You might also like
- The Present and Future of Bispecific Antibodies For Cancer TherapyDocument19 pagesThe Present and Future of Bispecific Antibodies For Cancer Therapyvignezh1No ratings yet
- Foods To Fight Cancer - What To Eat PDFDocument242 pagesFoods To Fight Cancer - What To Eat PDFdokundot86% (7)
- Seeing The UnseenDocument8 pagesSeeing The UnseenCale HollowayNo ratings yet
- AtlasDocument56 pagesAtlasKolea HanganuNo ratings yet
- Gerontologic NursingDocument231 pagesGerontologic NursingKirk08100% (2)
- Discharge PlanDocument5 pagesDischarge PlanYa Mei Li100% (1)
- Statement of Deficiencies and Plan of Correction For Andbe Home (Via DHHS)Document12 pagesStatement of Deficiencies and Plan of Correction For Andbe Home (Via DHHS)NTV NewsNo ratings yet
- Reading Review TOEFL Exercise (Skill 1 - 7)Document2 pagesReading Review TOEFL Exercise (Skill 1 - 7)LussyAlbayinnah100% (1)
- Common Childhood Solid Tumors (Part 2)Document56 pagesCommon Childhood Solid Tumors (Part 2)Princess Aira Bucag CarbonelNo ratings yet
- PNET, Pineal TumorsDocument58 pagesPNET, Pineal TumorsGed OlayanNo ratings yet
- BRAIN Tumors PDFDocument44 pagesBRAIN Tumors PDFHalima Assi100% (1)
- Brain CancerDocument186 pagesBrain CancerAlin BlagaNo ratings yet
- M Sandamela Salivary Gland SandamelaDocument45 pagesM Sandamela Salivary Gland SandamelaRockson SamuelNo ratings yet
- Solitary Thyroid Nodule Done by Dr. Dana Al-Zarraq Supervised y Dr. Saleh HammadDocument50 pagesSolitary Thyroid Nodule Done by Dr. Dana Al-Zarraq Supervised y Dr. Saleh HammadMohammad BanisalmanNo ratings yet
- Brain TumorsDocument78 pagesBrain Tumorsnarswiponshistoryan100% (3)
- MedulloblastomaDocument29 pagesMedulloblastomaFaizyabNo ratings yet
- Ped Onc For ENT 091216Document28 pagesPed Onc For ENT 091216Justine NyangaresiNo ratings yet
- Testicular CancerDocument48 pagesTesticular Cancerluckyswiss7776848No ratings yet
- Neuroblastoma EAUDocument86 pagesNeuroblastoma EAUaemy13266No ratings yet
- Neoplasms of Testis NishDocument54 pagesNeoplasms of Testis NishRamesh ReddyNo ratings yet
- Thyroid CarcinomaDocument27 pagesThyroid CarcinomaGanesh MarutinathNo ratings yet
- Thyroid CancerDocument38 pagesThyroid CancerNinikNo ratings yet
- Katelyn Fernando Presentation MedulloblastomaDocument25 pagesKatelyn Fernando Presentation Medulloblastomaapi-543045416No ratings yet
- RetinoblastomaDocument72 pagesRetinoblastomaDr-Muhammad IsrarNo ratings yet
- Testicular Tumours 2020Document55 pagesTesticular Tumours 2020Ramesh ReddyNo ratings yet
- Carcinoma Thyroid: Diagnosis and Management: Professor Ravi KantDocument51 pagesCarcinoma Thyroid: Diagnosis and Management: Professor Ravi KantMubarakDiedaNo ratings yet
- RETINOBLASTOMA, DR Claudio Owino, SurgeryDocument30 pagesRETINOBLASTOMA, DR Claudio Owino, SurgeryKaruga NyagahNo ratings yet
- Papillary Thyroid CarcinomaDocument9 pagesPapillary Thyroid CarcinomaELinkTulusNo ratings yet
- Parapharyngeal Space TumorsDocument60 pagesParapharyngeal Space TumorsHossam ThabetNo ratings yet
- Melanoma: Edward Buckingham, M.D. Combined Plastics Conference September 6, 2000Document53 pagesMelanoma: Edward Buckingham, M.D. Combined Plastics Conference September 6, 2000Kadek Ariarta MahartamaNo ratings yet
- Approach To Thyroid MalignancyDocument9 pagesApproach To Thyroid MalignancyHuda Al-AnabrNo ratings yet
- Thyroid NodulesDocument9 pagesThyroid Nodulesmarselia23No ratings yet
- Brain Tumours PresentationDocument19 pagesBrain Tumours PresentationBonfaceNo ratings yet
- Management of Brain MetsDocument53 pagesManagement of Brain MetsDSankhlaudrNo ratings yet
