Download as pdf or txt
You might also like
- Code Examples For dsPIC30F4011Document28 pagesCode Examples For dsPIC30F4011Minh VuNo ratings yet
- Hospital Emergency Department Facility Audit Report - OT, Ward and Floor ManagementDocument12 pagesHospital Emergency Department Facility Audit Report - OT, Ward and Floor Managementjeremy joshuaNo ratings yet
- Disorders of PancreasDocument17 pagesDisorders of PancreasjonasNo ratings yet
- Yarn ManufacturerersDocument31 pagesYarn ManufacturerersMarufNo ratings yet
- Ncstudio V9 Programming Manual-R5.1Document102 pagesNcstudio V9 Programming Manual-R5.1beanib83No ratings yet
- Percutaneous Transhepatic Biliary InterventionsDocument11 pagesPercutaneous Transhepatic Biliary InterventionsLe Hu ThaNo ratings yet
- Obstructive Jaundice A Clinical StudyDocument7 pagesObstructive Jaundice A Clinical StudyAnisah Maryam DianahNo ratings yet
- mosler2011 2Document7 pagesmosler2011 2Althea Ninotschka AgaloosNo ratings yet
- 1Document10 pages1jeremy joshuaNo ratings yet
- Liver and BiliaryDocument15 pagesLiver and Biliaryasmatmasoom5566No ratings yet
- CH 7Document35 pagesCH 7Al VinaNo ratings yet
- Endoscopic Retrograde CholangiopancreatographyDocument7 pagesEndoscopic Retrograde CholangiopancreatographyMat JawiNo ratings yet
- Investigation and Treatment of Surgical JaundiceDocument38 pagesInvestigation and Treatment of Surgical JaundiceUjas PatelNo ratings yet
- 1 s2.0 S1365182X16317725 MainDocument6 pages1 s2.0 S1365182X16317725 MainocramusNo ratings yet
- Percutaneous Transhepatic Biliary Stenting: The First Experience and Results of The Hospital of Kaunas University of MedicineDocument8 pagesPercutaneous Transhepatic Biliary Stenting: The First Experience and Results of The Hospital of Kaunas University of MedicinefgrxczwyzyNo ratings yet
- Presentant: Dr. Arli Suryawinata Fasilitator: Dr. M.Iqbal Rivai, SP.-KBDDocument44 pagesPresentant: Dr. Arli Suryawinata Fasilitator: Dr. M.Iqbal Rivai, SP.-KBDArli SuryaNo ratings yet
- M.04 Liver (Part 4) (Dr. Cinio) (10-29-20)Document8 pagesM.04 Liver (Part 4) (Dr. Cinio) (10-29-20)VanessaNo ratings yet
- Acutecholangitis 110927014348 Phpapp01Document25 pagesAcutecholangitis 110927014348 Phpapp01shintameliaNo ratings yet
- Gra's Acute Pancreatitis-1Document37 pagesGra's Acute Pancreatitis-1Louis MushaikeNo ratings yet
- Scintigraphicdetectionof Segmentalbile-Ductobstruction: Case ReportsDocument2 pagesScintigraphicdetectionof Segmentalbile-Ductobstruction: Case ReportsMuzafar AhmedNo ratings yet
- Bile Duct DilatedDocument4 pagesBile Duct DilatedAmit GauravNo ratings yet
- Coledocolitiasis CurrentDocument6 pagesColedocolitiasis CurrentvalNo ratings yet
- Acute PancreatitisDocument5 pagesAcute PancreatitisLady Nell DescanzoNo ratings yet
- SMALL INTESTINE QuickDocument8 pagesSMALL INTESTINE QuickErald PaderangaNo ratings yet
- Mrcs HepatobiliaryDocument40 pagesMrcs HepatobiliaryAdebisiNo ratings yet
- Current Treatment of StricutresDocument4 pagesCurrent Treatment of StricutresAditya GNo ratings yet
- Investigation and Treatment of Surgical JaundiceDocument38 pagesInvestigation and Treatment of Surgical JaundiceUjas PatelNo ratings yet
- Laparoscopic Aproach in Hidatic CystDocument17 pagesLaparoscopic Aproach in Hidatic CystcrisssNo ratings yet
- 5) Image Interpretation AbdomenDocument68 pages5) Image Interpretation AbdomenMurkNo ratings yet
