Download as pdf or txt
You might also like
- Textbook of GB Madhuri For Cardio-Respiratory Cardiac Surgery and Thoracic Surgery ConditionsDocument340 pagesTextbook of GB Madhuri For Cardio-Respiratory Cardiac Surgery and Thoracic Surgery ConditionsBpt4 Kims100% (1)
- Toronto Notes - Cardiac SurgeryDocument32 pagesToronto Notes - Cardiac Surgerymicielij100% (1)
- How To Detect and To Treat EarlierDocument59 pagesHow To Detect and To Treat EarlierFaisal ShaldyNo ratings yet
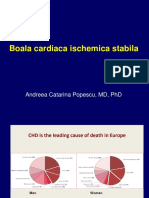
- Atherosclerosis and Stable Ihd-HorvathDocument60 pagesAtherosclerosis and Stable Ihd-HorvathTaarik DookieNo ratings yet
- Chest Pain Evaluation and Management - 2023 - Physician Assistant ClinicsDocument16 pagesChest Pain Evaluation and Management - 2023 - Physician Assistant ClinicsJose AnaconaNo ratings yet
- Study Guide 4Document21 pagesStudy Guide 4cNo ratings yet
- Anaesthetic Management of A Patient With Ischaemic Heart Disease Undergoing Non Cardiac SurgeryDocument72 pagesAnaesthetic Management of A Patient With Ischaemic Heart Disease Undergoing Non Cardiac SurgeryDebasis SahooNo ratings yet
- CardiologyDocument52 pagesCardiologyDexzal100% (2)
- Acute Coronary SyndromeDocument84 pagesAcute Coronary SyndromeRinkita MallickNo ratings yet
- Angina Pect & Infark Miokard (Dr. Ilham Uddin, SP - JP (K) )Document108 pagesAngina Pect & Infark Miokard (Dr. Ilham Uddin, SP - JP (K) )Vania Nazhara FitrianaNo ratings yet
- Acute Coronary Syndrome (G4)Document6 pagesAcute Coronary Syndrome (G4)Francis Josh DagohoyNo ratings yet
- CAD - Ischemic Heart Disease: AtherosclerosisDocument5 pagesCAD - Ischemic Heart Disease: Atherosclerosisbri ngNo ratings yet
- CARDIAC IMAGISTIC MRI AND CT GifDocument39 pagesCARDIAC IMAGISTIC MRI AND CT GifAlexandra StancuNo ratings yet
- DR Supartono-ECG DiagnosisDocument85 pagesDR Supartono-ECG DiagnosisvinahandoyoNo ratings yet
- Chronic Coronary SyndromeDocument71 pagesChronic Coronary SyndromeNancy VellisiaNo ratings yet
- 25 Cardiovascular DiseaseDocument35 pages25 Cardiovascular DiseaseBramantyo NugrosNo ratings yet
- Angina Stabila 2019Document132 pagesAngina Stabila 2019raresteo96No ratings yet
- Acute Coronary SyndromeDocument57 pagesAcute Coronary SyndromePreety ShresthaNo ratings yet
- Cardiogenic ShockDocument9 pagesCardiogenic Shockrio kharismaNo ratings yet
- Danger, Danger, High Output - 2023 - JscaiDocument3 pagesDanger, Danger, High Output - 2023 - JscaiLuis Rafael Suárez U.No ratings yet
- Heart Failure: Departemen Kardiologi FK USU RSUP. H. Adam Malik MedanDocument42 pagesHeart Failure: Departemen Kardiologi FK USU RSUP. H. Adam Malik Medanbilli lisanuddinNo ratings yet
- Energency Skill Lec 2Document50 pagesEnergency Skill Lec 2adnanreshunNo ratings yet
- Arterial Stiffness-1Document21 pagesArterial Stiffness-1yoeldp100% (2)
- Heart Failure: Departemen Kardiologi FK USU RSUP. H. Adam Malik MedanDocument48 pagesHeart Failure: Departemen Kardiologi FK USU RSUP. H. Adam Malik MedanAlbert SitepuNo ratings yet
- Acute Coronary Syndrome Sindroma Koroner AkutDocument50 pagesAcute Coronary Syndrome Sindroma Koroner AkutWinda Ayu PurnamasariNo ratings yet
- MateriDocument39 pagesMateriDR BASUKINo ratings yet
- Konsep Tatalaksana Pada ImaDocument57 pagesKonsep Tatalaksana Pada Imariska silviaNo ratings yet
- Cardiac Biomarker 2014Document52 pagesCardiac Biomarker 2014karin amalia sabrina100% (1)
- Acs Acls Aha 2015Document63 pagesAcs Acls Aha 2015Desy Nurlailani IlmaNo ratings yet
