Download as pdf or txt
You might also like
- Sketchy Pharm RuntimesDocument5 pagesSketchy Pharm RuntimesAmin ValenciaNo ratings yet
- Checklist & Algoritma ACLSDocument16 pagesChecklist & Algoritma ACLSNadhif JovaldyNo ratings yet
- Neonatal Resuscitation ProgramDocument1 pageNeonatal Resuscitation ProgramWilma Yandan Bau67% (6)
- Advanced Cardiovascular Life SupportDocument43 pagesAdvanced Cardiovascular Life SupportGeraldine Marie SalvoNo ratings yet
- AclsDocument1 pageAclsJoice DasNo ratings yet
- Drug Study - MidazolamDocument2 pagesDrug Study - MidazolamKian HerreraNo ratings yet
- Bio Crisis - 2nd DayDocument4 pagesBio Crisis - 2nd DayaryanjimeraNo ratings yet
- Acls PDFDocument2 pagesAcls PDFKyrie Diosabeth TumbagaNo ratings yet
- Crashing PTDocument1 pageCrashing PTansylaeNo ratings yet
- Emcrit Airway Checklist 2013-02-05Document3 pagesEmcrit Airway Checklist 2013-02-05Kyra PoggenpoelNo ratings yet
- Simplified ACLS AlgorithmDocument1 pageSimplified ACLS AlgorithmBrianNo ratings yet
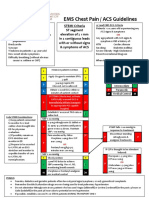
- EMS Chest Pain / ACS GuidelinesDocument1 pageEMS Chest Pain / ACS GuidelinesJuanaly BadiolaNo ratings yet
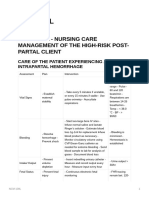
- NCM 109LDocument22 pagesNCM 109LMariah Alexis EncinaNo ratings yet
- Adult Cardiac Arrest Circular Algorithm: Monitor CPR QualityDocument1 pageAdult Cardiac Arrest Circular Algorithm: Monitor CPR QualityAlexis HospitalNo ratings yet
- Adult Cardiac Arrest Circular Algorithm: Monitor CPR QualityDocument1 pageAdult Cardiac Arrest Circular Algorithm: Monitor CPR QualityChris LeeNo ratings yet
- Drug Study: EpinephrineDocument5 pagesDrug Study: EpinephrineOmyl-Khayr M. SulogNo ratings yet
- RespDisord (PART B & C)Document4 pagesRespDisord (PART B & C)GraceNo ratings yet
- Persiapan Triage Primary Survey Resusitasi Adjunct Primary: By: RiswanDocument7 pagesPersiapan Triage Primary Survey Resusitasi Adjunct Primary: By: Riswanrudi mirinoNo ratings yet
- Ecg ReadingsDocument11 pagesEcg ReadingsAnton Laurenciana100% (5)
- PALSDocument4 pagesPALSwiraNo ratings yet
- With A Pulse and Poor Perfusion: Pediatric TachycardiaDocument1 pageWith A Pulse and Poor Perfusion: Pediatric TachycardiaIin-Ignasia Diahayujulindah Mujiman0% (1)
- Peri-Arrest ArrythmiaDocument14 pagesPeri-Arrest Arrythmiamohamed mowafeyNo ratings yet
- PRONE Position Wheezing Chest Retractions Grunt: - Chocking - Hacking/Barking Cough-Worse at NightDocument3 pagesPRONE Position Wheezing Chest Retractions Grunt: - Chocking - Hacking/Barking Cough-Worse at NightEben Ezar Dela CruzNo ratings yet
- Drug StudyDocument4 pagesDrug Studytaurus_gm27No ratings yet
- NCMB 312 Cu7Document5 pagesNCMB 312 Cu7Demierish DimaanoNo ratings yet
- General AnestheticDocument2 pagesGeneral AnestheticKirby AcobaNo ratings yet
- Laporan KematianDocument1 pageLaporan KematianIntan Robi'ahNo ratings yet
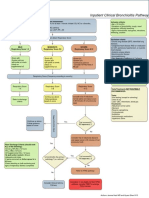
- Bronchiolitis Pathway InpatientDocument1 pageBronchiolitis Pathway Inpatientd'Agung NugrohoNo ratings yet
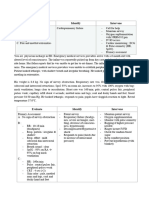
- Assessment Nursing Diagnosis Planning Intervention Rationale EvaluationDocument7 pagesAssessment Nursing Diagnosis Planning Intervention Rationale EvaluationEula ReyesNo ratings yet
- Albuterol or SalbutamolDocument1 pageAlbuterol or SalbutamolRyana Recar FerrerosNo ratings yet