- Tumors of CNS: MBBS, FCPS, M.Phil. Histopathology Department of PathologyDocument23 pagesTumors of CNS: MBBS, FCPS, M.Phil. Histopathology Department of PathologyOga bogaNo ratings yet
- Malignant Diseases of The OvaryDocument64 pagesMalignant Diseases of The OvaryGÖKSU SAYGILINo ratings yet
- Tumor OtakDocument47 pagesTumor OtaksekiannNo ratings yet
- GTD For CIsDocument82 pagesGTD For CIsDegefaw BikoyNo ratings yet
- Cerebral Metastasis: Syed Maroof AliDocument28 pagesCerebral Metastasis: Syed Maroof AliMaroofAliNo ratings yet
- Childhood Solid Tumors: For C-1 StudentsDocument72 pagesChildhood Solid Tumors: For C-1 StudentsYemata HailuNo ratings yet
- Papillary and Follicular Thyroid Cancer: K. A. Ikram Hussain Final Year M.B.B.SDocument26 pagesPapillary and Follicular Thyroid Cancer: K. A. Ikram Hussain Final Year M.B.B.SAhsan JamilNo ratings yet
- MedulloblastomaDocument17 pagesMedulloblastomabrown_chocolate87643No ratings yet
- Epk FDocument73 pagesEpk FBryan FjbNo ratings yet
- Craniopharyngioma Simon Brown TalkDocument38 pagesCraniopharyngioma Simon Brown TalkOka Iramda SaputraNo ratings yet
- Discuss The Principles of Management of Solitary ThyroidDocument46 pagesDiscuss The Principles of Management of Solitary ThyroidNdenwaneku OkuwaNo ratings yet
- Tumor IntraabdomenDocument30 pagesTumor IntraabdomenBedahanakugmNo ratings yet
- Thyroid Cancer PDFDocument67 pagesThyroid Cancer PDFJaredNo ratings yet
- Ca ThyroidDocument49 pagesCa Thyroidfaiz NNo ratings yet
- Papillar y and Follicula R Thyroi D Cancer: K. A. Ikram Hussain Final Year M.B.B.SDocument26 pagesPapillar y and Follicula R Thyroi D Cancer: K. A. Ikram Hussain Final Year M.B.B.SAhsan JamilNo ratings yet
- Brain Cancer: by Cara KlingamanDocument16 pagesBrain Cancer: by Cara KlingamanLouis FortunatoNo ratings yet
- Salivary Gland NeoplasmsDocument63 pagesSalivary Gland Neoplasmsyashwanth bNo ratings yet
- Journal Club: Dr. Preethi.S DNB Resident Ent 31/03/23Document27 pagesJournal Club: Dr. Preethi.S DNB Resident Ent 31/03/23PreethiNo ratings yet
- Squamous Cell CarcinomaDocument53 pagesSquamous Cell CarcinomaWacky BlankNo ratings yet
- Li FraumeniDocument28 pagesLi FraumeniPaigeNo ratings yet
- Laryngeal Mass: John F. Mcguire, MD, MbaDocument33 pagesLaryngeal Mass: John F. Mcguire, MD, MbaIvan DarioNo ratings yet
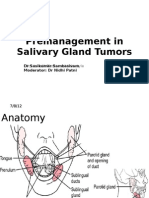
- Premanagement in Salivary Gland TumorsDocument40 pagesPremanagement in Salivary Gland TumorsDr Sasikumar SambasivamNo ratings yet
- Salivary 020Document74 pagesSalivary 020Dirga Rasyidin LNo ratings yet
- Null - PDF 3Document24 pagesNull - PDF 3مهند حسام محمد سعيد عبدNo ratings yet
- Tumors of TestisDocument25 pagesTumors of TestisYazeed AsrawiNo ratings yet
- Thyroid NeoplasmsDocument62 pagesThyroid Neoplasmshemanarasimha gandikotaNo ratings yet
- Solitary Nodules Are Most Likely To Be Malignant in Patients Older Than 60 Years and in Patients Younger Than 30 YearsDocument5 pagesSolitary Nodules Are Most Likely To Be Malignant in Patients Older Than 60 Years and in Patients Younger Than 30 YearsAbdurrahman Afa HaridhiNo ratings yet
- The Evaluation and Management of Neck Masses of Unknown EtiologyDocument38 pagesThe Evaluation and Management of Neck Masses of Unknown EtiologyShaxawan Mahmood AliNo ratings yet
- Thyroid Diseases 3 NeoplasmDocument30 pagesThyroid Diseases 3 NeoplasmSolomon Fallah Foa SandyNo ratings yet
- Thyroid Malignancies: DR Rajesh P SDocument37 pagesThyroid Malignancies: DR Rajesh P SdrrajeshpsmsNo ratings yet