- StrokeDocument53 pagesStrokeGhinaSofianaLestari100% (1)
- Acute Coronary Syndrome (Acs) : DR M. Arman Nasution SPPDDocument162 pagesAcute Coronary Syndrome (Acs) : DR M. Arman Nasution SPPDfifahNo ratings yet
- Ischaemic Heart Disease Mku 2020Document38 pagesIschaemic Heart Disease Mku 2020ElvisNo ratings yet
- Penyakit Kardiovaskular Yang Sering DijumpaiDocument121 pagesPenyakit Kardiovaskular Yang Sering Dijumpaiandikaagus13No ratings yet
- Acute & Chronic Heart Failure: Dr. Nurkhalis, SPJP, FihaDocument98 pagesAcute & Chronic Heart Failure: Dr. Nurkhalis, SPJP, FihablackcatNo ratings yet
- ACS LectureDocument74 pagesACS Lecturekarin amalia sabrinaNo ratings yet
- Acs AmiDocument79 pagesAcs Amihhh hhhNo ratings yet
- Instrumental MethodDocument24 pagesInstrumental Methodzerish0208No ratings yet
- Single Coronary Artery Anomaly Case ReportDocument5 pagesSingle Coronary Artery Anomaly Case ReportJhonike NawipaNo ratings yet
- Acute Coronary Syndrome Sindroma Koroner Akut: Toni Mustahsani Aprami, DR., SPPD, SPJPDocument57 pagesAcute Coronary Syndrome Sindroma Koroner Akut: Toni Mustahsani Aprami, DR., SPPD, SPJPrian susantoNo ratings yet
- Kelainan Pembuluh DarahDocument81 pagesKelainan Pembuluh DarahAnisa Karamina WardaniNo ratings yet
- ACS LectureDocument76 pagesACS Lecture21701101047 Laksmita AnggaraniNo ratings yet
- ACS MALEEKDocument42 pagesACS MALEEKAbdul maleek rexNo ratings yet
- Acute Coronary SyndromeDocument43 pagesAcute Coronary SyndromeberthyNo ratings yet
- Askep Pada Acute Coronary Syndrome AcsDocument62 pagesAskep Pada Acute Coronary Syndrome Acsdefi rhNo ratings yet
- Syahrul: Department of Neurology Faculty of Medicine, Syiah Kuala University Banda Aceh, March 29, 2011Document53 pagesSyahrul: Department of Neurology Faculty of Medicine, Syiah Kuala University Banda Aceh, March 29, 2011Nasyirah IsmailNo ratings yet
- Basic Cardiac Ds C-1 RadiologyDocument30 pagesBasic Cardiac Ds C-1 RadiologygetemeselewNo ratings yet
- Acute Coronary Syndrome Sindroma Koroner Akut: PUJI RAHAYU,.S.Kep.,Ners, M.KepDocument52 pagesAcute Coronary Syndrome Sindroma Koroner Akut: PUJI RAHAYU,.S.Kep.,Ners, M.KepLabu SiamNo ratings yet
- Acute Coronary SyndromeDocument42 pagesAcute Coronary SyndromeGorgieNo ratings yet
- Coronary Artery DiseaseDocument20 pagesCoronary Artery DiseaseAli Aborges Jr.No ratings yet
- Syok Kardiogenik PPT (3440) - 1Document18 pagesSyok Kardiogenik PPT (3440) - 1Mark YangNo ratings yet
- Review Notes 2000 - CardiologyDocument58 pagesReview Notes 2000 - Cardiologyeliaszavaleta100% (1)
- Aortic AneurysmDocument20 pagesAortic AneurysmMargaretta LimawanNo ratings yet
- Cardiac Care and COVID-19: Perspectives in Medical PracticeFrom EverandCardiac Care and COVID-19: Perspectives in Medical PracticeNo ratings yet
- Compendium on Cardiomyopathies - Basics, Therapeutics, and PerspectivesFrom EverandCompendium on Cardiomyopathies - Basics, Therapeutics, and PerspectivesNo ratings yet
- Comprehensive Insights into Acute Coronary Syndrome: Pathways, Interventions, and Holistic RecoveryFrom EverandComprehensive Insights into Acute Coronary Syndrome: Pathways, Interventions, and Holistic RecoveryNo ratings yet
- Atlas of Coronary Intravascular Optical Coherence TomographyFrom EverandAtlas of Coronary Intravascular Optical Coherence TomographyNo ratings yet
- MPAS540 2019 PA Medicine I SyllabusDocument6 pagesMPAS540 2019 PA Medicine I SyllabusSteven CongressNo ratings yet