- Roams Review of All Medical Subjects Pdfdrivecom PDF PDF FreeDocument31 pagesRoams Review of All Medical Subjects Pdfdrivecom PDF PDF FreeBiswajitNo ratings yet
- PharmaDocument3 pagesPharmaVinceNo ratings yet
- QRH 2-6 Bradycardia v1-1Document1 pageQRH 2-6 Bradycardia v1-1Baha MirzaeifarNo ratings yet
- Mind Maping MIDocument1 pageMind Maping MIimambiyono9728No ratings yet
- Any Up-Dates Are To Be Completed in Different Color Ink. The Student Is Expected To Document All Meds The Client Is Currently ReceivingDocument1 pageAny Up-Dates Are To Be Completed in Different Color Ink. The Student Is Expected To Document All Meds The Client Is Currently Receivinggeorgeloto12No ratings yet
- Airway ManagementDocument4 pagesAirway ManagementEllamae DerupeNo ratings yet
- Inpatientpathway PDFDocument2 pagesInpatientpathway PDFLuis Fernando SaraviaNo ratings yet
- AdenosineDocument2 pagesAdenosinegovind_soni_150% (1)
- Drug - Study VENTOLINDocument1 pageDrug - Study VENTOLINahrhicxNo ratings yet
- MEGACODEDocument6 pagesMEGACODESafety JNo ratings yet
- AlgorithmACLSBradycardiawithapulse PDFDocument1 pageAlgorithmACLSBradycardiawithapulse PDFjohndoe1995No ratings yet
- NCM 118 A Review Random FinalDocument3 pagesNCM 118 A Review Random FinalRosel Vivien EstoqueNo ratings yet
- Albuterol (Ventolin, Salbutamol)Document1 pageAlbuterol (Ventolin, Salbutamol)Jocelyn Rivera100% (1)
- Checklist & Algoritma ACLSDocument16 pagesChecklist & Algoritma ACLSNadhif JovaldyNo ratings yet
- NCPPPPPPPPPDocument4 pagesNCPPPPPPPPPHannah ChiuNo ratings yet
- Uued Coivd 19mgmt Guide For Publication 9 - 15 - 2020Document29 pagesUued Coivd 19mgmt Guide For Publication 9 - 15 - 2020JorgeNo ratings yet
- Drug StudyDocument5 pagesDrug Studyeduardbaldoz69No ratings yet
- Adult CardDocument1 pageAdult CardIvan MoralesNo ratings yet
- Algorithms of AHA 2020Document23 pagesAlgorithms of AHA 2020Emirhan llkhanNo ratings yet
- Pharmacology in NursingDocument1 pagePharmacology in NursingJessa Mae Barquilla100% (1)
- Slide Dr. Irene OS Eria 24 Juni 2021Document39 pagesSlide Dr. Irene OS Eria 24 Juni 2021wawanNo ratings yet
- Stress Eco and Eco ReportDocument4 pagesStress Eco and Eco ReportguptarichaandassociatesNo ratings yet
- Care PlanDocument20 pagesCare Planapi-490235704No ratings yet
- Medschool AnestheticsDocument4 pagesMedschool AnestheticsJustin HulinNo ratings yet
- Emergency DrugsDocument75 pagesEmergency DrugsQuinonez Anna MarieNo ratings yet
- (Issues and Orders To Cover) : - DyspneaDocument1 page(Issues and Orders To Cover) : - DyspneaAngelNo ratings yet
- 116 Prelim ElearningDocument10 pages116 Prelim ElearningJonathan MangawiliNo ratings yet
- Drug Study: Propofol: CNS Depressants: AdditiveDocument5 pagesDrug Study: Propofol: CNS Depressants: AdditiveShara Lailanie A. AzisNo ratings yet
- COMPRE - MODULE 4 (Pharmacology and Toxicology) : Attempt ReviewDocument40 pagesCOMPRE - MODULE 4 (Pharmacology and Toxicology) : Attempt ReviewLance RafaelNo ratings yet
- Metformin: Its Botanical Background: Practical Diabetes International April 2004Document4 pagesMetformin: Its Botanical Background: Practical Diabetes International April 2004made dwi novitasariNo ratings yet
- An Overview of Behavioral Disorders and Its Therapeutic Management in Dogs and CatsDocument12 pagesAn Overview of Behavioral Disorders and Its Therapeutic Management in Dogs and CatsDr N B ShridharNo ratings yet
