 pagesAdherence To Nucleos (T) Ide Analogue PDFVirgo WNo ratings yet
- Evaluation of The Factors Influencing Adherence To ART in HIVAIDS Patients at Kampala International University Teaching Hospital Bushenyi DistrictDocument17 pagesEvaluation of The Factors Influencing Adherence To ART in HIVAIDS Patients at Kampala International University Teaching Hospital Bushenyi DistrictKIU PUBLICATION AND EXTENSIONNo ratings yet
- AIDS Research and TherapyDocument10 pagesAIDS Research and TherapyDjamal ToeNo ratings yet
- Caro-Vega Et Al. - 2021 - Suppression Among Antiretroviral Treatment-Naïve and Experienced Persons Participating in A Nationally RepresDocument10 pagesCaro-Vega Et Al. - 2021 - Suppression Among Antiretroviral Treatment-Naïve and Experienced Persons Participating in A Nationally RepresferalaesNo ratings yet
- Influencing Factors To Adherence To ArvDocument8 pagesInfluencing Factors To Adherence To ArvOBIOMA LILIAN OKWUONUNo ratings yet
- Knowledge and Adherence To Antiretroviral Therapy Among Adult People Living With HIV/AIDS Treated in The Health Care Centers of The Association "Espoir Vie Togo" in Togo, West AfricaDocument7 pagesKnowledge and Adherence To Antiretroviral Therapy Among Adult People Living With HIV/AIDS Treated in The Health Care Centers of The Association "Espoir Vie Togo" in Togo, West AfricanazargafarNo ratings yet
- Viruses 16 00239Document18 pagesViruses 16 00239jhonny12321No ratings yet
- Researcharticle Open Access: Tigist EngdaDocument12 pagesResearcharticle Open Access: Tigist EngdasitiNo ratings yet
- Knowledge, Attitudes, and Practices of Bedside Nursing Staff PDFDocument4 pagesKnowledge, Attitudes, and Practices of Bedside Nursing Staff PDFwindysandy100% (1)
- Long Walk TBDocument3 pagesLong Walk TBdellanurainiNo ratings yet
- Journal of Global Pharma Technology: Pharmacoepidemiology of Antiretroviral Drugs in A Tertiary Care Teaching HospitalDocument7 pagesJournal of Global Pharma Technology: Pharmacoepidemiology of Antiretroviral Drugs in A Tertiary Care Teaching HospitalsonyekanugrahaNo ratings yet
- Centers For Disease Control and Prevention's Sexually Transmitted Diseases Infection GuidelinesDocument6 pagesCenters For Disease Control and Prevention's Sexually Transmitted Diseases Infection GuidelinesabhinavrautNo ratings yet
- Patient Reported BarriesDocument14 pagesPatient Reported Barriesdani catriaNo ratings yet
- Healthcare: A Systematic Review of Healthcare-Associated Infectious Organisms in Medical Radiation Science DepartmentsDocument14 pagesHealthcare: A Systematic Review of Healthcare-Associated Infectious Organisms in Medical Radiation Science DepartmentsArina Al-KhaqNo ratings yet
- Community Knowledge, Awareness and Attitudes Towards Antimicrobial Resistance in Qassim Region, Saudi ArabiaDocument9 pagesCommunity Knowledge, Awareness and Attitudes Towards Antimicrobial Resistance in Qassim Region, Saudi ArabiaIJAR JOURNALNo ratings yet
- 2017 Article 2875Document7 pages2017 Article 2875IFan Erian KurniawanNo ratings yet
- Systematic Review and Meta-AnalysisDocument11 pagesSystematic Review and Meta-AnalysisHabtamu WondifrawNo ratings yet
- Ofx 137Document7 pagesOfx 137Sheila Alcalde RNo ratings yet
