Download as doc, pdf, or txt
You might also like
- Ferosac InjDocument2 pagesFerosac InjMohamed Taleb75% (4)
- Pharmacology 2 Final Exam 2021-NkDocument16 pagesPharmacology 2 Final Exam 2021-NkT'amo HanashNo ratings yet
- ASSIGNMENT ON DRUGS AND PROCEDURES PERMITTED TO BE USED BY NURSE MIDWIVES BY GoIDocument5 pagesASSIGNMENT ON DRUGS AND PROCEDURES PERMITTED TO BE USED BY NURSE MIDWIVES BY GoIannu panchal100% (1)
- Metabolic Stress Case StudyDocument10 pagesMetabolic Stress Case StudydakotaNo ratings yet
- Psych Clinic Intake & Report OutlineDocument4 pagesPsych Clinic Intake & Report OutlineJulie Anne DeeNo ratings yet
- IVIron IGDocument12 pagesIVIron IGLorenz Joey RicarteNo ratings yet
- Nutrition in Pregnancy & AnaemiaDocument60 pagesNutrition in Pregnancy & AnaemiamohamadehabNo ratings yet
- MATERI 6 Mek. Toksisitas (Overdose)Document7 pagesMATERI 6 Mek. Toksisitas (Overdose)PERMATASARI BKUNo ratings yet
- Problems With The Thyroid GlandDocument10 pagesProblems With The Thyroid GlandElla Marie CruzadaNo ratings yet
- Curative Treatment of IDADocument40 pagesCurative Treatment of IDARakshita JainNo ratings yet
- Drug Guideline For Iron Polymaltose InjectionDocument7 pagesDrug Guideline For Iron Polymaltose Injectionmirza_baig_46No ratings yet
- Ferrous Sulfate Fer-In-SolDocument2 pagesFerrous Sulfate Fer-In-SolMilagrosMariaLlanosMamaniNo ratings yet
- Hematinics-Reading MaterialsDocument3 pagesHematinics-Reading MaterialsbNo ratings yet
- Hypothyroidism TestDocument6 pagesHypothyroidism TestVrushaliNo ratings yet
- Low Molecular Weight Heparins (LMWH) : I. Mechanism of ActionDocument7 pagesLow Molecular Weight Heparins (LMWH) : I. Mechanism of ActionIniya RajendranNo ratings yet
- Ferrous Sulphate NeomedDocument3 pagesFerrous Sulphate NeomedShuaib KauchaliNo ratings yet
- Oral and Parenteral Iron Preparations in PregnancyDocument45 pagesOral and Parenteral Iron Preparations in PregnancyArun George100% (3)
- Assessment TAsk PharmacodynamicsDocument2 pagesAssessment TAsk PharmacodynamicsMelvin Lazaro CabusoNo ratings yet
- Daunorubicin Hydrochloride IV Over 6 Hours On Days 1, 3, and 5, and Etoposide IV Over 4Document4 pagesDaunorubicin Hydrochloride IV Over 6 Hours On Days 1, 3, and 5, and Etoposide IV Over 4Mohammed HaiderNo ratings yet
- Management of Anaemia in PregnancyDocument8 pagesManagement of Anaemia in PregnancyAnonymous 9dVZCnTXSNo ratings yet
- Mastery Test 2 On MS 1Document17 pagesMastery Test 2 On MS 1Rika MaeNo ratings yet
- Extended Infusion Beta-Lactams ProtocolDocument9 pagesExtended Infusion Beta-Lactams ProtocolKanaga6432No ratings yet
- 9.2016. Parenteral Iron Therapy For Ida in PregnancyDocument2 pages9.2016. Parenteral Iron Therapy For Ida in PregnancynaquibroslanNo ratings yet
- Preparations of Intravenous IronDocument5 pagesPreparations of Intravenous IronSri Siti KhadijahElfNo ratings yet
- 2 - Canine and Feline Anesthesia GuidelinesDocument14 pages2 - Canine and Feline Anesthesia Guidelinesunknowen 22No ratings yet
- Amphotericin B Infusion ProtocolDocument1 pageAmphotericin B Infusion ProtocolNatasha MunapNo ratings yet
- Daunorubicin Hydrochloride IV Over 6 Hours On Days 1, 3, and 5, and Etoposide IV Over 4Document3 pagesDaunorubicin Hydrochloride IV Over 6 Hours On Days 1, 3, and 5, and Etoposide IV Over 4Mohammed HaiderNo ratings yet
