
Diagnostic Imaging ENT
Diagnostic Imaging ENT
You might also like
- Alveolarbone 191230081117 PDFDocument41 pagesAlveolarbone 191230081117 PDFسارة العبيديNo ratings yet
- Adrenal Function TestDocument26 pagesAdrenal Function TestSaroja Veeresh86% (7)
- Radiology September 2010Document33 pagesRadiology September 2010Pushpanjali Crosslay HospitalNo ratings yet
- Imaging and Diagnosis For Planning The Surgical Procedure: Ferdinand BauerDocument26 pagesImaging and Diagnosis For Planning The Surgical Procedure: Ferdinand BauerIblisuang UangNo ratings yet
- CT Scan in VeterinaryDocument4 pagesCT Scan in VeterinarySurajNo ratings yet
- Article Imaging of Salivary Gland TumoursDocument11 pagesArticle Imaging of Salivary Gland TumourskaryndpNo ratings yet
- Intra-Axial Brain TumorsDocument18 pagesIntra-Axial Brain Tumorsputu risyaNo ratings yet
- 2020 Mielotc PDFDocument15 pages2020 Mielotc PDFR M MNo ratings yet
- Computerised Tomography and Magnetic Resonance Imaging of Laryngeal Squamous Cell Carcinoma: A Practical ApproachDocument8 pagesComputerised Tomography and Magnetic Resonance Imaging of Laryngeal Squamous Cell Carcinoma: A Practical ApproachNengLukmanNo ratings yet
- Anatomy de NeckDocument17 pagesAnatomy de NeckAnonymous yv4iLzsKtgNo ratings yet
- JCB 12 42254Document7 pagesJCB 12 42254yohanasmjtNo ratings yet
- Thoracicneoplasms Inchildren: Beverley NewmanDocument32 pagesThoracicneoplasms Inchildren: Beverley NewmannadiaNo ratings yet
- MRI KydneyDocument14 pagesMRI KydneyManuel Leonardo CaetanoNo ratings yet
- The Different Faces of Central Nervous MetastasisDocument15 pagesThe Different Faces of Central Nervous MetastasisTika wahyuNo ratings yet
- Jurnal Pancoast TumorDocument6 pagesJurnal Pancoast Tumordwi ajiNo ratings yet
- Promotion of Well Being During Treatment For.12Document17 pagesPromotion of Well Being During Treatment For.12Nica SalazarNo ratings yet
- Yuh2009 Article ImagingOfEpendymomasMRIAndCTDocument11 pagesYuh2009 Article ImagingOfEpendymomasMRIAndCTHuyen NguyenNo ratings yet
- IndianJRadiolImaging - Imaging in Laringeal CancerDocument18 pagesIndianJRadiolImaging - Imaging in Laringeal CancerMirela IordacheNo ratings yet
- 4644 16382 1 PBDocument8 pages4644 16382 1 PBWahyu RianiNo ratings yet
- DownloadDocument9 pagesDownloadhasan nazzalNo ratings yet
- Brain and Lung Cancer DetectionDocument15 pagesBrain and Lung Cancer DetectionSachin PathareNo ratings yet
- Healthcare 01 00084Document12 pagesHealthcare 01 00084svrobertNo ratings yet
- Principles of Management of Soft Tissue SarcomaDocument33 pagesPrinciples of Management of Soft Tissue Sarcomabashiruaminu100% (1)
- (2016) Computed Tomography Imaging in Oncology.Document15 pages(2016) Computed Tomography Imaging in Oncology.ludiegues752No ratings yet
- Max Illo Facial SurgeryDocument92 pagesMax Illo Facial Surgerychueychuan100% (1)
- Guidelines Endoscopic Spine SurgeryDocument11 pagesGuidelines Endoscopic Spine SurgerynhieuntnNo ratings yet
- Hallifax Radiological Investigation of Pleural DiseaseDocument38 pagesHallifax Radiological Investigation of Pleural Diseaselaila.forestaNo ratings yet
- Imaging The Temporal Bone: NeuroradiologyDocument15 pagesImaging The Temporal Bone: NeuroradiologyMaulidianaIndahNo ratings yet