- 2016 Antifungal Agent Full PDFDocument16 pages2016 Antifungal Agent Full PDFyeni novi yantiNo ratings yet
- Community Acquired Pneumonia In+childrenDocument4 pagesCommunity Acquired Pneumonia In+childrendai shujuanNo ratings yet
- Preventive Medicine Reports: Samuel R. Bunting, Brian A. Feinstein, Aniruddha Hazra, Neeral K. Sheth, Sarah S. GarberDocument9 pagesPreventive Medicine Reports: Samuel R. Bunting, Brian A. Feinstein, Aniruddha Hazra, Neeral K. Sheth, Sarah S. GarberKnowledge PepalaNo ratings yet
- The Effect of The E-Patuh Application On HIV/Aids Patients' Adherence in Consuming AntiretroviralDocument9 pagesThe Effect of The E-Patuh Application On HIV/Aids Patients' Adherence in Consuming AntiretroviralNeneng Aini KaruniawanNo ratings yet
- Policy Guidance On Drug-Susceptibility Testing (DST) of Second-Line Antituberculosis DrugsDocument20 pagesPolicy Guidance On Drug-Susceptibility Testing (DST) of Second-Line Antituberculosis DrugsrehanaNo ratings yet
- JurnalDocument7 pagesJurnalyenni elfiraNo ratings yet
- Cmar 12 4829Document11 pagesCmar 12 4829Ina MartianaNo ratings yet
- DR Akin Moses Chief Consultant & Head, Family Medicine, NationalDocument44 pagesDR Akin Moses Chief Consultant & Head, Family Medicine, Nationalayodeji78No ratings yet
- RujukanDocument2 pagesRujukanNurhidayah RamliNo ratings yet
- Global Snapshot 2018Document4 pagesGlobal Snapshot 2018sofiabloemNo ratings yet
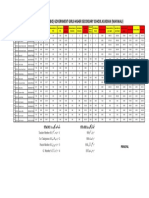
- Merit List Stis (Bio) Government Girls Higher Secondary School Kundian (Mianwali)Document1 pageMerit List Stis (Bio) Government Girls Higher Secondary School Kundian (Mianwali)Malik AsadNo ratings yet
- PSI INDIA - Will Balbir Pasha Help Fight AIDS: Target AudienceDocument2 pagesPSI INDIA - Will Balbir Pasha Help Fight AIDS: Target AudienceShambhawi SinhaNo ratings yet
- HIV in Mothers and Children: What's New?Document5 pagesHIV in Mothers and Children: What's New?VeronikaNo ratings yet
- 5 Myths About STDsDocument8 pages5 Myths About STDsThanh Bình ĐinhNo ratings yet
- Daftar PustakaDocument7 pagesDaftar PustakaAdilah RamadhaniNo ratings yet
- KAP SurveyDocument16 pagesKAP SurveyCortex PlussNo ratings yet
- 3 Konsep Terapi ARVDocument65 pages3 Konsep Terapi ARVkristinaNo ratings yet
- Worksho Pencegahan Dan Pengendalian Penyakit MonkeypoxDocument64 pagesWorksho Pencegahan Dan Pengendalian Penyakit MonkeypoxberiNo ratings yet
- NCM 112 - Sexually Transmitted Disease (STD)Document4 pagesNCM 112 - Sexually Transmitted Disease (STD)Cailah Sofia SelausoNo ratings yet
- Hiv/Aids Awareness: World Aids Day (1 Dec)Document31 pagesHiv/Aids Awareness: World Aids Day (1 Dec)RatneshNo ratings yet
- Filipino RRLDocument4 pagesFilipino RRLAndreNicoloGuloyNo ratings yet
- Sexual Health in ArmeniaDocument8 pagesSexual Health in ArmeniaJacques HamalianNo ratings yet
- Inventing The AIDS VirusDocument724 pagesInventing The AIDS VirusConventionalThinker94% (16)
- dm2023-0339 Reiteration On Providing Adherence Counseling and Employing Multi-Month Dispensing of Antiretroviral (ARV) Drugs For PLHIVDocument2 pagesdm2023-0339 Reiteration On Providing Adherence Counseling and Employing Multi-Month Dispensing of Antiretroviral (ARV) Drugs For PLHIVithran khoNo ratings yet
