Download as pdf or txt
You might also like
- The A.S.P.E.N. Adult Nutrition Support Core CurriculumDocument740 pagesThe A.S.P.E.N. Adult Nutrition Support Core CurriculumAIMANIBRAHIM82100% (3)
- Exam MaterialsDocument4 pagesExam MaterialsDr-Usman KhanNo ratings yet
- Neonatal Parenteral and Enteral NutritionDocument23 pagesNeonatal Parenteral and Enteral NutritionPrimadiati Nickyta Sari100% (1)
- Policy For Exemption From Assessment and Examination FinalDocument28 pagesPolicy For Exemption From Assessment and Examination FinalGloria JaisonNo ratings yet
- Social Media Ethics Case StudyDocument20 pagesSocial Media Ethics Case StudyHanah100% (3)
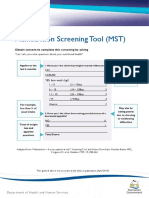
- Malnutrition Screening Tool (MST) : Obtain Consent To Complete This Screening by AskingDocument2 pagesMalnutrition Screening Tool (MST) : Obtain Consent To Complete This Screening by AskingAku dienaNo ratings yet
- Master Prospectus Autumn-2019Document97 pagesMaster Prospectus Autumn-2019chancher jee50% (2)
- Clinical Guideline: Enteral Feeding - Iron Supplementation: Neonatal Clinical Oversight GroupDocument12 pagesClinical Guideline: Enteral Feeding - Iron Supplementation: Neonatal Clinical Oversight GroupStphn WllngtnNo ratings yet
- Network PNguidleines FINALmay 2017Document17 pagesNetwork PNguidleines FINALmay 2017NguyễnĐứcThiệnNo ratings yet
- Infant Food: Caloric RequirementsDocument9 pagesInfant Food: Caloric Requirementsakskun57No ratings yet
- Postdischarge Nutritional TXDocument27 pagesPostdischarge Nutritional TXPaulina BangunNo ratings yet
- Total Parenteral NutritionDocument32 pagesTotal Parenteral Nutritionlordoftheweb100% (13)
- Gaps ProtocolDocument3 pagesGaps ProtocolVíctor Valdez100% (2)
- Glutaric Aciduria Type 1 (GA1) Dietetic Management PathwayDocument7 pagesGlutaric Aciduria Type 1 (GA1) Dietetic Management PathwayMoroianu Irina-GabrielaNo ratings yet
- Enteral Feeding GuidelinesDocument15 pagesEnteral Feeding GuidelinesAnonymous rDD9I2No ratings yet
- LIPO RED Product Data SheetDocument2 pagesLIPO RED Product Data SheetRich CarrNo ratings yet
- Zinc Sulfate: Drug Information: Pharmacologic CategoryDocument5 pagesZinc Sulfate: Drug Information: Pharmacologic CategoryVictoria Eliza InguilloNo ratings yet
- Feeding of Low Birth Weight and Preterm Babies PG - MHOMCC 6Document4 pagesFeeding of Low Birth Weight and Preterm Babies PG - MHOMCC 6heavenjot5911No ratings yet
- Enteral Feeding of PretermDocument9 pagesEnteral Feeding of PretermanuNo ratings yet
- smoflipidinf(4)Document13 pagessmoflipidinf(4)AndreaNo ratings yet
- Nutritional SupplementsDocument4 pagesNutritional SupplementsBiciin MarianNo ratings yet
- Vitalipid N PIDocument7 pagesVitalipid N PInieken proboratriNo ratings yet
- TPN Basics For The Hospital - RalphDocument54 pagesTPN Basics For The Hospital - RalphJayrine MonteroNo ratings yet
- Vitamin B Complex: By, Dr. Priyanga. P (Part I) Department of PaediatricsDocument41 pagesVitamin B Complex: By, Dr. Priyanga. P (Part I) Department of PaediatricsPRIYANGA. PNo ratings yet
