Download as pdf or txt
You might also like
- Altman 2017Document9 pagesAltman 2017Sílvia BastosNo ratings yet
- Clinico-Epidemiological Profile and Predictors of Outcome in Children With Diphtheria: A Study From Northern IndiaDocument6 pagesClinico-Epidemiological Profile and Predictors of Outcome in Children With Diphtheria: A Study From Northern IndiamariaprincesitaNo ratings yet
- Pertussis VaccinesDocument7 pagesPertussis VaccinesNur SulistiyaningsihNo ratings yet
- Varicella Vaccine Effectiveness Over 10 Years in Australia - 2019 - Journal ofDocument6 pagesVaricella Vaccine Effectiveness Over 10 Years in Australia - 2019 - Journal ofNihad MalikzadeNo ratings yet
- Swine Enteric Coronavirus Disease - A Review of 4 Years With Porcine Epidemic Diarrhoea Virus and Porcine Deltacoronavirus in The United States and CanadaDocument16 pagesSwine Enteric Coronavirus Disease - A Review of 4 Years With Porcine Epidemic Diarrhoea Virus and Porcine Deltacoronavirus in The United States and CanadaJuan Daniel Hernandez ValenzuelaNo ratings yet
- 2020 Aahaa Afp Feline Vaccination GuidelinesDocument17 pages2020 Aahaa Afp Feline Vaccination GuidelinesJeff WyattNo ratings yet
- 2022 Aaha Canine Vaccinations GuidelinesDocument18 pages2022 Aaha Canine Vaccinations Guidelinesarumugamks7628No ratings yet
- A Multicenter Point Prevalence Survey of Antibiotic Use in Haiti Juneaugust 2019 Findings and ImplicationsDocument2 pagesA Multicenter Point Prevalence Survey of Antibiotic Use in Haiti Juneaugust 2019 Findings and ImplicationsMentor Ali Ber LucienNo ratings yet
- Rotavirus Vaccines: Targeting The Developing World: SupplementarticleDocument7 pagesRotavirus Vaccines: Targeting The Developing World: SupplementarticleAbigailNo ratings yet
- Community Acquired Pneumonia In+childrenDocument4 pagesCommunity Acquired Pneumonia In+childrendai shujuanNo ratings yet
- Animal Models and Antibody Assays For Evaluating Candidate SARS Vaccines: Summary of A Technical Meeting 25-26 August 2005, London, UKDocument10 pagesAnimal Models and Antibody Assays For Evaluating Candidate SARS Vaccines: Summary of A Technical Meeting 25-26 August 2005, London, UKIon CorbuNo ratings yet
- Bulletin PDFDocument5 pagesBulletin PDFhasanbatoolNo ratings yet
- Giardia Prevalencia Mundial 2015 MetadataDocument22 pagesGiardia Prevalencia Mundial 2015 MetadataCelua Annette Sierra JananiaNo ratings yet
- Global prevalence of varicella-associated complicationsDocument25 pagesGlobal prevalence of varicella-associated complicationsluis sanchezNo ratings yet
- Vaccine: Parveen Fathima, Thomas L. Snelling, Robyn A. GibbsDocument6 pagesVaccine: Parveen Fathima, Thomas L. Snelling, Robyn A. GibbsAhmad Harissul IbadNo ratings yet
- Original Article - EnterococcusDocument7 pagesOriginal Article - EnterococcusQworldNo ratings yet
- BJC 2017154Document8 pagesBJC 2017154Altair CamargoNo ratings yet
- Newly Identified Viruses in Human Gastroenteritis: Espid R RDocument4 pagesNewly Identified Viruses in Human Gastroenteritis: Espid R RArianne LasamNo ratings yet
- Vijay 2018Document6 pagesVijay 2018Rabiatul 'raney' AdawiyahNo ratings yet
- 4) Respiratory Disease Diagnostics of Cattle CCCDocument8 pages4) Respiratory Disease Diagnostics of Cattle CCCCamilo Celis GarciaNo ratings yet