- 1808 8694 Bjorl 86 s1 0s23Document3 pages1808 8694 Bjorl 86 s1 0s23VITOR PEREZNo ratings yet
- Breast Mri ThesisDocument9 pagesBreast Mri ThesisKaela Johnson100% (2)
- TC YrmnDocument18 pagesTC Yrmnangelica cuevasNo ratings yet
- PIIS1064968921006942Document20 pagesPIIS1064968921006942Monik AlamandaNo ratings yet
- Intracranial Yolk Sac Tumor in An Adult Patient: MRI, Diffusion-Weighted Imaging and H MR Spectroscopy FeaturesDocument4 pagesIntracranial Yolk Sac Tumor in An Adult Patient: MRI, Diffusion-Weighted Imaging and H MR Spectroscopy FeaturestiaraNo ratings yet
- Intracranial CystsDocument9 pagesIntracranial CystsjosephNo ratings yet
- Managment of Temporomandibular DisordersDocument25 pagesManagment of Temporomandibular DisordersDewi Astuti100% (1)
- Jurnal 1Document10 pagesJurnal 1Putri Dery CahyaniNo ratings yet
- Paranasal Sinus Imaging: Roberto Maroldi, Marco Ravanelli, Andrea Borghesi, Davide FarinaDocument15 pagesParanasal Sinus Imaging: Roberto Maroldi, Marco Ravanelli, Andrea Borghesi, Davide FarinaAlin SuarliakNo ratings yet
- Multiple Cranial Nerve PalsiesDocument11 pagesMultiple Cranial Nerve PalsiesVijay BabuNo ratings yet
- Kelompok 6 Mri For Pituitary GlandDocument23 pagesKelompok 6 Mri For Pituitary GlandAndahZantman AsmirandahNo ratings yet
- A Rare Case of Large Size Undifferentiated Pleomorphic Sarcoma of AnkleDocument5 pagesA Rare Case of Large Size Undifferentiated Pleomorphic Sarcoma of AnkleIJAR JOURNALNo ratings yet
- TMD For Fifth Stage Students 2023Document19 pagesTMD For Fifth Stage Students 2023wxmdkhbyvkNo ratings yet
- Bjro 20200019Document11 pagesBjro 20200019AmandaNo ratings yet
- BJR 71 846 9849380Document8 pagesBJR 71 846 9849380BitaNo ratings yet
- Chin-Optimization and Comparison of Myocardial T1 Techniques at 3T in Patients With Aortic Stenosis - 2014-Eur Heart J Cardiovasc ImagingDocument10 pagesChin-Optimization and Comparison of Myocardial T1 Techniques at 3T in Patients With Aortic Stenosis - 2014-Eur Heart J Cardiovasc Imagingcchin03mNo ratings yet
- Forrest2016 CT Imaging CancerDocument15 pagesForrest2016 CT Imaging CancerLetícia InamassuNo ratings yet
- 2012 Effects of RT in Head and NeckDocument10 pages2012 Effects of RT in Head and NeckCamiDavidNo ratings yet
- CT ScanDocument14 pagesCT ScanShyam Narayanan100% (1)
- Gc55inf 5 Att1 - enDocument10 pagesGc55inf 5 Att1 - enMaria DovinaNo ratings yet
- TAC en TraumaDocument9 pagesTAC en Traumasamuelfdiaz.0103No ratings yet
- Jurnal 1 PDFDocument10 pagesJurnal 1 PDFPutri Dery CahyaniNo ratings yet
- Meningioma in The Lumbar SpineDocument12 pagesMeningioma in The Lumbar Spinemex487No ratings yet
- Lung BiopsyDocument8 pagesLung BiopsySiya PatilNo ratings yet
- Imaging in Brain MeningiomaDocument12 pagesImaging in Brain MeningiomaBramanda Sml TobingNo ratings yet
- Lee 2009Document9 pagesLee 2009PGY 6No ratings yet
- Theme: Evaluation of The Technique of Performing Angio-Scanning at Chme LuxembourgDocument9 pagesTheme: Evaluation of The Technique of Performing Angio-Scanning at Chme LuxembourgIJAR JOURNALNo ratings yet
- Chapter 3 1-Response Evaluation and Follow-Up by IDocument32 pagesChapter 3 1-Response Evaluation and Follow-Up by IZe PushNo ratings yet