- 2.vitamin ADocument20 pages2.vitamin AdrmaseerkhanNo ratings yet
- Pure & Essential Advanced Multivitamin & Minerals - A Nutritionist's GuideDocument4 pagesPure & Essential Advanced Multivitamin & Minerals - A Nutritionist's GuidejitenparekhNo ratings yet
- Short Guide Clinical NutritionDocument30 pagesShort Guide Clinical Nutritiontopiq100% (1)
- Parenteral and Enteral Nutrition in NeonatesDocument22 pagesParenteral and Enteral Nutrition in NeonatesStrept PneumoniaNo ratings yet
- Adult Enteral FormulasDocument2 pagesAdult Enteral FormulasMaulidatul Khasanah New100% (1)
- Nutrition Management Premie NashDocument49 pagesNutrition Management Premie NashathaNo ratings yet
- NUTRITION IN THE PRETERM AND SGA INFANTS/ Term Neonates/Children/Athletes-Dr. Ramolete Feb 5, 2014Document6 pagesNUTRITION IN THE PRETERM AND SGA INFANTS/ Term Neonates/Children/Athletes-Dr. Ramolete Feb 5, 2014Monique Angela Turingan GanganNo ratings yet
- Wayne Paeds Procedures 179Document221 pagesWayne Paeds Procedures 179GingerNo ratings yet
- Pedi Math Packet 2016-2017-1Document26 pagesPedi Math Packet 2016-2017-1NursyNurseNo ratings yet
- Ferrous Sulphate NeomedDocument3 pagesFerrous Sulphate NeomedShuaib KauchaliNo ratings yet
- Total Parenteral NutritionDocument9 pagesTotal Parenteral NutritionsaravananNo ratings yet
- Infant Nutrition 101: Amanda Mcmurray Registered Dietitian PediatricsDocument21 pagesInfant Nutrition 101: Amanda Mcmurray Registered Dietitian PediatricsxxpixiexxNo ratings yet
- NDT Exercise No.2 For BSN 2Document20 pagesNDT Exercise No.2 For BSN 2Celline Isabelle ReyesNo ratings yet
- Formula Choice 2022 - Dr. YogaDocument36 pagesFormula Choice 2022 - Dr. YogarosaliadesiNo ratings yet
- Enteral Nutrition and Nutraceutics - OH - 06 2012Document31 pagesEnteral Nutrition and Nutraceutics - OH - 06 2012irmaNo ratings yet
- JG College of Nursing, AhmedabadDocument13 pagesJG College of Nursing, AhmedabadVinayak Srivastava100% (1)
- Nutrition Bio f4Document12 pagesNutrition Bio f4is1977No ratings yet
- Paediatric Pam I DR On Ate IV MonographDocument2 pagesPaediatric Pam I DR On Ate IV MonographDouglas MutenyoNo ratings yet
- Session 3Document9 pagesSession 3SandyNo ratings yet
- Formulas and Fortifiers For Premature and Low Birth Weight InfantsDocument2 pagesFormulas and Fortifiers For Premature and Low Birth Weight InfantsShuaib KauchaliNo ratings yet
- Nutritional and Nutritional RequirementsDocument25 pagesNutritional and Nutritional RequirementsCLEMENTNo ratings yet
- Presented By-: Bibhu Prasad Sahu Rupsy Diya Saha Hitesh Khatua Arpit Patel Prith Vi Sena JasDocument47 pagesPresented By-: Bibhu Prasad Sahu Rupsy Diya Saha Hitesh Khatua Arpit Patel Prith Vi Sena JasKrishNo ratings yet
- Nutrition in The High Risk NeonatesDocument41 pagesNutrition in The High Risk NeonatesJohanna LomuljoNo ratings yet
- Parenteral and Enteral Nutrition in NeonateDocument22 pagesParenteral and Enteral Nutrition in NeonateAnonymous N2PHMnTIYLNo ratings yet