- HIV Dr. Suwanta RSUD WaledDocument58 pagesHIV Dr. Suwanta RSUD WaledTeddie RustendieNo ratings yet
- 143Document68 pages143Charles ChalimbaNo ratings yet
- Hiv Informative Genre FinalDocument9 pagesHiv Informative Genre Finalapi-510346047No ratings yet
- CXC Social Studies Sba 2023Document27 pagesCXC Social Studies Sba 2023David DillonNo ratings yet
- Philippine-Aids-Prevention-and-Control-Act Sample EssayDocument11 pagesPhilippine-Aids-Prevention-and-Control-Act Sample EssaySirhcmonne Jacob PosadasNo ratings yet
- Reproductive Tract Infection/Std Control ProgrammeDocument33 pagesReproductive Tract Infection/Std Control Programmeayushi rainaNo ratings yet
- Third-Line Antiretroviral Therapy in Africa: Effectiveness in A Southern African Retrospective Cohort StudyDocument7 pagesThird-Line Antiretroviral Therapy in Africa: Effectiveness in A Southern African Retrospective Cohort StudyPetros TemboNo ratings yet
- Doxy PEPDocument2 pagesDoxy PEPDoverocks7No ratings yet
- Hiv 101Document56 pagesHiv 101AIDSPhil100% (1)
- Analisis Faktor Risiko Penyakit HIV Berbasis Perilaku ManusiaDocument6 pagesAnalisis Faktor Risiko Penyakit HIV Berbasis Perilaku ManusiaPuriNo ratings yet
- UNAIDS Core Epidemiology Slides enDocument11 pagesUNAIDS Core Epidemiology Slides enTabarcea VitaliNo ratings yet
- Gorontalo ImsDocument18 pagesGorontalo ImsMuhammad FansyuriNo ratings yet
- HIV For NAPLEXDocument9 pagesHIV For NAPLEXtpatel0986100% (2)























































































Download as pdf or txt
You might also like
- International Journal of Infectious Diseases: SciencedirectDocument5 pagesInternational Journal of Infectious Diseases: SciencedirectMuh Syukriadi AnsarNo ratings yet
- The Role of a Pharmacist in the Analysis of Adherence Rates and Associated Factors in HIV-Patients Registered on Centralized Chronic Medicines Dispensing and Distribution (CCMDD) Programme in the Public Sector in South AfricaDocument11 pagesThe Role of a Pharmacist in the Analysis of Adherence Rates and Associated Factors in HIV-Patients Registered on Centralized Chronic Medicines Dispensing and Distribution (CCMDD) Programme in the Public Sector in South AfricaSabrina JonesNo ratings yet
- Viruses 14 02208Document16 pagesViruses 14 02208jhonny12321No ratings yet
- The HIV Care Continuum and HIV-1 Drug Resistance Among Female Sex Workers: A Key Population in Guinea-BissauDocument11 pagesThe HIV Care Continuum and HIV-1 Drug Resistance Among Female Sex Workers: A Key Population in Guinea-Bissautomasarino74No ratings yet
- Journal of Clinical Tuberculosis and Other Mycobacterial DiseasesDocument16 pagesJournal of Clinical Tuberculosis and Other Mycobacterial DiseasesIlna RamadhaniNo ratings yet
- Understanding The Gaps in DR TB Care Casc - 2020 - Journal of Clinical TuberculoDocument16 pagesUnderstanding The Gaps in DR TB Care Casc - 2020 - Journal of Clinical TuberculoKarina ChristantoNo ratings yet
- Therapeutic Drug Monitoring in Human Immunodeficiency Virus/Acquired Immunodeficiency SyndromeDocument3 pagesTherapeutic Drug Monitoring in Human Immunodeficiency Virus/Acquired Immunodeficiency SyndromeFransiskus Samuel RenaldiNo ratings yet