- Clinical Application CTDocument40 pagesClinical Application CTWalaa MajeedNo ratings yet
- Altmayer 2019Document50 pagesAltmayer 2019Radiologi RSPDNo ratings yet
- CT in Staging of Lung Cancer 2002 Eur Resp JDocument9 pagesCT in Staging of Lung Cancer 2002 Eur Resp JPradeepNo ratings yet
- Clinical MRIDocument30 pagesClinical MRImarcu.dragos94No ratings yet
- Head InjuryDocument39 pagesHead InjuryDr. Jayesh Patidar100% (1)
- DTL Implants-ABDocument2 pagesDTL Implants-ABananthNo ratings yet
- 7structural Organization in Animals PDFDocument8 pages7structural Organization in Animals PDFDharmendra SinghNo ratings yet
- Lect.8 HyperaldosteronismDocument10 pagesLect.8 HyperaldosteronismShubhamNo ratings yet
- Craniofacial Changes in Patients With Class III Malocclusion Treated With The Rampa SystemDocument7 pagesCraniofacial Changes in Patients With Class III Malocclusion Treated With The Rampa Systemapi-192260741100% (1)
- NCM 107 (OB) Module 1BDocument48 pagesNCM 107 (OB) Module 1BAmiel simon NgoNo ratings yet
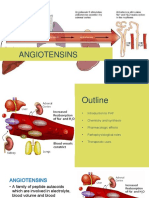
- 3.9. Angiotensins''Document44 pages3.9. Angiotensins''Garry LasagaNo ratings yet
- The Endocrine System Who Is in Control HereDocument43 pagesThe Endocrine System Who Is in Control HereJoe Marie A Mendoza0% (1)
- Maternal Lec Week 1 3Document4 pagesMaternal Lec Week 1 3Althea ManarpiisNo ratings yet
- ASTRO Contouring-Table - 1supplementDocument5 pagesASTRO Contouring-Table - 1supplementEskadmas BelayNo ratings yet
- How Impacted Wisdom Teeth Affect Your Oral HealthDocument2 pagesHow Impacted Wisdom Teeth Affect Your Oral HealthWisdom Teeth RemovalNo ratings yet
- Chicken AnatomyDocument24 pagesChicken Anatomybrianmore10No ratings yet
- Circulatory System AssignmentDocument23 pagesCirculatory System Assignmentapi-239884728100% (1)
- Mantak Chia CNT Book - Open Wind GateDocument1 pageMantak Chia CNT Book - Open Wind GateUniversal Healing Tao100% (6)
- Anatomy Question BankDocument13 pagesAnatomy Question BankMahnaz MushtaqNo ratings yet
- Respiratory SystemDocument20 pagesRespiratory Systemapi-235944649No ratings yet
- Sas 3 AnaphyDocument7 pagesSas 3 AnaphyClarrinne Geralence Galo RomoNo ratings yet
- Hormones and The Endocrine System: BiologyDocument78 pagesHormones and The Endocrine System: Biologytricia tghNo ratings yet
- The Excretory SystemDocument3 pagesThe Excretory SystemMelvel John Nobleza AmarilloNo ratings yet
- Digestive System Label MeDocument13 pagesDigestive System Label MeMuhammad AdibNo ratings yet
- LarynxDocument21 pagesLarynxnano1987N100% (1)
- 46 MusclesDocument5 pages46 Musclesuddim004100% (2)
- The Digestive System: Chapter 2, Section 2.2Document10 pagesThe Digestive System: Chapter 2, Section 2.2Noralyn Ngislawan-GunnawaNo ratings yet
- Puberty and Its Disorders Puberty and Its DisordersDocument57 pagesPuberty and Its Disorders Puberty and Its DisordersYeltserNo ratings yet
- Blood CellsDocument10 pagesBlood CellsTItan NainiNo ratings yet
- Hassel 1995Document9 pagesHassel 1995Emilio MurciaNo ratings yet
- Organ TransplantationDocument36 pagesOrgan TransplantationAnonymous 4TUSi0SqNo ratings yet
- Bahasa Inggris 1.13Document5 pagesBahasa Inggris 1.13Rizky AdiNo ratings yet
























































