- Interventional Approaches Gallbladder DiseaseDocument9 pagesInterventional Approaches Gallbladder DiseaseAntônio GoulartNo ratings yet
- Diverticular DiseaseDocument8 pagesDiverticular DiseaseaizatamlikhaNo ratings yet
- Biliary AtresiaDocument39 pagesBiliary AtresiaRamesh ReddyNo ratings yet
- Madhu Sud Han 2016Document13 pagesMadhu Sud Han 2016Shivaraj S ANo ratings yet
- Marzano 2010 - Laparoscopic Treatment of Biliary Peritonitis Following Nonoperative Management of Blunt Liver TraumaDocument3 pagesMarzano 2010 - Laparoscopic Treatment of Biliary Peritonitis Following Nonoperative Management of Blunt Liver TraumaCandace LongNo ratings yet
- Pancreaticobilliary MaljunctionDocument7 pagesPancreaticobilliary MaljunctionadrianiNo ratings yet
- Materi DR Budi WidodoDocument44 pagesMateri DR Budi WidodoAnna Maria UlfaNo ratings yet
- Obstructive Jaundice: Abdel Rahman A. Al Manasra, MDDocument56 pagesObstructive Jaundice: Abdel Rahman A. Al Manasra, MDAmyandNo ratings yet
- DOI V3. Timing of Cholecystectomy - Pancreapedia - v4 6-22-15Document7 pagesDOI V3. Timing of Cholecystectomy - Pancreapedia - v4 6-22-15Oswaldo MascareñasNo ratings yet
- J Gastrointest Cancer 2019 50 3 578-82Document5 pagesJ Gastrointest Cancer 2019 50 3 578-82Fernando SousaNo ratings yet
- Acutecholangitis 110927014348 Phpapp01Document25 pagesAcutecholangitis 110927014348 Phpapp01Rabecca TobingNo ratings yet
- Z - 2016-03 - Spontaneous Rupture of Pancreatic Pseudocyst - Report of Two CasesDocument3 pagesZ - 2016-03 - Spontaneous Rupture of Pancreatic Pseudocyst - Report of Two CasesNawzad SulayvaniNo ratings yet
- Post-Operative Biliary StricturesDocument7 pagesPost-Operative Biliary StricturesGeraldNo ratings yet
- Management of The Pancreatic Remnant During Whipple OperationDocument4 pagesManagement of The Pancreatic Remnant During Whipple OperationYacine Tarik Aizel100% (1)
- Pancreatitis: M.N. Homoeopathic Medical College & Research Institute, Bikaner B.H.M.S. III YearDocument36 pagesPancreatitis: M.N. Homoeopathic Medical College & Research Institute, Bikaner B.H.M.S. III YearYamini SoniNo ratings yet
- Gastroduodenal Artery Pseudoaneurysm and Aberrant Right Hepatic ArteryDocument3 pagesGastroduodenal Artery Pseudoaneurysm and Aberrant Right Hepatic ArteryGordana PuzovicNo ratings yet
- Hepatobiliary and Pancreas Surgery: Liver Disease Management & Transplant ProgramDocument4 pagesHepatobiliary and Pancreas Surgery: Liver Disease Management & Transplant ProgramDeviselvam100% (1)
- Acta Anaesthesiologica Taiwanica: Long Wang, Wei-Feng YuDocument8 pagesActa Anaesthesiologica Taiwanica: Long Wang, Wei-Feng Yusitoxpadang ceriaNo ratings yet
- Kolangitis Case 1Document6 pagesKolangitis Case 1Dhen Mas PrimanaNo ratings yet
- Obstructive Jaundice Aetiological SpectrDocument8 pagesObstructive Jaundice Aetiological Spectrvvwaghmare30No ratings yet
- Chronic Pancreatitis 1Document21 pagesChronic Pancreatitis 1Bala DhanaNo ratings yet
- Gallstone Ileus, Surgical Management Review: Íleo Biliar, Revisión Del Manejo QuirúrgicoDocument5 pagesGallstone Ileus, Surgical Management Review: Íleo Biliar, Revisión Del Manejo Quirúrgicorama bagusNo ratings yet
- OJ EditedDocument57 pagesOJ EditedrobelNo ratings yet
- Surgical Clinics of North America (1996) - Surgical Management and Treatment of Pancreatic FistulasDocument15 pagesSurgical Clinics of North America (1996) - Surgical Management and Treatment of Pancreatic Fistulasjesus peñaNo ratings yet