- Pharmacology Adrenal GlandsDocument3 pagesPharmacology Adrenal GlandsMarc FosterNo ratings yet
- Administration of FerinjectDocument5 pagesAdministration of FerinjectSalma Al nemriNo ratings yet
- Ob ReviewerDocument6 pagesOb Reviewerjanelle tapiruNo ratings yet
- DesferalDocument11 pagesDesferalFalisha Belvia KairinNo ratings yet
- Long Quiz Drugs For Endocrinologic DisordersDocument4 pagesLong Quiz Drugs For Endocrinologic Disorderspay tinapayNo ratings yet
- Understanding Medical Surgical Nursing - 0845-0845Document1 pageUnderstanding Medical Surgical Nursing - 0845-0845Anas TasyaNo ratings yet
- Iron Supplement - During Pregnancy, Requirements For Iron IncreaseDocument1 pageIron Supplement - During Pregnancy, Requirements For Iron Increasegeorgeloto12No ratings yet
- FCM InsertDocument1 pageFCM InsertFida MarvatNo ratings yet
- DISP-CalculationsWorksheetLab LecDocument4 pagesDISP-CalculationsWorksheetLab LecRafaelaNo ratings yet
- Imidocarb Summary Report 2 Committee Veterinary Medicinal Products enDocument6 pagesImidocarb Summary Report 2 Committee Veterinary Medicinal Products enGilsson FigueroaNo ratings yet
- Thyroid & Antithyroid Drugs - 2020Document7 pagesThyroid & Antithyroid Drugs - 2020ireneNo ratings yet
- ObsNGyn - Medical Disorders in Pregnancy AtfDocument15 pagesObsNGyn - Medical Disorders in Pregnancy Atfosman nurNo ratings yet
- SMILE (Etoposide, Ifosfamide, Methotrexate and Dexamethasone)Document7 pagesSMILE (Etoposide, Ifosfamide, Methotrexate and Dexamethasone)SolikinNo ratings yet
- PharmacoDocument4 pagesPharmacoRouie Björn ABrianNo ratings yet
- Cuarta ParteDocument15 pagesCuarta ParterrhhNo ratings yet
- CancerDocument14 pagesCancerClara De Guzman83% (6)
- BloodDocument27 pagesBloodPATRICK ROSHAN ANo ratings yet
- Tutorial 2 - KGDocument4 pagesTutorial 2 - KGAbdurRahmanShafiNo ratings yet
- I. See Also: MyocardiumDocument4 pagesI. See Also: MyocardiumGiorgi NanetashviliNo ratings yet
- Ati Pharmacology Proctored ExamDocument4 pagesAti Pharmacology Proctored Examkinyuaboris990No ratings yet
- Human Albumin Prescription - AdministrationDocument4 pagesHuman Albumin Prescription - AdministrationKarissa MagaruNo ratings yet
- SQC ABx Guidelines 2-21-2011 PDFDocument2 pagesSQC ABx Guidelines 2-21-2011 PDFMinh SteveNo ratings yet
- Amoxicillin 125 MG 250 MG 5 ML Oral SuspensionDocument16 pagesAmoxicillin 125 MG 250 MG 5 ML Oral SuspensionAshrafNo ratings yet
- Boston Medical Center Maternity Care Guideline Guideline: Iron Defficiency Anemia Accepted: Updated: 04/2015Document4 pagesBoston Medical Center Maternity Care Guideline Guideline: Iron Defficiency Anemia Accepted: Updated: 04/2015Fernando Cardenas AriasNo ratings yet
- 35 Items Saunders Fluids and ElectrolytesDocument4 pages35 Items Saunders Fluids and ElectrolytesKrystelle Jade LabineNo ratings yet
- Pre Exam Answers I FoundDocument73 pagesPre Exam Answers I FoundDuy LuuNo ratings yet
- Ferrous Sulfate Syrup InsertDocument6 pagesFerrous Sulfate Syrup InsertPrincess TiongsonNo ratings yet
- Iron Deficiency Anemia in Pregnant Woman (RAD)Document24 pagesIron Deficiency Anemia in Pregnant Woman (RAD)Radziah Abd malekNo ratings yet
- Anemia in Pregnancy by MahreeDocument53 pagesAnemia in Pregnancy by MahreesherzadmahreeNo ratings yet
- Pharmacy & Medical Store Procedure.Document22 pagesPharmacy & Medical Store Procedure.Google BdNo ratings yet