- Coronary Revascularization of The Anterior Descending ArteryDocument13 pagesCoronary Revascularization of The Anterior Descending Arteryapi-658511625No ratings yet
- Coronary Artery DiseaseDocument22 pagesCoronary Artery DiseaseApil BhutaniNo ratings yet
- Week 29-Angina - MI PDFDocument7 pagesWeek 29-Angina - MI PDFJaimie Charlotte Marie LangilleNo ratings yet
- Presented By: Nor Maisarah BT Mohamed Shukri Supervisor: Dr. Pendrik Tandean, SPPDDocument28 pagesPresented By: Nor Maisarah BT Mohamed Shukri Supervisor: Dr. Pendrik Tandean, SPPDRika Yulizah GobelNo ratings yet
- Blood Supply of The Heart & Conduction System: Dr. Nabil KhouriDocument37 pagesBlood Supply of The Heart & Conduction System: Dr. Nabil KhouriDefyna Dwi LestariNo ratings yet
- Ischemic Heart Disease Congestive Heart Failure ShockDocument30 pagesIschemic Heart Disease Congestive Heart Failure ShockHerbert Baquerizo VargasNo ratings yet
- Diagnosis and Management of Stable AnginaDocument14 pagesDiagnosis and Management of Stable AnginaDiosvel José SarmientoNo ratings yet
- Textbook of Anaesthesia For Postgraduates PDFDocument1,218 pagesTextbook of Anaesthesia For Postgraduates PDFMohammad HayajnehNo ratings yet
- Bioavailability and Pharmacokinetics of Magnesium AfterDocument13 pagesBioavailability and Pharmacokinetics of Magnesium Afternoviyanti christianaNo ratings yet
- INTENSIVE CARDIOVASCULAR NURSING NotesDocument19 pagesINTENSIVE CARDIOVASCULAR NURSING NotesZayne Lucas Gabrielle TadiamonNo ratings yet
- Cardiogenic Shock: Sparsh Goel 77Document28 pagesCardiogenic Shock: Sparsh Goel 77Sparsh GoelNo ratings yet
- Cardiology WorkBookDocument102 pagesCardiology WorkBookCastleKGNo ratings yet
- PathophysiologyDocument137 pagesPathophysiologyAhmed S. Hamid0% (1)
- Degenerative Disorders: by Dr. Madiha Ehsan UlhaqDocument31 pagesDegenerative Disorders: by Dr. Madiha Ehsan UlhaqMohad HaiderNo ratings yet
- Tndlive Medicine1Document45 pagesTndlive Medicine1Madhu SowmithaNo ratings yet
- Buddiga, 2014 Cardiovascular System Anatomy - Overview, Gross Anatomy, Natural VariantsDocument13 pagesBuddiga, 2014 Cardiovascular System Anatomy - Overview, Gross Anatomy, Natural VariantsAzilu FalaNo ratings yet
- SL Penyakit Jantung Pulmonal & HipertensiDocument24 pagesSL Penyakit Jantung Pulmonal & HipertensiReni MelindaNo ratings yet
- Pathophysiology Worksheet MIDocument2 pagesPathophysiology Worksheet MIpjbedelNo ratings yet
- Notes For Responses To Altered Tissue PerfusionDocument12 pagesNotes For Responses To Altered Tissue Perfusiondivine armentonNo ratings yet
- Transport in AnimalsDocument81 pagesTransport in AnimalsIbrahim NOORZADNo ratings yet
- Human Circulatory SystemDocument3 pagesHuman Circulatory SystemMir Rehan Mushtaq100% (1)
- IabpDocument152 pagesIabpRaghavendra PrasadNo ratings yet
- The Anatomy of The Coronary SinusDocument7 pagesThe Anatomy of The Coronary Sinusmihalcea alinNo ratings yet
- Aan 204 Group Coursework: in Partial Fulfillment of The Requirements For The CourseDocument118 pagesAan 204 Group Coursework: in Partial Fulfillment of The Requirements For The CourseLucian CaelumNo ratings yet
- Cvs 253Document253 pagesCvs 253CHALIE MEQUNo ratings yet
- What Is in A Name EssayDocument5 pagesWhat Is in A Name Essayxlgnhkaeg100% (2)
- Cardio Exercise Testing in Children and AdolecentsDocument288 pagesCardio Exercise Testing in Children and AdolecentsTeoNo ratings yet
- Technical Seminar For Intra-Aortic Balloon Pumping System 98/98XTDocument43 pagesTechnical Seminar For Intra-Aortic Balloon Pumping System 98/98XTGabriel MorilloNo ratings yet