- s42269 022 00961 3Document9 pagess42269 022 00961 3Cliff Daniel DIANZOLE MOUNKANANo ratings yet
- Detectable Viral Load and Human Immuno Deficiency Drug ResistanceDocument11 pagesDetectable Viral Load and Human Immuno Deficiency Drug ResistanceFelistus KanjiraNo ratings yet
- Long-Acting Antiretrovirals: A New Era For The Management and Prevention of HIV InfectionDocument13 pagesLong-Acting Antiretrovirals: A New Era For The Management and Prevention of HIV InfectionRobles Murillo Carlos Eduardo Augusto 1FNo ratings yet
- Piaa 030Document10 pagesPiaa 030Suryadi LimardiNo ratings yet
- Effects of Adherence To Antiretroviral Therapy On Body Mass Index, Immunological and Virological Status of Nigerians Living With HIV/AIDSDocument4 pagesEffects of Adherence To Antiretroviral Therapy On Body Mass Index, Immunological and Virological Status of Nigerians Living With HIV/AIDSDavidNo ratings yet
- Journal Pone 0245498Document36 pagesJournal Pone 0245498Aklilu FelekeNo ratings yet
- Comparison of The Efficacy and Safety of 2 Different Antiretroviral Regimens in Tertiary Care Hospital: A Retrospective Observational StudyDocument5 pagesComparison of The Efficacy and Safety of 2 Different Antiretroviral Regimens in Tertiary Care Hospital: A Retrospective Observational StudyNarendranath SNo ratings yet
- Hiv 13 1111Document8 pagesHiv 13 1111Cliff Daniel DIANZOLE MOUNKANANo ratings yet
- Isoniazid Prophylaxis Highly Effective But UnderutDocument2 pagesIsoniazid Prophylaxis Highly Effective But Underutemilianoarteagagarcia11No ratings yet
- Adhearence GechoDocument9 pagesAdhearence Gechosinte beyuNo ratings yet
- Malaria Treatment-Seeking Behaviour and Its Associated FactorsDocument34 pagesMalaria Treatment-Seeking Behaviour and Its Associated FactorsDaniel BoibanNo ratings yet
- Knowledge, Attitudes, and Practices (KAP) of Healthcare Workers On Viral Hepatitis B and Its Vaccination in 12 Health Establishments in The Centre Region of CameroonDocument8 pagesKnowledge, Attitudes, and Practices (KAP) of Healthcare Workers On Viral Hepatitis B and Its Vaccination in 12 Health Establishments in The Centre Region of CameroonInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Lester 2010Document8 pagesLester 2010Riska Resty WasitaNo ratings yet
- s12879 021 06459 ZDocument11 pagess12879 021 06459 ZCliff Daniel DIANZOLE MOUNKANANo ratings yet
- Pone 0150849Document12 pagesPone 0150849yeremia imanuelNo ratings yet
- Research Article: Factors Affecting Compliance of Infection Control Measures Among Dental RadiographersDocument11 pagesResearch Article: Factors Affecting Compliance of Infection Control Measures Among Dental RadiographersPRADNJA SURYA PARAMITHANo ratings yet
- Role of Telepharmacy in Pharmacist Counselling To Coronavirus Disease 2019 Patients and Medication Dispensing ErrorsDocument10 pagesRole of Telepharmacy in Pharmacist Counselling To Coronavirus Disease 2019 Patients and Medication Dispensing ErrorsIndra Braja MaespatiNo ratings yet
- 1 s2.0 S2210803316300781 MainDocument8 pages1 s2.0 S2210803316300781 MainGilang Aji P. EmonNo ratings yet
- Dengvaxia VaccineDocument8 pagesDengvaxia VaccineBayek NgekekNo ratings yet
