Download as doc, pdf, or txt
You might also like
- Format For Field Technical Report (2017) For Certified Professional in Sewage Treatment Plant OperationsDocument25 pagesFormat For Field Technical Report (2017) For Certified Professional in Sewage Treatment Plant OperationsyogapostNo ratings yet
- Made to Serve: How Manufacturers can Compete Through Servitization and Product Service SystemsFrom EverandMade to Serve: How Manufacturers can Compete Through Servitization and Product Service SystemsNo ratings yet
- As 1755-2000 Conveyors - Safety RequirementsDocument8 pagesAs 1755-2000 Conveyors - Safety RequirementsSAI Global - APACNo ratings yet
- Fraud Survey by TM ForumDocument44 pagesFraud Survey by TM ForumPreetam Edwin LakraNo ratings yet
- Professional Review Industry Route Application FormDocument14 pagesProfessional Review Industry Route Application FormshajbabyNo ratings yet
- Reading Starbucks Case StudyDocument35 pagesReading Starbucks Case StudyArun Prashanth BNo ratings yet
- MFPADocument6 pagesMFPAJohnny TehNo ratings yet
- Application For Industrial / Institutional MembershipDocument2 pagesApplication For Industrial / Institutional MembershipHeet PatelNo ratings yet
- Companies and Business Booklet 2021Document65 pagesCompanies and Business Booklet 2021Benjamin BandaNo ratings yet
- RFP - Giveaways For DPCSH 2023 V2 - Clean Version (002) FinalDocument40 pagesRFP - Giveaways For DPCSH 2023 V2 - Clean Version (002) FinalUmair AzizNo ratings yet
- Expressions of Interest EOI Goods and ServicesDocument16 pagesExpressions of Interest EOI Goods and ServicesomarNo ratings yet
- PHD Part Time NoC Letter FormatDocument1 pagePHD Part Time NoC Letter Formatapparao kunchala100% (1)
- 23012019112133request For ProposalDocument74 pages23012019112133request For ProposalpallavNo ratings yet
- Response and Work Breakdown Form Enter Respondent Name Here: IT Service Management Solution (ITSM) ImplementationDocument70 pagesResponse and Work Breakdown Form Enter Respondent Name Here: IT Service Management Solution (ITSM) ImplementationBikash Ranjan SatapathyNo ratings yet
- Vrlabsimulation SRD FinalDocument14 pagesVrlabsimulation SRD Finalapi-548719926No ratings yet
- Langat BenardDocument37 pagesLangat Benardjackey akodhe0% (1)
- BGC FormDocument2 pagesBGC FormKunika BhalotraNo ratings yet
- Corporate Manual V1Document9 pagesCorporate Manual V1manishNo ratings yet
- Expression of InterestDocument98 pagesExpression of InterestOracle1991No ratings yet
- Joseph Burn A Cles Belle NarrativeDocument26 pagesJoseph Burn A Cles Belle NarrativeGrace Anne TubosaNo ratings yet
- E Tender BGREISep 2019Document44 pagesE Tender BGREISep 2019Enamul HaqueNo ratings yet
- Tamil Nadu Skill Development CorporationDocument29 pagesTamil Nadu Skill Development CorporationSEED GLOBALNo ratings yet
- Pre-Qualified Suppliers Invitation LetterDocument8 pagesPre-Qualified Suppliers Invitation Lettermorgan mainaNo ratings yet
- Gems Sap SRM Ros Userguide 1 2Document48 pagesGems Sap SRM Ros Userguide 1 2Lam Chun YienNo ratings yet
- Licensing For EstablishmentDocument31 pagesLicensing For EstablishmentTZ LABNo ratings yet
- Multitech Business SchoolDocument32 pagesMultitech Business SchoolMUBANGIZI FELEXNo ratings yet
- COSO Registration Form Eng.Document2 pagesCOSO Registration Form Eng.mosoliman86No ratings yet
- PQDs For 2k MasajidDocument29 pagesPQDs For 2k MasajidAdnan KhanNo ratings yet
- Application For Initial Approval, Change To Approval or Remote Site Approval Under EC Regulation 2042/2003 Annex IV Part-147Document7 pagesApplication For Initial Approval, Change To Approval or Remote Site Approval Under EC Regulation 2042/2003 Annex IV Part-147David OwenNo ratings yet
- Form IDocument1 pageForm Izahidtanveer1990No ratings yet