- Iron Isomaltoside Monofer Final April 2011 Amended 030511 For WebsiteDocument8 pagesIron Isomaltoside Monofer Final April 2011 Amended 030511 For WebsiteUmaima faizNo ratings yet
- IV PO Conversion CAPDocument3 pagesIV PO Conversion CAPdamondouglasNo ratings yet
- PIs Drug InteractionDocument1 pagePIs Drug InteractiondamondouglasNo ratings yet
- IV PO Conversion P&P.V2Document3 pagesIV PO Conversion P&P.V2damondouglasNo ratings yet
- University of Maryland Medical Center Fluconazole (Diflucan®)Document6 pagesUniversity of Maryland Medical Center Fluconazole (Diflucan®)damondouglasNo ratings yet
- Restricted AntimicrobialsDocument1 pageRestricted AntimicrobialsdamondouglasNo ratings yet
- Antimicrobial Renal DosingDocument5 pagesAntimicrobial Renal DosingdamondouglasNo ratings yet
- CAP Guidelines For UseDocument11 pagesCAP Guidelines For Usedamondouglas100% (1)
- CAP AlgorithmDocument1 pageCAP AlgorithmdamondouglasNo ratings yet
- 3.E.2-Caspofungin Guideline 2003Document3 pages3.E.2-Caspofungin Guideline 2003damondouglasNo ratings yet
- Sedation Pain AlgorithmDocument1 pageSedation Pain Algorithmdamondouglas100% (2)
- Perioperative Antibiotics For Surgical ProphylaxisDocument1 pagePerioperative Antibiotics For Surgical ProphylaxisdamondouglasNo ratings yet
- Sodium Content of Inject Able AntibioticsDocument1 pageSodium Content of Inject Able AntibioticsdamondouglasNo ratings yet
- Antibiogram 07Document1 pageAntibiogram 07damondouglas100% (1)
- CAP Guidelines For UseDocument11 pagesCAP Guidelines For Usedamondouglas100% (1)
- PONV GuidelinesDocument3 pagesPONV GuidelinesdamondouglasNo ratings yet
- IV Insulin - FinalDocument18 pagesIV Insulin - Finaldamondouglas100% (2)
- Opioid Equianalgesic ChartDocument1 pageOpioid Equianalgesic Chartdamondouglas100% (7)
- Hypertensive Urgency EmergencyDocument5 pagesHypertensive Urgency Emergencydamondouglas100% (3)
- NSAID Agonist Antagonist TableDocument1 pageNSAID Agonist Antagonist TabledamondouglasNo ratings yet
- IV PO ConversionsDocument1 pageIV PO Conversionsdamondouglas100% (1)
- GCC Anti Emetic Guidelines 2003Document2 pagesGCC Anti Emetic Guidelines 2003damondouglasNo ratings yet
- Practice Guidelines: Enteral Nutrition Delivery For The Adult PatientDocument15 pagesPractice Guidelines: Enteral Nutrition Delivery For The Adult Patientdamondouglas100% (1)
- HIT ProtocolDocument1 pageHIT ProtocoldamondouglasNo ratings yet
- IV PO Conversion CAPDocument3 pagesIV PO Conversion CAPdamondouglasNo ratings yet
- Hyperglycemia Algorithm 2Document1 pageHyperglycemia Algorithm 2damondouglasNo ratings yet
- Antifungal GuidelineDocument2 pagesAntifungal GuidelinedamondouglasNo ratings yet
- Clostridium Difficile Guideline - UMMCDocument5 pagesClostridium Difficile Guideline - UMMCdamondouglas100% (3)
- Calcium Gluconate Infusion Guideline For Use in CVVHDDocument1 pageCalcium Gluconate Infusion Guideline For Use in CVVHDdamondouglas100% (1)
- Calcium Dosing For PediatricsDocument1 pageCalcium Dosing For PediatricsdamondouglasNo ratings yet
- Antibiotic Dosing ESRDDocument6 pagesAntibiotic Dosing ESRDdamondouglas100% (3)
- RhabdovirusDocument74 pagesRhabdovirustummalapalli venkateswara raoNo ratings yet
- So You Want To Be A Urologist?: The First StepDocument2 pagesSo You Want To Be A Urologist?: The First StepDrThamma ShahiNo ratings yet
