Download as pdf or txt
You might also like
- Campbell - Walsh-Wein UROLOGY 12th Ed (Dragged)Document20 pagesCampbell - Walsh-Wein UROLOGY 12th Ed (Dragged)revanth kallaNo ratings yet
- Renal FailureDocument48 pagesRenal FailureCindy MamalangkasNo ratings yet
- Toshiba Case 3Document4 pagesToshiba Case 3Deta Detade100% (1)
- An Overview Of: Acute Kidney Injury (Aki: Hasan BasriDocument22 pagesAn Overview Of: Acute Kidney Injury (Aki: Hasan BasriDz PutraNo ratings yet
- Opgave 1: Side 1 Af 11Document11 pagesOpgave 1: Side 1 Af 11shamoNo ratings yet
- Renal Function TestsDocument34 pagesRenal Function TestsMandavi HindNo ratings yet
- MNT Penyakit GinjalDocument41 pagesMNT Penyakit GinjalNurfitriana DwiNo ratings yet
- Kidney and Liver Function TestsDocument76 pagesKidney and Liver Function TestsKellyNo ratings yet
- Chronic Kidney Disease in ChildrenDocument29 pagesChronic Kidney Disease in ChildrenAlvin OmondiNo ratings yet
- 16 - RE - Acute Kidney InjuryDocument8 pages16 - RE - Acute Kidney Injury078229933aaNo ratings yet
- Renal Failure March 2020Document46 pagesRenal Failure March 2020dicksonsamboNo ratings yet
- Renal PathologyDocument31 pagesRenal PathologySaddamix AL OmariNo ratings yet
- Acute Kidney Failure: Dr. Syamsudin, M.Biomed Fakultas Farmasi Universitas PancasilaDocument48 pagesAcute Kidney Failure: Dr. Syamsudin, M.Biomed Fakultas Farmasi Universitas PancasilariyuNo ratings yet
- Abnormal Constituents of Urine Interpretation PracticalDocument42 pagesAbnormal Constituents of Urine Interpretation PracticalTEJASWI ModiNo ratings yet
- Renal Diseases " Review "Document22 pagesRenal Diseases " Review "api-3827876No ratings yet
- Chronic Renal FailureDocument28 pagesChronic Renal FailuremarshmalouNo ratings yet
- Acute Kidney Injury:: A Brief OutlineDocument48 pagesAcute Kidney Injury:: A Brief OutlinehanaNo ratings yet
- Urinalysis 1Document27 pagesUrinalysis 1ullifannuriNo ratings yet
- Chem Lect Unit 7 Kidney FunctionDocument38 pagesChem Lect Unit 7 Kidney FunctionMustafa KhandgawiNo ratings yet
- 6 - Clinical 2Document46 pages6 - Clinical 2levan guluaNo ratings yet
- Kidney DiseasesDocument45 pagesKidney DiseasesSai ViswasNo ratings yet
- HBC/BC 306 Clinical Biochemistry: Type of SamplesDocument25 pagesHBC/BC 306 Clinical Biochemistry: Type of SamplesTennidoxNo ratings yet
- 7.acute Renal Failure (ARF)Document20 pages7.acute Renal Failure (ARF)Mahesh RathnayakeNo ratings yet
- IRC EngDocument89 pagesIRC EngMadalina SercaianuNo ratings yet
- Urine ExaminationDocument45 pagesUrine ExaminationSalwa FaisalNo ratings yet
- Renal PathophysiologyDocument35 pagesRenal Pathophysiologyyolondanic100% (1)
- ChemistryDocument103 pagesChemistryadis alemNo ratings yet
- Acute Kidney InjuryDocument16 pagesAcute Kidney InjuryPutrii Rahayu Sriikandi100% (1)
- AKIDocument23 pagesAKInadddNo ratings yet
- URINALYSISDocument63 pagesURINALYSISMedah Naserian100% (2)
- Renal Function TestsDocument43 pagesRenal Function TestsAbdulelah MurshidNo ratings yet
- Surgery Acute Kidney Injury 10-06-21Document49 pagesSurgery Acute Kidney Injury 10-06-21Muhammad ArsalNo ratings yet
- Surgery Acute Kidney Injury 10-06-21Document49 pagesSurgery Acute Kidney Injury 10-06-21Muhammad ArsalNo ratings yet
- Drugs Therapy For Kidney: Budi RaharjoDocument33 pagesDrugs Therapy For Kidney: Budi RaharjoNurul MasyithahNo ratings yet
