Download as rtf, pdf, or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5820)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
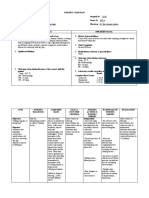
- Nursing Management & LeadershipDocument8 pagesNursing Management & LeadershipDjhoanna Kriska88% (42)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Department of Health Regional Office Ix: Statistical AccomplishmentDocument1 pageDepartment of Health Regional Office Ix: Statistical AccomplishmentNikko Pananganan DajaoNo ratings yet
- Nursing Care PlanDocument6 pagesNursing Care PlanNikko Pananganan DajaoNo ratings yet
- Chapter 36: PicornaviridaeDocument5 pagesChapter 36: PicornaviridaeNikko Pananganan DajaoNo ratings yet
- MNCH Case Study ReviewDocument2 pagesMNCH Case Study ReviewNikko Pananganan DajaoNo ratings yet
- Cap FlowchartDocument2 pagesCap FlowchartNikko Pananganan DajaoNo ratings yet
- ISO 2016 Document LabelsDocument1 pageISO 2016 Document LabelsNikko Pananganan DajaoNo ratings yet
- Biology Reviewer Cell Theory MicrosDocument28 pagesBiology Reviewer Cell Theory MicrosNikko Pananganan DajaoNo ratings yet
- (Citrus Aurantium) Orange Peels and (Citrus) Lemon Extract As A Cure To Open Wound DiseaseDocument8 pages(Citrus Aurantium) Orange Peels and (Citrus) Lemon Extract As A Cure To Open Wound DiseaseNikko Pananganan DajaoNo ratings yet
- Early Detection of Hiv-Aids Cases in Community Through Mobile VCT at High Risk PopulationDocument2 pagesEarly Detection of Hiv-Aids Cases in Community Through Mobile VCT at High Risk PopulationNikko Pananganan DajaoNo ratings yet
- College of Medicine: University of The Philippines ManilaDocument6 pagesCollege of Medicine: University of The Philippines ManilaNikko Pananganan DajaoNo ratings yet
- Theoretical-Conceptual FrameworkDocument2 pagesTheoretical-Conceptual FrameworkNikko Pananganan DajaoNo ratings yet
- Green FashionDocument1 pageGreen FashionNikko Pananganan DajaoNo ratings yet
- CTE Pours Free ThrowsDocument1 pageCTE Pours Free ThrowsNikko Pananganan DajaoNo ratings yet
- Philippine LitDocument71 pagesPhilippine LitNikko Pananganan DajaoNo ratings yet
- Game.: Final Standing (Men) : Final Standing (Women)Document1 pageGame.: Final Standing (Men) : Final Standing (Women)Nikko Pananganan DajaoNo ratings yet
- Predisposing Factors: Precipitating Factors:: Gender - Male Weather Age Young AdultsDocument2 pagesPredisposing Factors: Precipitating Factors:: Gender - Male Weather Age Young AdultsNikko Pananganan DajaoNo ratings yet
- Flare Ups in EndodonticsDocument12 pagesFlare Ups in EndodonticsAnamika Thakur RanaNo ratings yet
- Nursing Care Plan For "AIDS"Document31 pagesNursing Care Plan For "AIDS"jhonroks88% (8)
- Malnutrition-Related Diabetes Mellitus in Africa: PrevalenceDocument7 pagesMalnutrition-Related Diabetes Mellitus in Africa: PrevalenceAbdi KebedeNo ratings yet
- Cape Biology 2020 U2 p1Document17 pagesCape Biology 2020 U2 p1Andrea JaikaranNo ratings yet
- Superspecialty Procedures Under DR YSR Aarogyasri - PC - 13.08.2019 - 001finalDocument18 pagesSuperspecialty Procedures Under DR YSR Aarogyasri - PC - 13.08.2019 - 001finalLokesh KuppiliNo ratings yet
- UNAIDS Core Epidemiology Slides enDocument11 pagesUNAIDS Core Epidemiology Slides enTabarcea VitaliNo ratings yet
- Introduction To Maternity NursingDocument19 pagesIntroduction To Maternity Nursingalmaasfeh2002No ratings yet
- HL6 Crouzon SyndromeDocument4 pagesHL6 Crouzon SyndromeRizkaNNatsirNo ratings yet
- High Flow Nasal Oxygen PDFDocument26 pagesHigh Flow Nasal Oxygen PDFGulshan kumarNo ratings yet
- Stress and HormonesDocument5 pagesStress and HormonesDiana Espinoza SegoviaNo ratings yet
- Retinal Detachment UncenDocument38 pagesRetinal Detachment UncenNixal KurniawanNo ratings yet
- e97c7a82-8e5f-4cb6-bae0-6f90e5f1c198Document18 pagese97c7a82-8e5f-4cb6-bae0-6f90e5f1c198alex torresNo ratings yet
- Annex A - Licensing Standards For Primary Care FacilitiesDocument4 pagesAnnex A - Licensing Standards For Primary Care FacilitiesJoel LenamingNo ratings yet
- Deep Vein ThrombosisDocument103 pagesDeep Vein ThrombosisWildcane SalmeronNo ratings yet
- Metronidazole Drug StudyDocument2 pagesMetronidazole Drug StudyA.No ratings yet
- HaemodialysisDocument3 pagesHaemodialysisVasanth VasanthNo ratings yet
- A Systematic and Universal Artificial Intelligence Screening Method For Oropharyngeal Dysphagia - Improving Diagnosis Through Risk ManagementDocument14 pagesA Systematic and Universal Artificial Intelligence Screening Method For Oropharyngeal Dysphagia - Improving Diagnosis Through Risk ManagementAlvina RusliNo ratings yet
- Chiropractic PDFDocument20 pagesChiropractic PDFAlexandru Cristian StanciuNo ratings yet
- Superficcial MycosisDocument6 pagesSuperficcial MycosisIM CTNo ratings yet
- Pathology ChartsDocument21 pagesPathology Chartspadma maliniNo ratings yet
- High Altitude Phisiology: Adiartha GriadhiDocument43 pagesHigh Altitude Phisiology: Adiartha GriadhilindaNo ratings yet
- Long-Term Survey of Tooth Loss in 600 PtsDocument15 pagesLong-Term Survey of Tooth Loss in 600 PtsAndy HeNo ratings yet
- Set 1 1. Please Tell Us A Little About You.: Blood Donation SurveyDocument2 pagesSet 1 1. Please Tell Us A Little About You.: Blood Donation SurveyHisyam AhmadNo ratings yet
- EndoDocument1 pageEndoMohammed TarekNo ratings yet
- 03 清热剂clearing away heatDocument107 pages03 清热剂clearing away heatKang TianNo ratings yet
- Zapper Candida StudyDocument6 pagesZapper Candida StudymaxguevaraxNo ratings yet
- Lidocaina y CovidDocument5 pagesLidocaina y CovidrichabertNo ratings yet
- Acupuntura TungDocument381 pagesAcupuntura Tung57254343100% (3)
- Cord ProlapseDocument15 pagesCord Prolapsexxdrivexx67% (3)
- 01-12-2020 HMB EnglishDocument10 pages01-12-2020 HMB EnglishKiran SNNo ratings yet