Download as pdf or txt
You might also like
- Good Clinical Practice GuideFrom EverandGood Clinical Practice GuideRating: 5 out of 5 stars5/5 (1)
- Mrs Anar DeviDocument14 pagesMrs Anar DeviM.DNo ratings yet
- CBC 060619Document3 pagesCBC 060619Vijay SapraNo ratings yet
- 21.gigitan Ular (Snake Bite)Document16 pages21.gigitan Ular (Snake Bite)Priati Mprit100% (1)
- Lab - Report - BHAVISHKA JIDocument4 pagesLab - Report - BHAVISHKA JIYogeshKumarLoharNo ratings yet
- Screenshot 2024-04-03 at 10.12.42Document5 pagesScreenshot 2024-04-03 at 10.12.42Rajendra DagaonkarNo ratings yet
- Final: Code/Name & AddressDocument19 pagesFinal: Code/Name & AddressSUNSHINE DIAGNOSTICSNo ratings yet
- 0006XB0133786_565341vDocument11 pages0006XB0133786_565341vSahilNo ratings yet
- ExistingAppointment 1222869Document6 pagesExistingAppointment 1222869jecaw39027No ratings yet
- Juhi Shinde (871) 05.05.23Document6 pagesJuhi Shinde (871) 05.05.23Tushar ShindeNo ratings yet
- agilius report_unlockedDocument8 pagesagilius report_unlockedSucharit NarangNo ratings yet
- Diagnostic Report: FinalDocument7 pagesDiagnostic Report: FinalAhskNo ratings yet
- ReportDocument13 pagesReportAbhilashNo ratings yet
- Diagnostic Report: Client Code: Client'S Name and AddressDocument3 pagesDiagnostic Report: Client Code: Client'S Name and AddressDr.Sandeep SahuNo ratings yet
- Final: Code/Name & AddressDocument6 pagesFinal: Code/Name & AddresscrypticgarvNo ratings yet
- Final: Client Code: Client'S Name and AddressDocument2 pagesFinal: Client Code: Client'S Name and AddressPratsNo ratings yet
- Miss. BHAGYA LAXMIDocument2 pagesMiss. BHAGYA LAXMIpeetlasuresh921No ratings yet
- PdfText23 03 29T07490Document9 pagesPdfText23 03 29T07490Sudhir BhardwajNo ratings yet
- Diagnostic Report: FinalDocument8 pagesDiagnostic Report: FinalNeel RudraNo ratings yet
- Labreportnew (8) - 3Document11 pagesLabreportnew (8) - 3Rocky JNo ratings yet
- Afridi Shaikh-23Document5 pagesAfridi Shaikh-23Altamash AnsariNo ratings yet
- Diagnostic Report: Patient Name: Lakshmi Narayanappa FH.4309345 0093UE001838Document5 pagesDiagnostic Report: Patient Name: Lakshmi Narayanappa FH.4309345 0093UE001838Aditya LNo ratings yet
- MR JoshanramDocument4 pagesMR JoshanrammuthurajctNo ratings yet
- Medical Test ReportDocument10 pagesMedical Test ReportPadmaraj NairNo ratings yet
- 0015TH01116615 798775c PDFDocument3 pages0015TH01116615 798775c PDFAyush Kumar GuptaNo ratings yet
- Diagnostic Report: FinalDocument10 pagesDiagnostic Report: FinalKushagra SahniNo ratings yet
- Devendra - 2401611Document3 pagesDevendra - 2401611arslansiddique406No ratings yet
- Diagnostic Report: PreliminaryDocument8 pagesDiagnostic Report: PreliminarySaini VarunNo ratings yet
- Diagnostic Report: Client Code: Client'S Name and AddressDocument3 pagesDiagnostic Report: Client Code: Client'S Name and AddressKhurram Shadab IqbalNo ratings yet
- HeaderDocument13 pagesHeaderRoshan Virat PandeyNo ratings yet
- 0afc33cc Aee6 11ee A7f8 7c1e520e223c HeaderDocument21 pages0afc33cc Aee6 11ee A7f8 7c1e520e223c Headerpparmar871No ratings yet
