Download as doc, pdf, or txt
You might also like
- Krav Maga Pressure Points - Military Hand To Hand Combat GuideDocument27 pagesKrav Maga Pressure Points - Military Hand To Hand Combat Guidebrogan98% (135)
- Psychopharmacology 2 AntidepressantsDocument7 pagesPsychopharmacology 2 AntidepressantsBea Samonte100% (2)
- Ziva Meditation Ebook PDFDocument33 pagesZiva Meditation Ebook PDFneeta50% (4)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
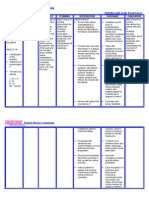
- NURSING CARE PLAN - Breast CancerDocument2 pagesNURSING CARE PLAN - Breast Cancerderic100% (3)
- Chapter 21 Antidepressant AgentsDocument4 pagesChapter 21 Antidepressant AgentsNicolle Lisay IlaganNo ratings yet
- Mantras - English - KundaliniDocument7 pagesMantras - English - KundaliniRPh Krishna Chandra JagritNo ratings yet
- Halberstein - 2005 - Annals of Epidemiology PDFDocument14 pagesHalberstein - 2005 - Annals of Epidemiology PDFWindhy HaningNo ratings yet
- Skimming and Scanning QuizDocument15 pagesSkimming and Scanning Quizeagle777jay0% (1)
- 11 Chapter 2Document8 pages11 Chapter 2Muhammad Tariq RazaNo ratings yet
- 15Document36 pages15michelleNo ratings yet
- Slides Mood DisordersDocument15 pagesSlides Mood DisordersEesha TahirNo ratings yet
- Antidepressant Drugs: Presented By-K.Vinod Dept. of PharmacologyDocument38 pagesAntidepressant Drugs: Presented By-K.Vinod Dept. of PharmacologyVinod GuruNo ratings yet
- Pharmacology of Mood Stabilizers: DR - Datten Bangun, MSC, SPFK Dept - Farmakologi & Terapetik Fak - Kedokteran Uhn MedanDocument51 pagesPharmacology of Mood Stabilizers: DR - Datten Bangun, MSC, SPFK Dept - Farmakologi & Terapetik Fak - Kedokteran Uhn MedanFansisca SiallaganNo ratings yet
- Biology of DepressionDocument5 pagesBiology of DepressionScience RespondsNo ratings yet
- AntidepressantsDocument36 pagesAntidepressantsLloyd Daniel BarrantesNo ratings yet
- "Serotonin Syndrome Causes HARM": Psychiatry PharamacologyDocument9 pages"Serotonin Syndrome Causes HARM": Psychiatry Pharamacologytycobb63100% (4)
- Antidepressants (ME216) 20 5Document40 pagesAntidepressants (ME216) 20 5Dineish MurugaiahNo ratings yet
- Lecture 2 (Psychotropic Drugs)Document17 pagesLecture 2 (Psychotropic Drugs)ahmadslayman1No ratings yet
- Class 1 Antidepressents 2020Document21 pagesClass 1 Antidepressents 2020Arafat 039No ratings yet
- Antidepressent (AutoRecovered)Document11 pagesAntidepressent (AutoRecovered)chakdiva11No ratings yet
- Inhibidores Recep Serotonina 2Document14 pagesInhibidores Recep Serotonina 2FarmaFMNo ratings yet
- Antidepressants AntidepressantsDocument38 pagesAntidepressants AntidepressantsjaneNo ratings yet
- Depression: Types Symptoms Diagnosis Causes TreatmentDocument32 pagesDepression: Types Symptoms Diagnosis Causes TreatmentThea MallariNo ratings yet
- Name: Class: Department: Roll No.: Subject: Course Code: Cr. HR.: Submitted To: Date of Submission: TopicDocument16 pagesName: Class: Department: Roll No.: Subject: Course Code: Cr. HR.: Submitted To: Date of Submission: TopicAnoosha FarooquiNo ratings yet
- Pharmacology 402 February 24, 2010 Mark Hamblin, MD, PHDDocument54 pagesPharmacology 402 February 24, 2010 Mark Hamblin, MD, PHDKarmila Novianti100% (1)
- Anti-Depressants: Bitek BrianDocument28 pagesAnti-Depressants: Bitek BrianMwanja MosesNo ratings yet
- Depression: Psychiatric DisordersDocument21 pagesDepression: Psychiatric DisordersNdoo NdooNo ratings yet
- Antidepressants: Samaiya Mushtaq CHEM 5398Document33 pagesAntidepressants: Samaiya Mushtaq CHEM 5398Renuga DeviNo ratings yet
- Extrapyramidal SymptomsDocument5 pagesExtrapyramidal SymptomsGenette Sy SolisNo ratings yet
- Artigo Fisiopato DepressãoDocument21 pagesArtigo Fisiopato DepressãoJ VichhyNo ratings yet
- Transmitters and Disorders HandoutDocument3 pagesTransmitters and Disorders HandoutfrazzycakebossNo ratings yet
- Treatment of Depressive DisordersDocument96 pagesTreatment of Depressive DisordersAbelNo ratings yet