Download as doc, pdf, or txt
You might also like
- Alveolarbone 191230081117 PDFDocument41 pagesAlveolarbone 191230081117 PDFسارة العبيديNo ratings yet
- Adrenal Function TestDocument26 pagesAdrenal Function TestSaroja Veeresh86% (7)
- Radiology September 2010Document33 pagesRadiology September 2010Pushpanjali Crosslay HospitalNo ratings yet
- Imaging and Diagnosis For Planning The Surgical Procedure: Ferdinand BauerDocument26 pagesImaging and Diagnosis For Planning The Surgical Procedure: Ferdinand BauerIblisuang UangNo ratings yet
- CT Scan in VeterinaryDocument4 pagesCT Scan in VeterinarySurajNo ratings yet
- Article Imaging of Salivary Gland TumoursDocument11 pagesArticle Imaging of Salivary Gland TumourskaryndpNo ratings yet
- Intra-Axial Brain TumorsDocument18 pagesIntra-Axial Brain Tumorsputu risyaNo ratings yet
- 2020 Mielotc PDFDocument15 pages2020 Mielotc PDFR M MNo ratings yet
- Computerised Tomography and Magnetic Resonance Imaging of Laryngeal Squamous Cell Carcinoma: A Practical ApproachDocument8 pagesComputerised Tomography and Magnetic Resonance Imaging of Laryngeal Squamous Cell Carcinoma: A Practical ApproachNengLukmanNo ratings yet
- Anatomy de NeckDocument17 pagesAnatomy de NeckAnonymous yv4iLzsKtgNo ratings yet
- JCB 12 42254Document7 pagesJCB 12 42254yohanasmjtNo ratings yet
- Thoracicneoplasms Inchildren: Beverley NewmanDocument32 pagesThoracicneoplasms Inchildren: Beverley NewmannadiaNo ratings yet
- MRI KydneyDocument14 pagesMRI KydneyManuel Leonardo CaetanoNo ratings yet
- The Different Faces of Central Nervous MetastasisDocument15 pagesThe Different Faces of Central Nervous MetastasisTika wahyuNo ratings yet
- Jurnal Pancoast TumorDocument6 pagesJurnal Pancoast Tumordwi ajiNo ratings yet
- Promotion of Well Being During Treatment For.12Document17 pagesPromotion of Well Being During Treatment For.12Nica SalazarNo ratings yet
- Yuh2009 Article ImagingOfEpendymomasMRIAndCTDocument11 pagesYuh2009 Article ImagingOfEpendymomasMRIAndCTHuyen NguyenNo ratings yet
- IndianJRadiolImaging - Imaging in Laringeal CancerDocument18 pagesIndianJRadiolImaging - Imaging in Laringeal CancerMirela IordacheNo ratings yet
- 4644 16382 1 PBDocument8 pages4644 16382 1 PBWahyu RianiNo ratings yet
- DownloadDocument9 pagesDownloadhasan nazzalNo ratings yet
- Brain and Lung Cancer DetectionDocument15 pagesBrain and Lung Cancer DetectionSachin PathareNo ratings yet
- Healthcare 01 00084Document12 pagesHealthcare 01 00084svrobertNo ratings yet
- Principles of Management of Soft Tissue SarcomaDocument33 pagesPrinciples of Management of Soft Tissue Sarcomabashiruaminu100% (1)
- (2016) Computed Tomography Imaging in Oncology.Document15 pages(2016) Computed Tomography Imaging in Oncology.ludiegues752No ratings yet
- Max Illo Facial SurgeryDocument92 pagesMax Illo Facial Surgerychueychuan100% (1)
- Guidelines Endoscopic Spine SurgeryDocument11 pagesGuidelines Endoscopic Spine SurgerynhieuntnNo ratings yet
- Hallifax Radiological Investigation of Pleural DiseaseDocument38 pagesHallifax Radiological Investigation of Pleural Diseaselaila.forestaNo ratings yet