- Gem LuckmowDocument66 pagesGem LuckmowTushaar PahujaNo ratings yet
- Business Registration Form: (Submitted With BMC)Document7 pagesBusiness Registration Form: (Submitted With BMC)NASIEYRA AMYLIANA BINTI MOHD NASIR / UPMNo ratings yet
- Allegato-4 Companyagreementform STUDENTIDocument7 pagesAllegato-4 Companyagreementform STUDENTIJacopo SoraniNo ratings yet
- SF424 RR Guide General Ver2Document194 pagesSF424 RR Guide General Ver2Kathleen DearingerNo ratings yet
- Application For Reg of A Prvte Med Inst 2021Document12 pagesApplication For Reg of A Prvte Med Inst 2021jlinkcyber20No ratings yet
- Constructors-Operators FormDocument13 pagesConstructors-Operators Formzain jawadNo ratings yet
- Application FormDocument3 pagesApplication FormManish PaliwalNo ratings yet
- Form-COS-5Document1 pageForm-COS-5asmybablooNo ratings yet
- IG1179 5G Revenue Management Impact Assessment v2.0.1Document90 pagesIG1179 5G Revenue Management Impact Assessment v2.0.1Komal PatelNo ratings yet
- EsdmDocument3 pagesEsdmShan HuayNo ratings yet
- Ce PPOMEDocument62 pagesCe PPOMEkhaidirman otah gimaNo ratings yet
- Motor Vehicles Spare PartsDocument38 pagesMotor Vehicles Spare PartsKevin AtutiNo ratings yet
- RFP Vol 2 NGO Darpan 2.0 UnlockedDocument182 pagesRFP Vol 2 NGO Darpan 2.0 UnlockedShashank AryaNo ratings yet
- Cepswam FTR Format 2018Document31 pagesCepswam FTR Format 2018ricky50% (10)
- DICKSONDocument33 pagesDICKSONkipchumbabrian702No ratings yet
- IT ITES Scheme Brochure 051020Document39 pagesIT ITES Scheme Brochure 051020monu160No ratings yet
- GB967 Policy in Charging and Billing V6 2Document62 pagesGB967 Policy in Charging and Billing V6 2El KabliNo ratings yet
- RFP For MobileSeva For TP Ver 1.2Document62 pagesRFP For MobileSeva For TP Ver 1.2Akram M. AlmotaaNo ratings yet
- Cal FadDocument79 pagesCal FadLeonardo Vence OrdoñezNo ratings yet
- List of Documents ProjectDocument2 pagesList of Documents ProjectSanjay ChowdhuryNo ratings yet
- Eo IdocumentDocument24 pagesEo IdocumentSEED GLOBALNo ratings yet
- Mfu SopDocument66 pagesMfu SopSuman KumarNo ratings yet
- Industrial Attachment Contract: The Industrial Training Act Cap 237 Laws of KenyaDocument4 pagesIndustrial Attachment Contract: The Industrial Training Act Cap 237 Laws of KenyaRouxcel abutoNo ratings yet
- Membership EIZ Applications Form 10Document4 pagesMembership EIZ Applications Form 10engkj75% (4)
- 5032100727..Nyongesa w Cosmas-3Document29 pages5032100727..Nyongesa w Cosmas-3Michael MunokoNo ratings yet
- Laporan PKL Gabung Vinka 2Document62 pagesLaporan PKL Gabung Vinka 2Jen Yu RaNo ratings yet
- SS ISO 9712-2022 PreviewDocument12 pagesSS ISO 9712-2022 Previewandrewhw100% (1)
- RFP For IRDAI SAP ERP AMC and FIORI Implementation ServicesDocument76 pagesRFP For IRDAI SAP ERP AMC and FIORI Implementation Serviceskamel ghiarNo ratings yet
- UEMS MJC SM Application For Certification by EquivalenceDocument4 pagesUEMS MJC SM Application For Certification by EquivalenceNico IonaşcuNo ratings yet
- Tendernotice 1Document78 pagesTendernotice 1JaiParkashNo ratings yet
- Just ›A Machine for Doing Business‹?: Sociomaterial Configurations of the Intranet in a Post-merger Telecommunications CompanyFrom EverandJust ›A Machine for Doing Business‹?: Sociomaterial Configurations of the Intranet in a Post-merger Telecommunications CompanyNo ratings yet
- The Addiction Counselor's Documentation Sourcebook: The Complete Paperwork Resource for Treating Clients with AddictionsFrom EverandThe Addiction Counselor's Documentation Sourcebook: The Complete Paperwork Resource for Treating Clients with AddictionsNo ratings yet
- Bec P Reading and WritingDocument15 pagesBec P Reading and WritingMonica IorgulescuNo ratings yet
- Working Jocil 06Document83 pagesWorking Jocil 06Phani Deepika Koritala0% (1)