- Review ArticleDocument8 pagesReview ArticleIdmNo ratings yet
- Ijccm 26 717Document6 pagesIjccm 26 717RonakhNo ratings yet
- Transbounding Emerging Dis - 2020 - Dee - The Risk of Viral Transmission in Feed What Do We Know What Do We DoDocument7 pagesTransbounding Emerging Dis - 2020 - Dee - The Risk of Viral Transmission in Feed What Do We Know What Do We DoTee tee buoNo ratings yet
- Effects of Adherence To Antiretroviral Therapy On Body Mass Index, Immunological and Virological Status of Nigerians Living With HIV/AIDSDocument4 pagesEffects of Adherence To Antiretroviral Therapy On Body Mass Index, Immunological and Virological Status of Nigerians Living With HIV/AIDSDavidNo ratings yet
- Efficiency of Web Application and Spaced Repetition Algorithms As An Aid in Preparing To Practical Examination of HistologyDocument2 pagesEfficiency of Web Application and Spaced Repetition Algorithms As An Aid in Preparing To Practical Examination of HistologyduffuchimpsNo ratings yet
- Nej Mo A 0807381Document12 pagesNej Mo A 0807381Mildred MontNo ratings yet
- Consensus On The Rational Use of Antithrombotics in Veterinary Critical Care (CURATIVE) Domain 6Document61 pagesConsensus On The Rational Use of Antithrombotics in Veterinary Critical Care (CURATIVE) Domain 6BiancaNo ratings yet
- 1 s2.0 S0264410X21003091 MainDocument11 pages1 s2.0 S0264410X21003091 MainLixia WeiNo ratings yet
- Knowledge, Attitude & Practice On Human Papillomavirus Vaccination: A Cross-Sectional Study Among Healthcare ProvidersDocument9 pagesKnowledge, Attitude & Practice On Human Papillomavirus Vaccination: A Cross-Sectional Study Among Healthcare ProvidersHari PrasathNo ratings yet
- Jurnal Home Care 5Document4 pagesJurnal Home Care 5Aida MawaddahNo ratings yet
- 16859604Document8 pages16859604Brent DoolanNo ratings yet
- Biomarcadores Parvo 2013Document7 pagesBiomarcadores Parvo 2013María JesúsNo ratings yet
- Risk Assessment of Hepatitis B Patients of Northern Areas of Pakistan: A Case Control StudyDocument3 pagesRisk Assessment of Hepatitis B Patients of Northern Areas of Pakistan: A Case Control StudyDr Alamzeb JadoonNo ratings yet
- This Content Downloaded From 85.186.63.198 On Wed, 29 Sep 2021 09:36:56 UTCDocument26 pagesThis Content Downloaded From 85.186.63.198 On Wed, 29 Sep 2021 09:36:56 UTCKollar RolandNo ratings yet
- Sciencedirect: A B A C A D A EDocument2 pagesSciencedirect: A B A C A D A EBrayanTrujilloNo ratings yet
- Diphtheria Ay GhatsarpaDocument6 pagesDiphtheria Ay GhatsarpamskchoudhuriNo ratings yet
- Safety Surveillance of Diphtheria and Tetanus Toxoids and Acellular Pertussis (Dtap) VaccinesDocument9 pagesSafety Surveillance of Diphtheria and Tetanus Toxoids and Acellular Pertussis (Dtap) VaccinesHansley Templeton CookNo ratings yet
- A Study of Typhoid Fever in Five Asian Countries: Disease Burden and Implications For ControlsDocument4 pagesA Study of Typhoid Fever in Five Asian Countries: Disease Burden and Implications For ControlsPutu SuartiniNo ratings yet
- Ped Infect Disease Jr. 2023Document4 pagesPed Infect Disease Jr. 2023cdsaludNo ratings yet
- Efficacy of A Tetravalent Dengue Vaccine in Healthy Children and AdolescentsDocument11 pagesEfficacy of A Tetravalent Dengue Vaccine in Healthy Children and AdolescentsRildo Pretelt AlvárezNo ratings yet