- Management of Antiretroviral Therapy With Boosted Protease Inhibitors-Darunavir/Ritonavir or Darunavir/CobicistatDocument36 pagesManagement of Antiretroviral Therapy With Boosted Protease Inhibitors-Darunavir/Ritonavir or Darunavir/Cobicistatnegru paulNo ratings yet
- Effectiveness of Outreach Clinical Mentoring On Retention in Care and Viral Suppression Among HIV Positive Young Persons On Art in North Central NigeriaDocument8 pagesEffectiveness of Outreach Clinical Mentoring On Retention in Care and Viral Suppression Among HIV Positive Young Persons On Art in North Central NigeriaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Journal Pone 0254890Document16 pagesJournal Pone 0254890muhammmad haris faisalNo ratings yet
- Khawcharoenporn2014 PDFDocument10 pagesKhawcharoenporn2014 PDFsinta belaNo ratings yet
- Comparative Exploration of Patient Related Factors That Influence Adherence To ART Among HIV Patients Attending Jinja Regional Referral Hospital.Document10 pagesComparative Exploration of Patient Related Factors That Influence Adherence To ART Among HIV Patients Attending Jinja Regional Referral Hospital.KIU PUBLICATION AND EXTENSIONNo ratings yet
- Patient-Centered Telehealth Solution For Observed Urine Collections in Substance Use Disorder Care Delivery During COVID-19 and BeyondDocument8 pagesPatient-Centered Telehealth Solution For Observed Urine Collections in Substance Use Disorder Care Delivery During COVID-19 and Beyondvovinda rujianaNo ratings yet
- ART Chapter One SubmissionDocument10 pagesART Chapter One SubmissionbstogarepiNo ratings yet
- Nomogram Model For Predicting The Risk of Multidrug-Resistant Bacteria Infection in Diabetic Foot PatientsDocument12 pagesNomogram Model For Predicting The Risk of Multidrug-Resistant Bacteria Infection in Diabetic Foot PatientsMai BasionyNo ratings yet
- Adherence To Nucleos (T) Ide Analogue PDFDocument8 pagesAdherence To Nucleos (T) Ide Analogue PDFVirgo WNo ratings yet
- Evaluation of The Factors Influencing Adherence To ART in HIVAIDS Patients at Kampala International University Teaching Hospital Bushenyi DistrictDocument17 pagesEvaluation of The Factors Influencing Adherence To ART in HIVAIDS Patients at Kampala International University Teaching Hospital Bushenyi DistrictKIU PUBLICATION AND EXTENSIONNo ratings yet
- AIDS Research and TherapyDocument10 pagesAIDS Research and TherapyDjamal ToeNo ratings yet
- Caro-Vega Et Al. - 2021 - Suppression Among Antiretroviral Treatment-Naïve and Experienced Persons Participating in A Nationally RepresDocument10 pagesCaro-Vega Et Al. - 2021 - Suppression Among Antiretroviral Treatment-Naïve and Experienced Persons Participating in A Nationally RepresferalaesNo ratings yet
- Influencing Factors To Adherence To ArvDocument8 pagesInfluencing Factors To Adherence To ArvOBIOMA LILIAN OKWUONUNo ratings yet
- Knowledge and Adherence To Antiretroviral Therapy Among Adult People Living With HIV/AIDS Treated in The Health Care Centers of The Association "Espoir Vie Togo" in Togo, West AfricaDocument7 pagesKnowledge and Adherence To Antiretroviral Therapy Among Adult People Living With HIV/AIDS Treated in The Health Care Centers of The Association "Espoir Vie Togo" in Togo, West AfricanazargafarNo ratings yet