- Acute Renal Failure: DR Grania PriceDocument24 pagesAcute Renal Failure: DR Grania PriceCastro KisuuleNo ratings yet
- URINALYSISDocument80 pagesURINALYSISredr7131No ratings yet
- Aki & CKD 2024Document68 pagesAki & CKD 2024AhemigishaNo ratings yet
- 1 - GueDocument24 pages1 - GueQasmNo ratings yet
- DRUGs FOR KIDNEYDocument33 pagesDRUGs FOR KIDNEYaNo ratings yet
- Urinepractical 200121115146Document56 pagesUrinepractical 200121115146Nakul JainNo ratings yet
- Kidney Diseases: Ivan Surya PradiptaDocument29 pagesKidney Diseases: Ivan Surya PradiptaAthirah BidinNo ratings yet
- Clinical Chemistry Renal FunctionDocument20 pagesClinical Chemistry Renal FunctionNida RidzuanNo ratings yet
- Care of The Patient With Renal and Urinary Disorders - HandoutDocument52 pagesCare of The Patient With Renal and Urinary Disorders - HandoutAaron Ramirez LuNo ratings yet
- Assessment or Acute Renal Failure SymptomsDocument6 pagesAssessment or Acute Renal Failure SymptomsRifa Aprillia CahyaniNo ratings yet
- Acute Kidney InjuryDocument64 pagesAcute Kidney InjuryBIAN ALKHAZMARINo ratings yet
- Chronic Kidney Failure Transplant 2Document22 pagesChronic Kidney Failure Transplant 2Gail Leslie HernandezNo ratings yet
- ESTIMATION OF UreaDocument13 pagesESTIMATION OF Ureaahmadhasham86No ratings yet
- Gagal Ginjal Kuliah FarmakoterapiDocument39 pagesGagal Ginjal Kuliah FarmakoterapiriyuNo ratings yet
- Renal Function TestsDocument38 pagesRenal Function TestsSupriya NayakNo ratings yet
- Renal FailureDocument2 pagesRenal Failurebimbong12No ratings yet
- Acute Renal FailureDocument15 pagesAcute Renal Failureayesha.facultyNo ratings yet
- Clinical Features of Renal DiseaseDocument80 pagesClinical Features of Renal DiseaseIdiAmadouNo ratings yet
- Diet Penyakit Ginjal Dan Saluran KemihDocument73 pagesDiet Penyakit Ginjal Dan Saluran KemihNurul AlfatarisyaNo ratings yet
- Acute Kidney Injury (AkiDocument23 pagesAcute Kidney Injury (AkiHyunna 15No ratings yet
- FLG 332 Renal Physiology-3 (2019)Document29 pagesFLG 332 Renal Physiology-3 (2019)Huzaifa KhanNo ratings yet
- Acute Renal FailureDocument45 pagesAcute Renal FailureRubinNo ratings yet
- Definition-Acute Kidney InjuryDocument6 pagesDefinition-Acute Kidney Injuryashi leginNo ratings yet
- Renal Function Test Amcj 8Document42 pagesRenal Function Test Amcj 8Md. Saifur Rahman SunnyNo ratings yet
- Renal Function Test (RFT) : Muhammad Asif Shaheen Lecturer Pathology Kemu, LahoreDocument14 pagesRenal Function Test (RFT) : Muhammad Asif Shaheen Lecturer Pathology Kemu, LahoreRimsha MustafaNo ratings yet
- What Is: Acute Renal Failure Acute Kidney InjuryDocument32 pagesWhat Is: Acute Renal Failure Acute Kidney InjuryCiedelle Honey Lou DimaligNo ratings yet
- Acute Kidney InjuryDocument15 pagesAcute Kidney InjuryGabrielle Frances FernandezNo ratings yet
- Czaja - LFTsDocument59 pagesCzaja - LFTsparik2321No ratings yet
- Liver Cirrhosis, A Simple Guide To The Condition, Treatment And Related DiseasesFrom EverandLiver Cirrhosis, A Simple Guide To The Condition, Treatment And Related DiseasesNo ratings yet
- Roles of Physiotherapy in Intensive Care Unit (Document28 pagesRoles of Physiotherapy in Intensive Care Unit (Chukwuemeka ChidogoNo ratings yet
- Rela Tori OhhDocument1,830 pagesRela Tori OhhLeandro MedeirosNo ratings yet