- GammaglobulinaDocument7 pagesGammaglobulinaIván Gustavo Magaña CeballosNo ratings yet
- Research Article: Risk Factors and Prevention Strategies of Nosocomial Infection in Geriatric PatientsDocument6 pagesResearch Article: Risk Factors and Prevention Strategies of Nosocomial Infection in Geriatric Patientschristian demasabuNo ratings yet
- Pessoa e Silva2019Document8 pagesPessoa e Silva2019blendam.ferreiraNo ratings yet
- Companion Animal Parasitology: A Clinical Perspective: Peter J. IrwinDocument13 pagesCompanion Animal Parasitology: A Clinical Perspective: Peter J. IrwinAngela SanchezNo ratings yet
- The Pet Vaccine Controversy: Are Pets Over-Vaccinated? Literature ReviewDocument13 pagesThe Pet Vaccine Controversy: Are Pets Over-Vaccinated? Literature ReviewJharmaineNo ratings yet
- 200 Supplement - 1 S9Document7 pages200 Supplement - 1 S9Kollar RolandNo ratings yet
- Uso Da EpidemiologiaDocument6 pagesUso Da EpidemiologiaRafael NicolinoNo ratings yet
- Journal Gerontik 1Document11 pagesJournal Gerontik 1AgUnk MancuNianNo ratings yet
- Vaccines: Frequency of Adverse Events Following Q Fever Immunisation in Young AdultsDocument13 pagesVaccines: Frequency of Adverse Events Following Q Fever Immunisation in Young AdultslilahgreenyNo ratings yet
- Viruses 11 01155 v2Document20 pagesViruses 11 01155 v2Daniela Angel CortesNo ratings yet
- Epidemiology of Invasive Early Onset Neonatal SepsisDocument11 pagesEpidemiology of Invasive Early Onset Neonatal SepsisLucas SalgadoNo ratings yet
- Nejm VaricellaDocument9 pagesNejm VaricellaadityailhamNo ratings yet
- 139683-Article Text-372650-1-10-20160718Document9 pages139683-Article Text-372650-1-10-20160718MATTHEW JALOWE MACARANASNo ratings yet
- Sepsis Proposal1Document34 pagesSepsis Proposal1Appiah Peter OforiNo ratings yet
- Preventive Veterinary Medicine: A. Wiseman, E.M. Berman, E. KlementDocument6 pagesPreventive Veterinary Medicine: A. Wiseman, E.M. Berman, E. KlementSyabillaNo ratings yet
- Jurnal 1Document6 pagesJurnal 1Rey M FakhruryNo ratings yet
- Vital Sign Predictors of Severe InfluenzaDocument11 pagesVital Sign Predictors of Severe InfluenzaDesiska PriciliaNo ratings yet
- A Critical Review Evaluation of The Efficacy of Covid19 Vaccines in EnglandDocument14 pagesA Critical Review Evaluation of The Efficacy of Covid19 Vaccines in EnglandvalgurNo ratings yet
- Bloodstream Infections in Hospitalized Children: Epidemiology and Antimicrobial SusceptibilitiesDocument4 pagesBloodstream Infections in Hospitalized Children: Epidemiology and Antimicrobial SusceptibilitiesrasioputraNo ratings yet
- The Vaccine Handbook: A Practical Guide for Clinicians, Twelfth EditionFrom EverandThe Vaccine Handbook: A Practical Guide for Clinicians, Twelfth EditionNo ratings yet
- IS.6 HypersensitivityDocument4 pagesIS.6 HypersensitivityDANIELLA LOMA CAPONPONNo ratings yet
- 5 Paragraph Expository Essay OutlineDocument3 pages5 Paragraph Expository Essay Outlineb71bpjha100% (2)
- Colorectal Carcinoma SurgeryDocument19 pagesColorectal Carcinoma SurgeryDaanishNo ratings yet
- Soc. Sci. 412: Understanding Human BehaviorDocument20 pagesSoc. Sci. 412: Understanding Human BehaviorClancy HernandezNo ratings yet
- Lesson 1 The Basics of First AidDocument70 pagesLesson 1 The Basics of First AidDJ JoeNo ratings yet