- Imaging The Temporal Bone: NeuroradiologyDocument15 pagesImaging The Temporal Bone: NeuroradiologyMaulidianaIndahNo ratings yet
- 1808 8694 Bjorl 86 s1 0s23Document3 pages1808 8694 Bjorl 86 s1 0s23VITOR PEREZNo ratings yet
- Breast Mri ThesisDocument9 pagesBreast Mri ThesisKaela Johnson100% (2)
- TC YrmnDocument18 pagesTC Yrmnangelica cuevasNo ratings yet
- PIIS1064968921006942Document20 pagesPIIS1064968921006942Monik AlamandaNo ratings yet
- Intracranial Yolk Sac Tumor in An Adult Patient: MRI, Diffusion-Weighted Imaging and H MR Spectroscopy FeaturesDocument4 pagesIntracranial Yolk Sac Tumor in An Adult Patient: MRI, Diffusion-Weighted Imaging and H MR Spectroscopy FeaturestiaraNo ratings yet
- Intracranial CystsDocument9 pagesIntracranial CystsjosephNo ratings yet
- Managment of Temporomandibular DisordersDocument25 pagesManagment of Temporomandibular DisordersDewi Astuti100% (1)
- Jurnal 1Document10 pagesJurnal 1Putri Dery CahyaniNo ratings yet
- Paranasal Sinus Imaging: Roberto Maroldi, Marco Ravanelli, Andrea Borghesi, Davide FarinaDocument15 pagesParanasal Sinus Imaging: Roberto Maroldi, Marco Ravanelli, Andrea Borghesi, Davide FarinaAlin SuarliakNo ratings yet
- Multiple Cranial Nerve PalsiesDocument11 pagesMultiple Cranial Nerve PalsiesVijay BabuNo ratings yet
- Kelompok 6 Mri For Pituitary GlandDocument23 pagesKelompok 6 Mri For Pituitary GlandAndahZantman AsmirandahNo ratings yet
- A Rare Case of Large Size Undifferentiated Pleomorphic Sarcoma of AnkleDocument5 pagesA Rare Case of Large Size Undifferentiated Pleomorphic Sarcoma of AnkleIJAR JOURNALNo ratings yet
- TMD For Fifth Stage Students 2023Document19 pagesTMD For Fifth Stage Students 2023wxmdkhbyvkNo ratings yet
- Bjro 20200019Document11 pagesBjro 20200019AmandaNo ratings yet
- BJR 71 846 9849380Document8 pagesBJR 71 846 9849380BitaNo ratings yet
- Chin-Optimization and Comparison of Myocardial T1 Techniques at 3T in Patients With Aortic Stenosis - 2014-Eur Heart J Cardiovasc ImagingDocument10 pagesChin-Optimization and Comparison of Myocardial T1 Techniques at 3T in Patients With Aortic Stenosis - 2014-Eur Heart J Cardiovasc Imagingcchin03mNo ratings yet
- Forrest2016 CT Imaging CancerDocument15 pagesForrest2016 CT Imaging CancerLetícia InamassuNo ratings yet
- 2012 Effects of RT in Head and NeckDocument10 pages2012 Effects of RT in Head and NeckCamiDavidNo ratings yet
- CT ScanDocument14 pagesCT ScanShyam Narayanan100% (1)
- Gc55inf 5 Att1 - enDocument10 pagesGc55inf 5 Att1 - enMaria DovinaNo ratings yet
- TAC en TraumaDocument9 pagesTAC en Traumasamuelfdiaz.0103No ratings yet
- Jurnal 1 PDFDocument10 pagesJurnal 1 PDFPutri Dery CahyaniNo ratings yet
- Meningioma in The Lumbar SpineDocument12 pagesMeningioma in The Lumbar Spinemex487No ratings yet
- Lung BiopsyDocument8 pagesLung BiopsySiya PatilNo ratings yet
- Imaging in Brain MeningiomaDocument12 pagesImaging in Brain MeningiomaBramanda Sml TobingNo ratings yet
- Lee 2009Document9 pagesLee 2009PGY 6No ratings yet
- Theme: Evaluation of The Technique of Performing Angio-Scanning at Chme LuxembourgDocument9 pagesTheme: Evaluation of The Technique of Performing Angio-Scanning at Chme LuxembourgIJAR JOURNALNo ratings yet
- Chapter 3 1-Response Evaluation and Follow-Up by IDocument32 pagesChapter 3 1-Response Evaluation and Follow-Up by IZe PushNo ratings yet