- Neurobiologi Depresi 2000 WFDocument6 pagesNeurobiologi Depresi 2000 WFKim AntelNo ratings yet
- AntidepressantsDocument28 pagesAntidepressantsakoeljames8543No ratings yet
- W3 Bipolar Disorder. Therapies. T2 2022-23Document41 pagesW3 Bipolar Disorder. Therapies. T2 2022-23Nayanaa VarsaaleNo ratings yet
- Slides SchizophreniaDocument28 pagesSlides SchizophreniaEesha TahirNo ratings yet
- Chapter 46 - 50Document74 pagesChapter 46 - 50mer12sswNo ratings yet
- Biological FactorsDocument3 pagesBiological FactorsDEEPIKA PREMLAL 2170101No ratings yet
- Antidepressant DrugsDocument55 pagesAntidepressant Drugsmaheen aurangzaib100% (2)
- Antidepressants AntianxietyDocument95 pagesAntidepressants AntianxietyCharles YiuNo ratings yet
- B2B Psychopharmacology 2015Document128 pagesB2B Psychopharmacology 2015Soleil DaddouNo ratings yet
- Depressive - EtiologyDocument35 pagesDepressive - EtiologygunjaNo ratings yet
- Antidepressant DrugsDocument47 pagesAntidepressant DrugsOjambo Flavia75% (4)
- Antidepressants and Treatment of Mood DisordersDocument24 pagesAntidepressants and Treatment of Mood DisordersFuad HadiNo ratings yet
- InsomniaDocument3 pagesInsomniaYudi MahardikaNo ratings yet
- Antidepressants ChristianDocument37 pagesAntidepressants ChristianciaranNo ratings yet
- Clinical PharmacologyDocument29 pagesClinical PharmacologyBilal KhanNo ratings yet
- Antidepressant DrugsDocument15 pagesAntidepressant DrugsDr. Mushfique Imtiaz ChowdhuryNo ratings yet
- Depression Theory PDFDocument2 pagesDepression Theory PDFdonkeyendutNo ratings yet
- Biological Therapies For Depression: Ask YourselfDocument6 pagesBiological Therapies For Depression: Ask YourselfAnni Christoforou100% (1)
- Antidepressant AgentsDocument45 pagesAntidepressant Agentsmadeha goharNo ratings yet
- AntidepressantsDocument59 pagesAntidepressantsanon_189054600100% (2)
- DepressionDocument26 pagesDepressionkanwalsweetNo ratings yet
- L7-Depression and BipolarDocument36 pagesL7-Depression and Bipolar120420314No ratings yet
- Antidepreesent AgentsDocument34 pagesAntidepreesent Agentsmaryamkefahn2003No ratings yet
- The PSYCH MAP ColoredDocument2 pagesThe PSYCH MAP Coloredcentrino17No ratings yet
- 3 Anti-Depressant DrugsDocument30 pages3 Anti-Depressant DrugsAjigotto ubiq.No ratings yet
- HypothesisDocument2 pagesHypothesisJomana MacalnasNo ratings yet
- WahabDocument7 pagesWahabwahabahmad4604No ratings yet
- Lecture 7bDocument8 pagesLecture 7bBetty MaiNo ratings yet
- The Nervous System: Blood Brain BarrierDocument17 pagesThe Nervous System: Blood Brain BarrierSuleiman AbdallahNo ratings yet
- Anti Depressants 2Document24 pagesAnti Depressants 2Ayesha AyeshaNo ratings yet
- Antidepressants Ssris, Snris: Selective Serotonin Reuptake Inhibitors Norepinephrine Reuptake InhibitorsDocument23 pagesAntidepressants Ssris, Snris: Selective Serotonin Reuptake Inhibitors Norepinephrine Reuptake InhibitorsJosh SchultzNo ratings yet
- Michelle Gillis - Phenylethylamine: More Than Just A Pea-Sized NeurochemicalDocument3 pagesMichelle Gillis - Phenylethylamine: More Than Just A Pea-Sized NeurochemicalNeerFamNo ratings yet
- نسخة ANTI-ARRHYTHMIC 2Document28 pagesنسخة ANTI-ARRHYTHMIC 2ManWol JangNo ratings yet
- Matrimonial Resume CVDocument3 pagesMatrimonial Resume CVRPh Krishna Chandra Jagrit76% (37)
- About MeningiomaDocument5 pagesAbout MeningiomaRPh Krishna Chandra JagritNo ratings yet
- Matrimonial Resume CVDocument3 pagesMatrimonial Resume CVRPh Krishna Chandra Jagrit76% (37)
- HTML-XHTML Tag SheDocument6 pagesHTML-XHTML Tag SheabcjohnNo ratings yet
- Matrimonial Resume CVDocument3 pagesMatrimonial Resume CVRPh Krishna Chandra Jagrit76% (37)
- About This Tutorial: Version HistoryDocument328 pagesAbout This Tutorial: Version HistoryKate CorralesNo ratings yet
- MantrasDocument24 pagesMantrasg_gaurishankar@rediffmail.com100% (4)