- Viruses 16 00239Document18 pagesViruses 16 00239jhonny12321No ratings yet
- Researcharticle Open Access: Tigist EngdaDocument12 pagesResearcharticle Open Access: Tigist EngdasitiNo ratings yet
- Knowledge, Attitudes, and Practices of Bedside Nursing Staff PDFDocument4 pagesKnowledge, Attitudes, and Practices of Bedside Nursing Staff PDFwindysandy100% (1)
- Long Walk TBDocument3 pagesLong Walk TBdellanurainiNo ratings yet
- Journal of Global Pharma Technology: Pharmacoepidemiology of Antiretroviral Drugs in A Tertiary Care Teaching HospitalDocument7 pagesJournal of Global Pharma Technology: Pharmacoepidemiology of Antiretroviral Drugs in A Tertiary Care Teaching HospitalsonyekanugrahaNo ratings yet
- Centers For Disease Control and Prevention's Sexually Transmitted Diseases Infection GuidelinesDocument6 pagesCenters For Disease Control and Prevention's Sexually Transmitted Diseases Infection GuidelinesabhinavrautNo ratings yet
- Patient Reported BarriesDocument14 pagesPatient Reported Barriesdani catriaNo ratings yet
- Healthcare: A Systematic Review of Healthcare-Associated Infectious Organisms in Medical Radiation Science DepartmentsDocument14 pagesHealthcare: A Systematic Review of Healthcare-Associated Infectious Organisms in Medical Radiation Science DepartmentsArina Al-KhaqNo ratings yet
- Community Knowledge, Awareness and Attitudes Towards Antimicrobial Resistance in Qassim Region, Saudi ArabiaDocument9 pagesCommunity Knowledge, Awareness and Attitudes Towards Antimicrobial Resistance in Qassim Region, Saudi ArabiaIJAR JOURNALNo ratings yet
- 2017 Article 2875Document7 pages2017 Article 2875IFan Erian KurniawanNo ratings yet
- Systematic Review and Meta-AnalysisDocument11 pagesSystematic Review and Meta-AnalysisHabtamu WondifrawNo ratings yet
- Ofx 137Document7 pagesOfx 137Sheila Alcalde RNo ratings yet
- 2016 Antifungal Agent Full PDFDocument16 pages2016 Antifungal Agent Full PDFyeni novi yantiNo ratings yet
- Community Acquired Pneumonia In+childrenDocument4 pagesCommunity Acquired Pneumonia In+childrendai shujuanNo ratings yet
- Preventive Medicine Reports: Samuel R. Bunting, Brian A. Feinstein, Aniruddha Hazra, Neeral K. Sheth, Sarah S. GarberDocument9 pagesPreventive Medicine Reports: Samuel R. Bunting, Brian A. Feinstein, Aniruddha Hazra, Neeral K. Sheth, Sarah S. GarberKnowledge PepalaNo ratings yet
- The Effect of The E-Patuh Application On HIV/Aids Patients' Adherence in Consuming AntiretroviralDocument9 pagesThe Effect of The E-Patuh Application On HIV/Aids Patients' Adherence in Consuming AntiretroviralNeneng Aini KaruniawanNo ratings yet
- Policy Guidance On Drug-Susceptibility Testing (DST) of Second-Line Antituberculosis DrugsDocument20 pagesPolicy Guidance On Drug-Susceptibility Testing (DST) of Second-Line Antituberculosis DrugsrehanaNo ratings yet
- JurnalDocument7 pagesJurnalyenni elfiraNo ratings yet
- Cmar 12 4829Document11 pagesCmar 12 4829Ina MartianaNo ratings yet
- DR Akin Moses Chief Consultant & Head, Family Medicine, NationalDocument44 pagesDR Akin Moses Chief Consultant & Head, Family Medicine, Nationalayodeji78No ratings yet
- RujukanDocument2 pagesRujukanNurhidayah RamliNo ratings yet
- Global Snapshot 2018Document4 pagesGlobal Snapshot 2018sofiabloemNo ratings yet