- Clinical Application CTDocument40 pagesClinical Application CTWalaa MajeedNo ratings yet
- Altmayer 2019Document50 pagesAltmayer 2019Radiologi RSPDNo ratings yet
- CT in Staging of Lung Cancer 2002 Eur Resp JDocument9 pagesCT in Staging of Lung Cancer 2002 Eur Resp JPradeepNo ratings yet
- Clinical MRIDocument30 pagesClinical MRImarcu.dragos94No ratings yet
- Head InjuryDocument39 pagesHead InjuryDr. Jayesh Patidar100% (1)
- DTL Implants-ABDocument2 pagesDTL Implants-ABananthNo ratings yet
- 7structural Organization in Animals PDFDocument8 pages7structural Organization in Animals PDFDharmendra SinghNo ratings yet
- Lect.8 HyperaldosteronismDocument10 pagesLect.8 HyperaldosteronismShubhamNo ratings yet
- Craniofacial Changes in Patients With Class III Malocclusion Treated With The Rampa SystemDocument7 pagesCraniofacial Changes in Patients With Class III Malocclusion Treated With The Rampa Systemapi-192260741100% (1)
- NCM 107 (OB) Module 1BDocument48 pagesNCM 107 (OB) Module 1BAmiel simon NgoNo ratings yet
- 3.9. Angiotensins''Document44 pages3.9. Angiotensins''Garry LasagaNo ratings yet
- The Endocrine System Who Is in Control HereDocument43 pagesThe Endocrine System Who Is in Control HereJoe Marie A Mendoza0% (1)
- Maternal Lec Week 1 3Document4 pagesMaternal Lec Week 1 3Althea ManarpiisNo ratings yet
- ASTRO Contouring-Table - 1supplementDocument5 pagesASTRO Contouring-Table - 1supplementEskadmas BelayNo ratings yet
- How Impacted Wisdom Teeth Affect Your Oral HealthDocument2 pagesHow Impacted Wisdom Teeth Affect Your Oral HealthWisdom Teeth RemovalNo ratings yet
- Chicken AnatomyDocument24 pagesChicken Anatomybrianmore10No ratings yet
- Circulatory System AssignmentDocument23 pagesCirculatory System Assignmentapi-239884728100% (1)
- Mantak Chia CNT Book - Open Wind GateDocument1 pageMantak Chia CNT Book - Open Wind GateUniversal Healing Tao100% (6)
- Anatomy Question BankDocument13 pagesAnatomy Question BankMahnaz MushtaqNo ratings yet
- Respiratory SystemDocument20 pagesRespiratory Systemapi-235944649No ratings yet
- Sas 3 AnaphyDocument7 pagesSas 3 AnaphyClarrinne Geralence Galo RomoNo ratings yet
- Hormones and The Endocrine System: BiologyDocument78 pagesHormones and The Endocrine System: Biologytricia tghNo ratings yet
- The Excretory SystemDocument3 pagesThe Excretory SystemMelvel John Nobleza AmarilloNo ratings yet
- Digestive System Label MeDocument13 pagesDigestive System Label MeMuhammad AdibNo ratings yet
- LarynxDocument21 pagesLarynxnano1987N100% (1)
- 46 MusclesDocument5 pages46 Musclesuddim004100% (2)
- The Digestive System: Chapter 2, Section 2.2Document10 pagesThe Digestive System: Chapter 2, Section 2.2Noralyn Ngislawan-GunnawaNo ratings yet
- Puberty and Its Disorders Puberty and Its DisordersDocument57 pagesPuberty and Its Disorders Puberty and Its DisordersYeltserNo ratings yet
- Blood CellsDocument10 pagesBlood CellsTItan NainiNo ratings yet
- Hassel 1995Document9 pagesHassel 1995Emilio MurciaNo ratings yet
- Organ TransplantationDocument36 pagesOrgan TransplantationAnonymous 4TUSi0SqNo ratings yet
- Bahasa Inggris 1.13Document5 pagesBahasa Inggris 1.13Rizky AdiNo ratings yet