- Case Based Teaching - Urology: Haematuria & Renal TransplantDocument21 pagesCase Based Teaching - Urology: Haematuria & Renal Transplantamoody95No ratings yet
- Iatrogenic Hepatopancreaticobiliary Injuries: A ReviewDocument13 pagesIatrogenic Hepatopancreaticobiliary Injuries: A ReviewJohn ShipNo ratings yet
- Chronic Pancreatitis: DefinitionDocument4 pagesChronic Pancreatitis: DefinitionDrVishwa PrakashNo ratings yet
- Background: Endoscopic Retrograde Cholangiopancreatography (ERCP)Document4 pagesBackground: Endoscopic Retrograde Cholangiopancreatography (ERCP)Resci Angelli Rizada-NolascoNo ratings yet
- Surgical JaundiceDocument35 pagesSurgical JaundiceIbsa ShumaNo ratings yet
- CA Gall BladderDocument24 pagesCA Gall BladderTheoder RobinsonNo ratings yet
- Abdominal Pain MARS 2.0 - Dr. Siswidiyati, SP - RadDocument34 pagesAbdominal Pain MARS 2.0 - Dr. Siswidiyati, SP - RadarifdeathsciethNo ratings yet
- Surgery For Acute Pancreatitis PDFDocument7 pagesSurgery For Acute Pancreatitis PDFValean DanNo ratings yet
- An Approach To Obstructive JaundiceDocument5 pagesAn Approach To Obstructive JaundiceEvediciNo ratings yet
- Answers Surgery ExamDocument17 pagesAnswers Surgery ExamKing Bal94No ratings yet
- Post-cholecystectomy Bile Duct InjuryFrom EverandPost-cholecystectomy Bile Duct InjuryVinay K. KapoorNo ratings yet
- Embolization MaterialsDocument19 pagesEmbolization Materialsjeremy joshuaNo ratings yet
- 1Document10 pages1jeremy joshuaNo ratings yet
- percutaneous-transhepatic-biliary-drainage-(ptbd)Document6 pagespercutaneous-transhepatic-biliary-drainage-(ptbd)jeremy joshuaNo ratings yet
- 44f693ec-9feb-4b4e-9899-dcb3bf424d9eDocument5 pages44f693ec-9feb-4b4e-9899-dcb3bf424d9ejeremy joshuaNo ratings yet
- lee2003Document3 pageslee2003jeremy joshuaNo ratings yet
- Cardiovascular Hoarseness (Ortner’s Syndrome) a Pictorial ReviewDocument6 pagesCardiovascular Hoarseness (Ortner’s Syndrome) a Pictorial Reviewjeremy joshuaNo ratings yet
- BS-Net: Learning COVID-19 Pneumonia Severity On A Large Chest X-Ray DatasetDocument28 pagesBS-Net: Learning COVID-19 Pneumonia Severity On A Large Chest X-Ray Datasetjeremy joshuaNo ratings yet
- Are Chest Radiographs Routinely Indicated After Chest Tubes Placed For Non-Surgical Reasons Are Removed?Document9 pagesAre Chest Radiographs Routinely Indicated After Chest Tubes Placed For Non-Surgical Reasons Are Removed?jeremy joshuaNo ratings yet
- Deep Learning For Chest Radiograph Diagnosis in The Emergency DepartmentDocument8 pagesDeep Learning For Chest Radiograph Diagnosis in The Emergency Departmentjeremy joshuaNo ratings yet
- Missed Lung CancersDocument14 pagesMissed Lung Cancersjeremy joshuaNo ratings yet
- Journal Vaksin DHF PDFDocument11 pagesJournal Vaksin DHF PDFjeremy joshuaNo ratings yet
- Treatment Modalities For Lumbar Herniated Discs That Cause SciaticaDocument3 pagesTreatment Modalities For Lumbar Herniated Discs That Cause Sciaticajeremy joshuaNo ratings yet
- Syndrome: A Placebo-Controlled,: Failure of High-Dose Methylprednisolone in Established Dengue Shock Double-Blind StudyDocument7 pagesSyndrome: A Placebo-Controlled,: Failure of High-Dose Methylprednisolone in Established Dengue Shock Double-Blind Studyjeremy joshuaNo ratings yet
- Clay & Shale Industries in OntarioDocument193 pagesClay & Shale Industries in OntarioJohn JohnsonNo ratings yet