- Neoplastic Thyroid Disease ThyroidDocument74 pagesNeoplastic Thyroid Disease ThyroidpedramshakerinavaNo ratings yet
- Inde222 11 09 2015 11 Lect Higgins 1Document59 pagesInde222 11 09 2015 11 Lect Higgins 1Tri Novita SariNo ratings yet
- Endocrine EditedDocument130 pagesEndocrine EditedKirk08No ratings yet
- Concept On Immune Response and Inflammation REVISEDDocument163 pagesConcept On Immune Response and Inflammation REVISEDKirk08100% (1)
- Immune Deficinecy: By: Kirk Odrey O. Jimenez R.NDocument51 pagesImmune Deficinecy: By: Kirk Odrey O. Jimenez R.NKirk08No ratings yet
- Congenital Neurologic DisordersDocument114 pagesCongenital Neurologic DisordersKirk08No ratings yet
- Triage Color CodingDocument7 pagesTriage Color CodingKirk08100% (1)
- Aging PopulationDocument34 pagesAging PopulationKirk0867% (3)
- Neurologic Care NursingDocument439 pagesNeurologic Care NursingKirk08No ratings yet
- Formed Elements of The BloodDocument88 pagesFormed Elements of The BloodKirk08No ratings yet
- Daftar PustakaDocument2 pagesDaftar PustakaBasmalah EhmNo ratings yet
- L4 U03 LA RC - DecryptedDocument3 pagesL4 U03 LA RC - Decryptedkrkshkn100% (1)
- VETRII CA (English) July2023-March2024Document159 pagesVETRII CA (English) July2023-March2024Thiru98No ratings yet
- The Hemodialysis Prescription Past, Present, And.18Document4 pagesThe Hemodialysis Prescription Past, Present, And.18Tim Engineer HD RSUD Dr. SoetomoNo ratings yet
- The One Minute PreceptorDocument8 pagesThe One Minute PreceptorRannia ShehrishNo ratings yet
- Chemistry Project: Study of Adultrants in FoodDocument21 pagesChemistry Project: Study of Adultrants in Foodmohit pandeyNo ratings yet
- Casuga-Eroshanzjearue JournalanalysisDocument2 pagesCasuga-Eroshanzjearue JournalanalysisEros SmithNo ratings yet
- 0 - Rno. 02 Unani, Homeopathy System of MedicineDocument29 pages0 - Rno. 02 Unani, Homeopathy System of MedicineSakshi ChodankarNo ratings yet
- HY Endocrine UsmleDocument22 pagesHY Endocrine UsmleNakhal JararNo ratings yet
- Lower ExtremitiesDocument14 pagesLower ExtremitiesNicko PerezNo ratings yet
- Winawer Et Al-2018-Annals of NeurologyDocument14 pagesWinawer Et Al-2018-Annals of NeurologyAndoingNo ratings yet
- The Miracle Tree: Current Status of Available Knowledge: Euphorbia Tirucalli L. (Euphorbiaceae)Document10 pagesThe Miracle Tree: Current Status of Available Knowledge: Euphorbia Tirucalli L. (Euphorbiaceae)Lucas Meirelles SiqueiraNo ratings yet
- NCH Safe Pregnancy BrochureDocument6 pagesNCH Safe Pregnancy BrochurenehahNo ratings yet
- PIIS170121631730261XDocument4 pagesPIIS170121631730261XNina TorreblancaNo ratings yet
- Standard Operating Procedure (SOP)Document2 pagesStandard Operating Procedure (SOP)Rudrajit KarguptaNo ratings yet
- Alcoholhistory PDFDocument14 pagesAlcoholhistory PDFRupali RajputNo ratings yet
- Crops ClassificationDocument14 pagesCrops ClassificationMoiz Khan YousufzaiNo ratings yet
- Gadtc PHCDocument246 pagesGadtc PHCshawnNo ratings yet
- Review of SystemsDocument13 pagesReview of SystemsDenz Marc AleaNo ratings yet
- Biotechnology Old Question PaperDocument10 pagesBiotechnology Old Question PaperHarshitNo ratings yet
- SYNOPSISDocument18 pagesSYNOPSISsameer jadhavNo ratings yet
- Gels 10 00188Document46 pagesGels 10 00188mkhubaibNo ratings yet
- Skva SummaryDocument1 pageSkva SummarydaibysenekaNo ratings yet
- Preoperative Assessment of The Patient With Heart Disease Case FileDocument2 pagesPreoperative Assessment of The Patient With Heart Disease Case Filehttps://medical-phd.blogspot.comNo ratings yet