- Diagnostic Report: Patient Name: Sekhar Borah SEKHM241220530 0015TH003971Document11 pagesDiagnostic Report: Patient Name: Sekhar Borah SEKHM241220530 0015TH003971sekharNo ratings yet
- ReportDocument19 pagesReportpparmar871No ratings yet
- Mr. Jay Narayan YadavDocument5 pagesMr. Jay Narayan YadavAashish ChaudharyNo ratings yet
- Savitri Singh ThyrocareDocument20 pagesSavitri Singh ThyrocareAbhishek SinghNo ratings yet
- MR Santosh Rai: Method: CalculatedDocument10 pagesMR Santosh Rai: Method: CalculatedSantosh RaiNo ratings yet
- PdfText - 2023-10-16T101203.851Document12 pagesPdfText - 2023-10-16T101203.851Sanjana AntilNo ratings yet
- ReportsDocument5 pagesReportsguptaaarushi528No ratings yet
- ReportDocument12 pagesReportSimran jeet kaurNo ratings yet
- Header-1Document5 pagesHeader-1Sanchit NigamNo ratings yet
- HeaderDocument4 pagesHeaderatul kumarNo ratings yet
- Ms. Sathiya.C: Sid No. Patient ID 0400050308Document4 pagesMs. Sathiya.C: Sid No. Patient ID 0400050308Sathya CNo ratings yet
- Diagnostic Report: FinalDocument3 pagesDiagnostic Report: FinalPARTH SARTHI J174No ratings yet
- FastingDocument6 pagesFastingSwiss-Can Interlaken-VancouverNo ratings yet
- Report 220719 195623Document11 pagesReport 220719 195623Abdullah AlviNo ratings yet
- HeaderDocument11 pagesHeaderSrinivas MalladiNo ratings yet
- SR8188385Document2 pagesSR8188385mohanchowdhury1948No ratings yet
- Method: Calculated: Page 1 of 7 15-Jun-2022 01:22 PMDocument8 pagesMethod: Calculated: Page 1 of 7 15-Jun-2022 01:22 PMgunjan pratapNo ratings yet
- 1-Good Health Package - PO2162925017-153Document13 pages1-Good Health Package - PO2162925017-153venkatsidNo ratings yet
- 5047UD1771005047 478961cDocument7 pages5047UD1771005047 478961cVedika ThadhaniNo ratings yet
- Checkup ReportDocument17 pagesCheckup Reportshashwatpandey736No ratings yet
- Shephali Das-85Document3 pagesShephali Das-85Sanjoy DasNo ratings yet
- Diagnostic Report: Client Code: Client'S Name and AddressDocument5 pagesDiagnostic Report: Client Code: Client'S Name and AddressAbhinav AnandNo ratings yet
- And1912900076079253 RLSDocument10 pagesAnd1912900076079253 RLSshiva rama krishna reddiNo ratings yet
- Rama ReportDocument15 pagesRama ReportAnkush NayyarNo ratings yet
- Lab Report NewDocument5 pagesLab Report Newsamirghosal19No ratings yet
- GC129053 (1) - 210804 - 061549Document2 pagesGC129053 (1) - 210804 - 061549anuragNo ratings yet
- Complete Haemogram (Hemogram & Esr) Haemoglobin Total RBC CountDocument5 pagesComplete Haemogram (Hemogram & Esr) Haemoglobin Total RBC Countrohit bharadwazNo ratings yet
- Method: Calculated: Page 1 of 11 19-Jul-2022 04:36 PMDocument12 pagesMethod: Calculated: Page 1 of 11 19-Jul-2022 04:36 PMAashima SharmaNo ratings yet
- Archana Lab ReportDocument10 pagesArchana Lab Reportprabalsoni125No ratings yet
- Quick guide to Laboratory Medicine: a student's overviewFrom EverandQuick guide to Laboratory Medicine: a student's overviewNo ratings yet
- Sample Acceptance & Rejection CriteriaDocument26 pagesSample Acceptance & Rejection CriteriaSayan GhoshalNo ratings yet