- The Firm ProtocolDocument5 pagesThe Firm ProtocolspshekarNo ratings yet
- The Food and Supplement Guide For The Coronavirus Version 7Document59 pagesThe Food and Supplement Guide For The Coronavirus Version 7alexpla37No ratings yet
- NICU Resident Manual Chapter 3 Nutiriton 2013Document17 pagesNICU Resident Manual Chapter 3 Nutiriton 2013kurniawatiNo ratings yet
- CHN1 Lec Session #16 SASDocument8 pagesCHN1 Lec Session #16 SASJhanna Mae BalbonNo ratings yet
- Neonatal Parenteral and Enteral Nutrition: A Resource Guide For The Student and Novice Neonatal Nurse PractitionerDocument23 pagesNeonatal Parenteral and Enteral Nutrition: A Resource Guide For The Student and Novice Neonatal Nurse PractitionerMOHAMMED ALMAJEDNo ratings yet
- Neonatal TPN: Dr. Fahad Al-AqlDocument10 pagesNeonatal TPN: Dr. Fahad Al-AqlAnonymous 9dVZCnTXSNo ratings yet
- 47 TPNDocument7 pages47 TPNKhor Chin PooNo ratings yet
- 2nd Vitamin K Prophylaxis in Newborn Babies Guide For GPsDocument2 pages2nd Vitamin K Prophylaxis in Newborn Babies Guide For GPsDr Mahmoud MesbahNo ratings yet
- Wayne Senior Paeds NotesDocument176 pagesWayne Senior Paeds NotesGingerNo ratings yet
- A1. Breastfeeding and General Feeding PDFDocument5 pagesA1. Breastfeeding and General Feeding PDFVindra MNo ratings yet
- Nutritional Needs of The Preterm InfantDocument3 pagesNutritional Needs of The Preterm InfantShuaib KauchaliNo ratings yet
- Drug Study CeelinDocument5 pagesDrug Study CeelinRoshley Em Manzano0% (2)
- Formula FeedingDocument4 pagesFormula FeedingZeineddin EtkaidekNo ratings yet
- Total Parenteral NutritionDocument13 pagesTotal Parenteral NutritionAmy LalringhluaniNo ratings yet
- Similac Plus Follow-Up Formula Stage 2 Powder 400 GMDocument1 pageSimilac Plus Follow-Up Formula Stage 2 Powder 400 GMashiareekattuNo ratings yet
- Nutritional RequireDocument64 pagesNutritional RequireSuren AgarwalNo ratings yet
- Fix Your Genes to Fit Your Jeans: Optimizing Diet, Health and Weight Through Personal GeneticsFrom EverandFix Your Genes to Fit Your Jeans: Optimizing Diet, Health and Weight Through Personal GeneticsNo ratings yet
- DOMAIN: Mental and Emotional Health OUTCOME: Adaptive Coping With Stress MEASURE: KIDCOPE - Child VersionDocument2 pagesDOMAIN: Mental and Emotional Health OUTCOME: Adaptive Coping With Stress MEASURE: KIDCOPE - Child Versionrr_eeyNo ratings yet
- Acute Kidney Injury - Cardiorenal Syndromes (Acute Decompensated Heart Failure and Worsening Renal Function) - Renal and Urology NewsDocument25 pagesAcute Kidney Injury - Cardiorenal Syndromes (Acute Decompensated Heart Failure and Worsening Renal Function) - Renal and Urology Newsrr_eeyNo ratings yet
- Brain Arteriovenous Malforamtion: Dr. Suresh Bishokarma MS, MCH (Neurosurgery)Document95 pagesBrain Arteriovenous Malforamtion: Dr. Suresh Bishokarma MS, MCH (Neurosurgery)rr_eeyNo ratings yet
- The Prevalence of Unrecognized Congenital Heart DiDocument6 pagesThe Prevalence of Unrecognized Congenital Heart Dirr_eeyNo ratings yet