- Clostridium - Botulinum.Document26 pagesClostridium - Botulinum.tummalapalli venkateswara rao100% (1)
- Kedren Drug Study.2Document10 pagesKedren Drug Study.2Kedren Kent JawoodNo ratings yet
- EBRSR Handbook Chapter 5 - Rehab of Cognitive Impairment 2020Document100 pagesEBRSR Handbook Chapter 5 - Rehab of Cognitive Impairment 2020anjelikaNo ratings yet
- Long Case OrthopaedicDocument24 pagesLong Case OrthopaedicSyimah UmarNo ratings yet
- MedSurg NeuroDocument8 pagesMedSurg NeuroZachary T Hall100% (1)
- Department of Microbiology Sanjay Gandhi Post Graduate Institute of Medical SciencesDocument48 pagesDepartment of Microbiology Sanjay Gandhi Post Graduate Institute of Medical SciencesMaster PrintersNo ratings yet
- Conversion Disorder, Functional Neurological Symptom Disorder, and Chronic Pain - Comorbidity, Assessment, and TreatmentDocument10 pagesConversion Disorder, Functional Neurological Symptom Disorder, and Chronic Pain - Comorbidity, Assessment, and TreatmentViviana CalderónNo ratings yet
- Apa Itu MengikDocument2 pagesApa Itu MengikAmy Tryabto ArifinNo ratings yet
- Cracked Tooth Syndrome. Part 1 Aetiology and DiagnosisDocument17 pagesCracked Tooth Syndrome. Part 1 Aetiology and Diagnosisfloressam2000No ratings yet
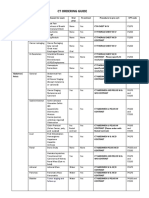
- CT Ordering Guide: Tumor Staging and Follow UpDocument2 pagesCT Ordering Guide: Tumor Staging and Follow UpanonNo ratings yet
- Morning Report: Dr. Dikara WS Maulidy, SP - PDDocument24 pagesMorning Report: Dr. Dikara WS Maulidy, SP - PDBethari Abi SafitriNo ratings yet
- Ketamine Psychedelic Psychotherapy: Focus On Its Pharmacology PHDocument59 pagesKetamine Psychedelic Psychotherapy: Focus On Its Pharmacology PHMartin Girard100% (1)
- LymphomaDocument3 pagesLymphomaMaya GoldbergerNo ratings yet
- Hubungan Kadar Interleukin 6 Dan Interleukin 10 Serum Pada Pasien Cedera Otak Berat Akibat TraumaDocument9 pagesHubungan Kadar Interleukin 6 Dan Interleukin 10 Serum Pada Pasien Cedera Otak Berat Akibat TraumaanggiNo ratings yet
- Ascites: DR Mohammed HussienDocument86 pagesAscites: DR Mohammed Hussienابراهيم عبداللهNo ratings yet
- AOCMF Brochure ISS5 A4 04 LRDocument16 pagesAOCMF Brochure ISS5 A4 04 LRDea Alberta SNo ratings yet
- Medical Immunology, 7th Edition PDFDocument479 pagesMedical Immunology, 7th Edition PDFoswaldo bigottNo ratings yet
- BOBATHDocument10 pagesBOBATHCatherine A.No ratings yet
- Post Operative Visit ReportDocument10 pagesPost Operative Visit ReportMARIA CHARMIN M. MEJIANo ratings yet
- Chmielewski ChapmanDocument3 pagesChmielewski Chapmanclinpsy.subsNo ratings yet
- Association Food Allergy Dried Fish Complex Regional Pain SyndromeDocument5 pagesAssociation Food Allergy Dried Fish Complex Regional Pain SyndromeSSR-IIJLS JournalNo ratings yet
- Modulo 200Document2 pagesModulo 200suso73No ratings yet
- (Groub 7) ST - Vincentius A Paulo (RKZ) SurabayaDocument7 pages(Groub 7) ST - Vincentius A Paulo (RKZ) SurabayaHeni RahayaanNo ratings yet
- Organization of Dominican-Haitian Cooperation Ocdh: "For The Sake of Haiti" Relief Concert February 5, 2010Document29 pagesOrganization of Dominican-Haitian Cooperation Ocdh: "For The Sake of Haiti" Relief Concert February 5, 2010stealphNo ratings yet
- Behavioral Disorders in Children...Document3 pagesBehavioral Disorders in Children...Abhishek1789No ratings yet