- Merit List Stis (Bio) Government Girls Higher Secondary School Kundian (Mianwali)Document1 pageMerit List Stis (Bio) Government Girls Higher Secondary School Kundian (Mianwali)Malik AsadNo ratings yet
- PSI INDIA - Will Balbir Pasha Help Fight AIDS: Target AudienceDocument2 pagesPSI INDIA - Will Balbir Pasha Help Fight AIDS: Target AudienceShambhawi SinhaNo ratings yet
- HIV in Mothers and Children: What's New?Document5 pagesHIV in Mothers and Children: What's New?VeronikaNo ratings yet
- 5 Myths About STDsDocument8 pages5 Myths About STDsThanh Bình ĐinhNo ratings yet
- Daftar PustakaDocument7 pagesDaftar PustakaAdilah RamadhaniNo ratings yet
- KAP SurveyDocument16 pagesKAP SurveyCortex PlussNo ratings yet
- 3 Konsep Terapi ARVDocument65 pages3 Konsep Terapi ARVkristinaNo ratings yet
- Worksho Pencegahan Dan Pengendalian Penyakit MonkeypoxDocument64 pagesWorksho Pencegahan Dan Pengendalian Penyakit MonkeypoxberiNo ratings yet
- NCM 112 - Sexually Transmitted Disease (STD)Document4 pagesNCM 112 - Sexually Transmitted Disease (STD)Cailah Sofia SelausoNo ratings yet
- Hiv/Aids Awareness: World Aids Day (1 Dec)Document31 pagesHiv/Aids Awareness: World Aids Day (1 Dec)RatneshNo ratings yet
- Filipino RRLDocument4 pagesFilipino RRLAndreNicoloGuloyNo ratings yet
- Sexual Health in ArmeniaDocument8 pagesSexual Health in ArmeniaJacques HamalianNo ratings yet
- Inventing The AIDS VirusDocument724 pagesInventing The AIDS VirusConventionalThinker94% (16)
- dm2023-0339 Reiteration On Providing Adherence Counseling and Employing Multi-Month Dispensing of Antiretroviral (ARV) Drugs For PLHIVDocument2 pagesdm2023-0339 Reiteration On Providing Adherence Counseling and Employing Multi-Month Dispensing of Antiretroviral (ARV) Drugs For PLHIVithran khoNo ratings yet
- HIV Dr. Suwanta RSUD WaledDocument58 pagesHIV Dr. Suwanta RSUD WaledTeddie RustendieNo ratings yet
- 143Document68 pages143Charles ChalimbaNo ratings yet
- Hiv Informative Genre FinalDocument9 pagesHiv Informative Genre Finalapi-510346047No ratings yet
- CXC Social Studies Sba 2023Document27 pagesCXC Social Studies Sba 2023David DillonNo ratings yet
- Philippine-Aids-Prevention-and-Control-Act Sample EssayDocument11 pagesPhilippine-Aids-Prevention-and-Control-Act Sample EssaySirhcmonne Jacob PosadasNo ratings yet
- Reproductive Tract Infection/Std Control ProgrammeDocument33 pagesReproductive Tract Infection/Std Control Programmeayushi rainaNo ratings yet
- Third-Line Antiretroviral Therapy in Africa: Effectiveness in A Southern African Retrospective Cohort StudyDocument7 pagesThird-Line Antiretroviral Therapy in Africa: Effectiveness in A Southern African Retrospective Cohort StudyPetros TemboNo ratings yet
- Doxy PEPDocument2 pagesDoxy PEPDoverocks7No ratings yet
- Hiv 101Document56 pagesHiv 101AIDSPhil100% (1)
- Analisis Faktor Risiko Penyakit HIV Berbasis Perilaku ManusiaDocument6 pagesAnalisis Faktor Risiko Penyakit HIV Berbasis Perilaku ManusiaPuriNo ratings yet
- UNAIDS Core Epidemiology Slides enDocument11 pagesUNAIDS Core Epidemiology Slides enTabarcea VitaliNo ratings yet
- Gorontalo ImsDocument18 pagesGorontalo ImsMuhammad FansyuriNo ratings yet
- HIV For NAPLEXDocument9 pagesHIV For NAPLEXtpatel0986100% (2)