- Risk Assumption Letter: Mi Service Centre Co Simran EnterprisesDocument4 pagesRisk Assumption Letter: Mi Service Centre Co Simran EnterprisesHitendra chauhanNo ratings yet
- Mismtmsummarywithopenformat3Mktratesummary 29100 29101 29102 29103 29104 29105 29106 29107 29108 29109 29110Document29 pagesMismtmsummarywithopenformat3Mktratesummary 29100 29101 29102 29103 29104 29105 29106 29107 29108 29109 29110kd316No ratings yet
- BR081410 An Intellectual Amit BhaduriDocument2 pagesBR081410 An Intellectual Amit BhaduriSwastee RanjanNo ratings yet
- Warwick Business School MBA Brochure 2017 18Document17 pagesWarwick Business School MBA Brochure 2017 18glenlcyNo ratings yet
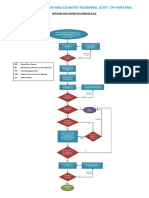
- Epartment of Town and Country Planning, Govt. of Haryana: Applying For Change of Landuse (Clu)Document2 pagesEpartment of Town and Country Planning, Govt. of Haryana: Applying For Change of Landuse (Clu)AnilNo ratings yet
- Redler Conveyor Company v. Commissioner of Internal Revenue, 303 F.2d 567, 1st Cir. (1962)Document4 pagesRedler Conveyor Company v. Commissioner of Internal Revenue, 303 F.2d 567, 1st Cir. (1962)Scribd Government DocsNo ratings yet
- Microtek Microtek Line Interactive UPS Legend 650 Ups Legend 650 UpsDocument1 pageMicrotek Microtek Line Interactive UPS Legend 650 Ups Legend 650 UpsAri0% (1)
- A Study On Female Shopping Behavior With Reference To Durable Goods - A Critical AnalysisDocument9 pagesA Study On Female Shopping Behavior With Reference To Durable Goods - A Critical AnalysisCHEIF EDITORNo ratings yet
- Income Elasticity and Cross Price ElasticityDocument6 pagesIncome Elasticity and Cross Price Elasticity5h4d0w4554551nNo ratings yet
- HR and Payroll ManagementDocument8 pagesHR and Payroll ManagementAmit Anand100% (1)
- Pobre Vs Defensor SantiagoDocument9 pagesPobre Vs Defensor SantiagoJohn Robert BautistaNo ratings yet
- Feasibility Study Plan: LabadabangoDocument38 pagesFeasibility Study Plan: LabadabangoCocoy Llamas HernandezNo ratings yet
- Marketing Final ReportDocument70 pagesMarketing Final Reportsatya0% (1)
- Unit 3 Job Application Letters: ContentDocument17 pagesUnit 3 Job Application Letters: ContentanaNo ratings yet
- Increase of Author Is Ed Share Capital ProcedureDocument3 pagesIncrease of Author Is Ed Share Capital ProcedureSai Charan GvNo ratings yet
- Mind GamesDocument9 pagesMind Gamesjbnewbie60% (5)
- Tata Company Entering Into China Market: Module Title: Module Code: Module Leader's NameDocument31 pagesTata Company Entering Into China Market: Module Title: Module Code: Module Leader's NameSouradeep SadhukhanNo ratings yet
- (3.) Interphil Laboratories Employees Union (Digest)Document2 pages(3.) Interphil Laboratories Employees Union (Digest)Dom Robinson BaggayanNo ratings yet
- CH10, Accounting Assignment Answer SheetDocument26 pagesCH10, Accounting Assignment Answer SheetTsenguun Bat-ochirNo ratings yet
- KEY-Sample Test M3 - K46Document3 pagesKEY-Sample Test M3 - K46Tuyền NguyễnNo ratings yet
- Professor P Rameshan: Trade: Challenges & Strategies. New Delhi: Excel BooksDocument5 pagesProfessor P Rameshan: Trade: Challenges & Strategies. New Delhi: Excel BooksRuchi PundhirNo ratings yet
- Fashion StylingDocument1 pageFashion Stylingtarancharan123No ratings yet
- BUSI1633 L5 - Value ChainDocument23 pagesBUSI1633 L5 - Value ChainBùi Thu Hươngg100% (1)
- 1st Sem Result of BBA (B&I) Exam Held in Feb 2023Document33 pages1st Sem Result of BBA (B&I) Exam Held in Feb 2023HardikNo ratings yet
- EX PARTE APPLICATION FEDERAL COURT NATIONSTAR MORTGAGE LLC (Billy Earley)Document25 pagesEX PARTE APPLICATION FEDERAL COURT NATIONSTAR MORTGAGE LLC (Billy Earley)Billy EarleyNo ratings yet
- Coco Tan REO BioDocument3 pagesCoco Tan REO Bioreales8No ratings yet