- Super Fast Mental Math - Vedic Math HistoryDocument51 pagesSuper Fast Mental Math - Vedic Math Historyvedicmath98% (42)
- Martial Arts - Bruce Lee's Training SecretsDocument3 pagesMartial Arts - Bruce Lee's Training Secretsbrogan91% (34)
- Martial Arts - Bruce Lee's Speed TrainingDocument4 pagesMartial Arts - Bruce Lee's Speed Trainingbrogan97% (33)
- Web DesigningDocument638 pagesWeb DesigningRPh Krishna Chandra JagritNo ratings yet
- Math Olympiad Problems Collection-V1Document97 pagesMath Olympiad Problems Collection-V1RPh Krishna Chandra Jagrit100% (1)
- Tally 9.2 NotesDocument1,918 pagesTally 9.2 NotesRamesh80% (5)
- Introduction in Human AnatomyDocument60 pagesIntroduction in Human AnatomyRPh Krishna Chandra JagritNo ratings yet
- Medicinal PlantsDocument29 pagesMedicinal PlantsGANESH KUMAR JELLANo ratings yet
- General KnowledgeDocument141 pagesGeneral KnowledgeRAVI KUMAR83% (12)
- General Pharmacology MCQDocument6 pagesGeneral Pharmacology MCQShrikant ThakurNo ratings yet
- Curriculum VitaeDocument2 pagesCurriculum VitaeRPh Krishna Chandra JagritNo ratings yet
- Aspire Products, The Makers of EMST150, Announces A New & Improved WebsiteDocument2 pagesAspire Products, The Makers of EMST150, Announces A New & Improved WebsiteAlexandra HartNo ratings yet
- Romsons All ProductDocument53 pagesRomsons All ProductBoyke WinterbergNo ratings yet
- Acupuncture For BurnsDocument34 pagesAcupuncture For BurnsIvonne Flores FernándezNo ratings yet
- Contact Dermatitis Guidelines 2017Document13 pagesContact Dermatitis Guidelines 2017Imam Muhamad RissandyNo ratings yet
- Anaesthesia - 2021 - Feray - PROSPECT Guidelines For Video Assisted Thoracoscopic Surgery A Systematic Review andDocument15 pagesAnaesthesia - 2021 - Feray - PROSPECT Guidelines For Video Assisted Thoracoscopic Surgery A Systematic Review andboby abdul rahmanNo ratings yet
- Evolution Occlusion and Occlusal Instruments: AcademicsDocument11 pagesEvolution Occlusion and Occlusal Instruments: AcademicsMelissa Perez GuerreroNo ratings yet
- Diclofenac: Mechanism of ActionDocument7 pagesDiclofenac: Mechanism of ActionaditNo ratings yet
- J 1600-0757 1998 tb00129 PDFDocument6 pagesJ 1600-0757 1998 tb00129 PDFdwinugrohojuandaNo ratings yet
- My - Lectures.Updated - II 2015Document137 pagesMy - Lectures.Updated - II 2015prasadmvk100% (1)
- Cerenia Combo PI May2012Document2 pagesCerenia Combo PI May2012wvhvet100% (1)
- Antalya Medical Tourism Guide 2014Document59 pagesAntalya Medical Tourism Guide 2014pilgrim13No ratings yet
- Basic Foundation of Iv TherapyDocument10 pagesBasic Foundation of Iv Therapyjanna mae patriarcaNo ratings yet
- AcsDocument103 pagesAcsVikrant WankhedeNo ratings yet
- Nephrology Curriculum - الزمالة المصرية للكليDocument60 pagesNephrology Curriculum - الزمالة المصرية للكليbook1man100% (1)
- Curriculum Vitae: 1. Personal Details: Ms. Jayanthi.JDocument6 pagesCurriculum Vitae: 1. Personal Details: Ms. Jayanthi.JRadha ThangamNo ratings yet
- Immunotherapy Post TransplantDocument12 pagesImmunotherapy Post TransplantaymenNo ratings yet
- Humms 11 Pasay Diass s2 q1 w4Document20 pagesHumms 11 Pasay Diass s2 q1 w4Victoria De Los SantosNo ratings yet
- Thoma 2015Document39 pagesThoma 2015Izabella de LimaNo ratings yet
- MCQ PneuDocument60 pagesMCQ PneuYanesh Bishundat0% (1)
- Azithromycin in PediatricsDocument40 pagesAzithromycin in PediatricsKishore ChandkiNo ratings yet
- HPLP II-English VersionDocument3 pagesHPLP II-English VersionGarr LordemadNo ratings yet
- Cyst and Cystlike Lung LesionsDocument57 pagesCyst and Cystlike Lung LesionsAna StankovicNo ratings yet
- Enrofloxacin: Therapeutic ReviewDocument4 pagesEnrofloxacin: Therapeutic ReviewAndi Dytha Pramitha SamNo ratings yet
- RADIOLOGYDocument3 pagesRADIOLOGYwendy carinoNo ratings yet
- An Introduction To Grounding: The Healing Chalet in The WoodsDocument7 pagesAn Introduction To Grounding: The Healing Chalet in The Woodse.j.wardNo ratings yet