- Bhuvanesh 60Document2 pagesBhuvanesh 60astheleoNo ratings yet
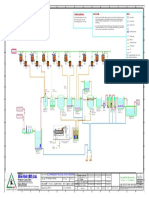
- Alim Knit (BD) LTD.: Recommended Process Flow DiagramDocument1 pageAlim Knit (BD) LTD.: Recommended Process Flow DiagramKamrul HasanNo ratings yet
- Standard CVDocument3 pagesStandard CVSurzo Chandra DasNo ratings yet
- Example 12: Design of Panel Walls: SolutionDocument2 pagesExample 12: Design of Panel Walls: SolutionSajidAliKhanNo ratings yet
- Lesson 1 - Plumbing MaterialsDocument18 pagesLesson 1 - Plumbing MaterialsNicholas Bonn SingNo ratings yet
- Lesson Plan PatrickDocument4 pagesLesson Plan PatrickPatrick Jerome SilvanoNo ratings yet
- EF4e Intplus Filetest 3bDocument7 pagesEF4e Intplus Filetest 3bjeanneramazanovaNo ratings yet
- Users' Preference Towards Traditional Banking Versus E-Banking - An Analysis Dr. S. Anthony Rahul GoldenDocument6 pagesUsers' Preference Towards Traditional Banking Versus E-Banking - An Analysis Dr. S. Anthony Rahul GoldenOmotayo AkinpelumiNo ratings yet
- EN EU Declaration of Conformity VEGAPULS Serie 60Document8 pagesEN EU Declaration of Conformity VEGAPULS Serie 60Jhon SuarezNo ratings yet
- A Study On The Dance Form of Yangge in Hebei, China: Multicultural EducationDocument3 pagesA Study On The Dance Form of Yangge in Hebei, China: Multicultural EducationdannialleeNo ratings yet
- Podman Part4Document5 pagesPodman Part4anbuchennai82No ratings yet
- Suraj Estate Developers Limited RHPDocument532 pagesSuraj Estate Developers Limited RHPJerry SinghNo ratings yet
- Egyptian PPP Law 67 For 2010 EnglishDocument17 pagesEgyptian PPP Law 67 For 2010 EnglishReham El AbnoudyNo ratings yet
- Hand Book of Transport Mode Lling - : Kenneth J. ButtonDocument8 pagesHand Book of Transport Mode Lling - : Kenneth J. ButtonSamuel ValentineNo ratings yet
- Marcopolo Is A Leading Brazilian Bus Body ManufacturerDocument4 pagesMarcopolo Is A Leading Brazilian Bus Body ManufacturerCH NAIRNo ratings yet
- Superficial Fungal Infections (2019)Document6 pagesSuperficial Fungal Infections (2019)mustika rachmaNo ratings yet
- Ijleo S 23 06033Document26 pagesIjleo S 23 06033Laura DiazNo ratings yet
- TensesDocument1 pageTensesharis ilyasNo ratings yet
- Dna Microarray Technology: Fatoki John OlabodeDocument9 pagesDna Microarray Technology: Fatoki John Olabodejohn tokiNo ratings yet
- LG W1943C Chass LM92C PDFDocument23 pagesLG W1943C Chass LM92C PDFDaniel Paguay100% (1)
- Case Study Emirates AirlinesDocument4 pagesCase Study Emirates Airlinesuzzmapk33% (9)
- Analysis of Customer Attitude, Preference and Satisfaction Level of Mutual Fund InvestmentDocument109 pagesAnalysis of Customer Attitude, Preference and Satisfaction Level of Mutual Fund Investmentlalitgitam80% (5)
- Market Composition and Performance of Firms in Broiler, Chicken Egg, and Swine Production - Implications To The Philippine Competition ActDocument17 pagesMarket Composition and Performance of Firms in Broiler, Chicken Egg, and Swine Production - Implications To The Philippine Competition ActAshlley Nicole VillaranNo ratings yet
- Applied Economics Module 3 Q1Document21 pagesApplied Economics Module 3 Q1Jefferson Del Rosario100% (1)
- SSP Assignment Problems - FinalDocument2 pagesSSP Assignment Problems - FinalVadivelan AdaikkappanNo ratings yet