- Unusual Course of Infective Endocarditis Acute RenDocument5 pagesUnusual Course of Infective Endocarditis Acute Renrr_eeyNo ratings yet
- Renal Compl of Bact EndoDocument6 pagesRenal Compl of Bact Endorr_eeyNo ratings yet
- Maharg Resume April 2017Document1 pageMaharg Resume April 2017api-292002018No ratings yet
- ST Teresas CollegeDocument25 pagesST Teresas Collegesree JithNo ratings yet
- Makeda Mikael Resume 7 Dietetics e PorfolioDocument2 pagesMakeda Mikael Resume 7 Dietetics e Porfolioapi-271347501No ratings yet
- CMO NO. 10 Series of 1998 CMO NO. 27 Series of 1998: Not StatedDocument7 pagesCMO NO. 10 Series of 1998 CMO NO. 27 Series of 1998: Not StatedJude BalalaNo ratings yet
- Irene Florence Mulongo CVDocument2 pagesIrene Florence Mulongo CVeddycorley2No ratings yet
- Dietetics Thesis TopicsDocument5 pagesDietetics Thesis Topicswbrgaygld100% (2)
- Bahaar Sharma - ResumeDocument2 pagesBahaar Sharma - Resumeapi-591355708No ratings yet
- Cruz Marissa Resume CsusbDocument3 pagesCruz Marissa Resume Csusbapi-341233003No ratings yet
- Final Print Uh As 2013Document92 pagesFinal Print Uh As 2013Francesca AckumburNo ratings yet
- Nutrition Degree Dissertation IdeasDocument5 pagesNutrition Degree Dissertation IdeasPaperWriterOnlineCanada100% (1)
- Concept 2 RowerDocument14 pagesConcept 2 Rowercscswimmer227No ratings yet
- Assessment-Tool-for CIU With RLED CommentsDocument7 pagesAssessment-Tool-for CIU With RLED CommentsLoreto District Hospital LDHNo ratings yet
- NM Self/Participant Direction Pre-Hire Packet: Criminal History Authorization For Release of Information (Required)Document7 pagesNM Self/Participant Direction Pre-Hire Packet: Criminal History Authorization For Release of Information (Required)ShellyJacksonNo ratings yet
- UC Davis General Catalog - Nutrition Science - 2022-03-13 - 231323Document12 pagesUC Davis General Catalog - Nutrition Science - 2022-03-13 - 231323XNo ratings yet
- Capstone ResumeDocument2 pagesCapstone Resumeapi-533745140No ratings yet
- Processing & Displaying Data: Research Methodology (Hfs4343)Document52 pagesProcessing & Displaying Data: Research Methodology (Hfs4343)Amouna Naouar Ep AbdelhakNo ratings yet
- Kelsey Buckley: EducationDocument2 pagesKelsey Buckley: Educationapi-241896339No ratings yet
- Enhanced Nursing Home Standards (2014)Document32 pagesEnhanced Nursing Home Standards (2014)cxz4321No ratings yet
- Majd Alomair: Clinical NutritionDocument6 pagesMajd Alomair: Clinical NutritionmajdNo ratings yet
- 4 Unit-Vi-Diet-TherapyDocument13 pages4 Unit-Vi-Diet-TherapyTrinidad SherwinNo ratings yet
- Grapevine, Winter2008Document20 pagesGrapevine, Winter2008Doug100% (6)
- Risk For Imbalanced NutritionDocument3 pagesRisk For Imbalanced Nutritionaudreyann.acobNo ratings yet
- Emily C. Bair, MS, MPH, RD: ContactDocument1 pageEmily C. Bair, MS, MPH, RD: Contactapi-381876451No ratings yet
- Sala A.Nadzria: Personal SkillsDocument3 pagesSala A.Nadzria: Personal SkillsNadzkhan JulmaniNo ratings yet