- Clinical Hematology Atlas 6Th Edition Jacqueline H Carr Full ChapterDocument67 pagesClinical Hematology Atlas 6Th Edition Jacqueline H Carr Full Chapterkerri.kite140100% (9)
- SharksDocument2 pagesSharksNudy ParedesNo ratings yet
- American AlligatorsDocument11 pagesAmerican Alligatorsapi-394440828No ratings yet
- By Dr. 'Abd Al-Hakam 'Abd Al-Latif as-Sa'IdiDocument1 pageBy Dr. 'Abd Al-Hakam 'Abd Al-Latif as-Sa'IdiadamNo ratings yet
- Alabama Snakes Acitivity BookDocument33 pagesAlabama Snakes Acitivity BookLevi CavalcanteNo ratings yet
- Blood Collection and Preservation - ppt-1-1Document40 pagesBlood Collection and Preservation - ppt-1-1samsonraju07No ratings yet
- Actividades Aicle AnimalsDocument3 pagesActividades Aicle AnimalsMaria Jose VillarrubiaNo ratings yet
- Evolution of FishDocument2 pagesEvolution of FishJered MoratoNo ratings yet
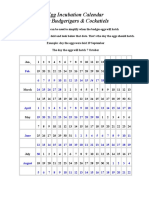
- Egg Incubation Calendar For Budgies and CockatielsDocument2 pagesEgg Incubation Calendar For Budgies and Cockatielsrmcastro72No ratings yet
- Week 7Document5 pagesWeek 7Shafa ArifinNo ratings yet
- Azores Rare and Scarce Bird Report 2013Document73 pagesAzores Rare and Scarce Bird Report 2013Peter Alfrey100% (1)
- Commonly Occurring Birds in GurgaonDocument22 pagesCommonly Occurring Birds in GurgaonUrmila Duhan100% (1)
- Marine Fish For Beginners EbookDocument12 pagesMarine Fish For Beginners Ebookpule rikyNo ratings yet
- Dutch AquariumDocument6 pagesDutch AquariumTom SndNo ratings yet
- W9 FishAnatomy 2019Document6 pagesW9 FishAnatomy 2019Abigail RefeeNo ratings yet
- RH Blood Group SystemDocument38 pagesRH Blood Group SystemMarry Flor CuerdoNo ratings yet
- Introduction To Fishes PDFDocument20 pagesIntroduction To Fishes PDFVikram Raj SinghNo ratings yet
- Kendriya Vidyalaya Sambalpur: Science Project SESSION 2016-17 Topic-Fishes Pujarani Behera Ix - C 16 S.S.Bhoi SirDocument8 pagesKendriya Vidyalaya Sambalpur: Science Project SESSION 2016-17 Topic-Fishes Pujarani Behera Ix - C 16 S.S.Bhoi SirNiranjan BeheraNo ratings yet
- Hemochroma PLUSDocument2 pagesHemochroma PLUSsatujuli23No ratings yet
- Science 4: Life Cycle of A FrogDocument27 pagesScience 4: Life Cycle of A FrogJennifer RagualNo ratings yet
- Dichotomous Key - WorksheetDocument2 pagesDichotomous Key - Worksheetramsha.sadaf2007No ratings yet
- PISCESDocument27 pagesPISCESHamdan FatahNo ratings yet
- Hematocrit Determination (Packed Cell Volume, PCV) (Relative Corpuscular Volume)Document17 pagesHematocrit Determination (Packed Cell Volume, PCV) (Relative Corpuscular Volume)abdoatefelsadanyNo ratings yet
- Amphibian Questions To Eyewitness FilmDocument3 pagesAmphibian Questions To Eyewitness FilmAttila DudasNo ratings yet
- 2023 EDGE Species RT CallDocument488 pages2023 EDGE Species RT CallMohamad HafizudinNo ratings yet
- FeathersDocument3 pagesFeathersvenice ibrahimNo ratings yet
- Freshwater Fishes of Pakistan - 075329Document56 pagesFreshwater Fishes of Pakistan - 075329Bold PersonNo ratings yet
- Science ScrapbookDocument10 pagesScience ScrapbookHilman ハサフ CrazeeNo ratings yet