- PDF Drug Induced Ocular Side Effects Clinical Ocular Toxicology 8Th Edition Frederick T Fraunfelder Ebook Full ChapterDocument53 pagesPDF Drug Induced Ocular Side Effects Clinical Ocular Toxicology 8Th Edition Frederick T Fraunfelder Ebook Full Chaptermargery.taylor882100% (4)
- Daftar ObatDocument3 pagesDaftar ObatLusia SeptianiNo ratings yet
- Guía Médica COMECOOP 07-11-2023Document2 pagesGuía Médica COMECOOP 07-11-2023braulio.a.b12No ratings yet
- Quiz 8 To 46Document7 pagesQuiz 8 To 46JhayneNo ratings yet
- Evaluation of Cyto-Toxic Potential of Aqua Distillate of Rosa Damascena Mill Using Brine Shrimp Lethality AssayDocument4 pagesEvaluation of Cyto-Toxic Potential of Aqua Distillate of Rosa Damascena Mill Using Brine Shrimp Lethality AssayDara Rustri ArdanaNo ratings yet
- Sapc Guide Line 2018Document38 pagesSapc Guide Line 2018Sabb12 Pat12No ratings yet
- Proton Pump Inhibitors, Adverse Events and Increased Risk of MortalityDocument36 pagesProton Pump Inhibitors, Adverse Events and Increased Risk of MortalityMohammad Mahmudur RahmanNo ratings yet
- Clinical ToxicologyDocument36 pagesClinical ToxicologyMuhammad FawadNo ratings yet
- Drug Study On EPINEPHRINEDocument6 pagesDrug Study On EPINEPHRINEshadow gonzalezNo ratings yet
- 603-Article Text-1341-1-10-20200925Document4 pages603-Article Text-1341-1-10-20200925Maria Valentina Peñaranda GarciaNo ratings yet
- Atorvastatin Patient LeafletDocument8 pagesAtorvastatin Patient LeafletKrupali TrivediNo ratings yet
- A Review On Oral Mucosal Drug Delivery SystemDocument8 pagesA Review On Oral Mucosal Drug Delivery SystemPharmacognosy JournalNo ratings yet
- Lista Me Cmimet e Barnave Jo Te Rimbursueshme 2014, 17feb2014Document340 pagesLista Me Cmimet e Barnave Jo Te Rimbursueshme 2014, 17feb2014Endri RamadaniNo ratings yet
- Mood DisordersDocument78 pagesMood Disorderspawan_sharma_55No ratings yet
- Harrison Care StudyDocument58 pagesHarrison Care Studygideon A. owusuNo ratings yet
- Spreading 6 Mar 2020Document792 pagesSpreading 6 Mar 2020resiNo ratings yet
- Isotonicity Adjustment Methods-2020 PDFDocument22 pagesIsotonicity Adjustment Methods-2020 PDFHisham GhanemNo ratings yet
- Assessment 8Document3 pagesAssessment 8Dianne LarozaNo ratings yet
- Our Lady of Fatima UniversityDocument15 pagesOur Lady of Fatima UniversityVincent BustamanteNo ratings yet
- PHAR 7633 Chapter 15 Multiple Oral Dose Administration: CP EquationDocument4 pagesPHAR 7633 Chapter 15 Multiple Oral Dose Administration: CP EquationSonia BaruaNo ratings yet
- 1 s2.0 S2405844024060286 MainDocument9 pages1 s2.0 S2405844024060286 MainSavaNo ratings yet
- COVID 19 Ayurveda Project Concept Paper DR Palitha SerasingheDocument8 pagesCOVID 19 Ayurveda Project Concept Paper DR Palitha SerasingheRajeshwari JadhavNo ratings yet
- Online Thrilokyavijaya Book PDF Version 1 PDFDocument352 pagesOnline Thrilokyavijaya Book PDF Version 1 PDFdanudmw0% (1)
- ClinicalDocument5 pagesClinicalMary Hope BacutaNo ratings yet
- Transdermal Drug Delivery System1Document38 pagesTransdermal Drug Delivery System1shobhitNo ratings yet
- Review: Theodore M. Sievers, Bernard M. Kubak and Annie Wong-BeringerDocument15 pagesReview: Theodore M. Sievers, Bernard M. Kubak and Annie Wong-BeringerRazzak CoolNo ratings yet