- Steroid Hyperglycemia: Prevalence, Early Detection and Therapeutic Recommendations: A Narrative ReviewDocument10 pagesSteroid Hyperglycemia: Prevalence, Early Detection and Therapeutic Recommendations: A Narrative ReviewMade Dedy KusnawanNo ratings yet
- 2011 Primary (Arabic Board)Document25 pages2011 Primary (Arabic Board)Mustafa Ismael NayyefNo ratings yet
- Dissociative Identity Disorder (DID) : Presented By: Joseph Rafael B. MasingDocument15 pagesDissociative Identity Disorder (DID) : Presented By: Joseph Rafael B. MasingIan Francis RojasNo ratings yet
- AIPGMEE 2006 Question PaperDocument96 pagesAIPGMEE 2006 Question PaperpavaniNo ratings yet
- Grade 3 Sense Organs, Nose Tongue and SkinDocument3 pagesGrade 3 Sense Organs, Nose Tongue and SkinPhen OrenNo ratings yet
- DR Nalli R GopinathDocument16 pagesDR Nalli R GopinathBabu RamakrishnanNo ratings yet
- Price ALL Z-VentDocument9 pagesPrice ALL Z-VentPanco NanaNo ratings yet
- Burning Mouth SyndromeDocument3 pagesBurning Mouth SyndromeYohana RebeccaNo ratings yet
- Gintex DSDocument1 pageGintex DSRaihanulKabirNo ratings yet
- Epidemiology of Covid-19 in A Long-Term Care Facility in King County, WashingtonDocument9 pagesEpidemiology of Covid-19 in A Long-Term Care Facility in King County, WashingtonZelgi PutraNo ratings yet
- Pharmacology of Silymarin: F. Fraschini, G. Demartini and D. EspostiDocument15 pagesPharmacology of Silymarin: F. Fraschini, G. Demartini and D. EspostiVennyNo ratings yet
- Year Book 2018-19 (21-08-20) - 1Document365 pagesYear Book 2018-19 (21-08-20) - 1Tabib Afzaal Ahmad VirkNo ratings yet
- Important Questions For Esic Staff Nurse Recruitment ExamDocument4 pagesImportant Questions For Esic Staff Nurse Recruitment ExamSuchitaNo ratings yet
- AOGD Bulletin December 2019Document68 pagesAOGD Bulletin December 2019Abhilekh SrivastavaNo ratings yet
- Neck Anatomy: Lymph NodesDocument5 pagesNeck Anatomy: Lymph NodesKiara GovenderNo ratings yet
- First AidDocument72 pagesFirst AidNaushad AliNo ratings yet
- ECG (Rythm Interpretation)Document39 pagesECG (Rythm Interpretation)RatnaSuryati100% (1)
- Menopause KDocument36 pagesMenopause Kkarendelarosa06100% (2)
- COMLEX Level 3 Time Grid and Self AssessmentDocument19 pagesCOMLEX Level 3 Time Grid and Self AssessmentR KidderNo ratings yet
- 06ectropion & EntropionDocument17 pages06ectropion & EntropionShari' Si Wahyu100% (1)
- High-Efficiency and High-Flux Hemodialysis: Sivasankaran Ambalavanan Gary Rabetoy Alfred K. CheungDocument10 pagesHigh-Efficiency and High-Flux Hemodialysis: Sivasankaran Ambalavanan Gary Rabetoy Alfred K. CheungveiaNo ratings yet
- Immunofluorescence Analyzer: Lifotronic FA-160Document2 pagesImmunofluorescence Analyzer: Lifotronic FA-160Bodega PromalabNo ratings yet
- Internet AddictionDocument23 pagesInternet AddictionAdam Bullock100% (1)
- Amandeep Kaur Nursing Demonstrator Ionurc, Goindwal Sahib, PunjabDocument20 pagesAmandeep Kaur Nursing Demonstrator Ionurc, Goindwal Sahib, PunjabSanjay Kumar SanjuNo ratings yet
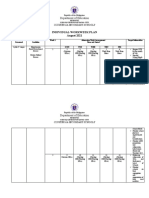
- Department of Education: Individual Workweek Plan August 2021Document5 pagesDepartment of Education: Individual Workweek Plan August 2021Jeffren P. MiguelNo ratings yet
- ResearchDocument3 pagesResearchDr Sreeja KSNo ratings yet
- A Psychobiological Perspective On The Personality Disorders: LarryDocument12 pagesA Psychobiological Perspective On The Personality Disorders: LarryDrobota MirunaNo ratings yet