- Application of UV Spectrophotometric Method For Estimation of Iron in Tablet Dosage FormDocument2 pagesApplication of UV Spectrophotometric Method For Estimation of Iron in Tablet Dosage Formahmed ismailNo ratings yet
- EVS Level A - Workbook 202108041859159269Document50 pagesEVS Level A - Workbook 202108041859159269Nabhasvit HegdeNo ratings yet
- Consumption of Functional Food and Our Health ConcernsDocument8 pagesConsumption of Functional Food and Our Health ConcernsPhysiology by Dr RaghuveerNo ratings yet
- Rev0 (Technical and User's Manual)Document72 pagesRev0 (Technical and User's Manual)mohamedNo ratings yet
- Autoclaved Aerated ConcreteDocument4 pagesAutoclaved Aerated ConcreteArunima DineshNo ratings yet
- Machine Design Final Coaching ProblemsDocument63 pagesMachine Design Final Coaching ProblemsasapamoreNo ratings yet
- The Welding Journal 1958 7Document150 pagesThe Welding Journal 1958 7AlexeyNo ratings yet
- LEAP Brochure 2013Document15 pagesLEAP Brochure 2013Reparto100% (1)
- Design Process in ElectrochemistryDocument92 pagesDesign Process in ElectrochemistryWulan SariNo ratings yet
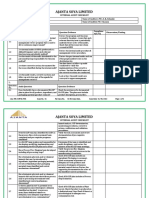
- Internal Audit Checklist Food Safety-MRDocument5 pagesInternal Audit Checklist Food Safety-MRRavi BaghelNo ratings yet
- SnowblowerDocument28 pagesSnowblowerJim KrebsNo ratings yet
- Traumatic Diaphragmatic Hernia: Case Series and Topic ReviewDocument12 pagesTraumatic Diaphragmatic Hernia: Case Series and Topic ReviewMohammad SyahrezkiNo ratings yet
- A7D/A7DP: Ultra-Small, Low-Cost, Push-Operated SwitchesDocument5 pagesA7D/A7DP: Ultra-Small, Low-Cost, Push-Operated SwitchesHerbitus DuininhoNo ratings yet
- About Barfani DadajiDocument4 pagesAbout Barfani DadajiNaren MukherjeeNo ratings yet
- Tomographic Imaging in Aditya Tokamak: Nitin JainDocument21 pagesTomographic Imaging in Aditya Tokamak: Nitin JainHafiz Luqman SaifiNo ratings yet
- Instalacion de Kits de Aislamiento PIKOTEKDocument2 pagesInstalacion de Kits de Aislamiento PIKOTEKAlfonso Alberto ArguelloNo ratings yet
- Sastra University Biosensors SyllabusDocument2 pagesSastra University Biosensors SyllabusAkshey BadrinarayanNo ratings yet
- Dextrose Prolotherapy For Muscle, Tendon and Ligament Injury or Pathology: A Systematic ReviewDocument21 pagesDextrose Prolotherapy For Muscle, Tendon and Ligament Injury or Pathology: A Systematic ReviewJP ChenNo ratings yet
- Comparison of Greenhouse Gas AnalyzersDocument7 pagesComparison of Greenhouse Gas AnalyzersSabeeqa MalikNo ratings yet
- Review Paper: There Are 5 Branches That We Choose To TasteDocument3 pagesReview Paper: There Are 5 Branches That We Choose To TasteAllysa BatoliñoNo ratings yet
- Jagdtiger: Panzerjäger Tiger Ausf. BDocument11 pagesJagdtiger: Panzerjäger Tiger Ausf. Bjason maiNo ratings yet
- ON Diesel D2 Russian Gasoil L-0.2-62 Gost 305-82 Contract SpotDocument10 pagesON Diesel D2 Russian Gasoil L-0.2-62 Gost 305-82 Contract Spotdendy alfasaNo ratings yet
- EnviSci Lesson 9 Land Management and ConservationDocument33 pagesEnviSci Lesson 9 Land Management and ConservationJohn Carlo De Guzman OcampoNo ratings yet
- Session - 2 Other Sources HintsDocument36 pagesSession - 2 Other Sources HintsJohn KAlespiNo ratings yet
- ALTITUDE Presentation DeckDocument35 pagesALTITUDE Presentation DeckVikas ChaudharyNo ratings yet