Download as pdf or txt
You might also like
- Donald A. Neumann-Kinesiology of The Musculoskeletal System PDFDocument607 pagesDonald A. Neumann-Kinesiology of The Musculoskeletal System PDFSekar Ciptaningrum97% (97)
- A - Level Project Work Insights & ReflectionsDocument3 pagesA - Level Project Work Insights & ReflectionsKou Uraki0% (1)
- Squeezed by Alissa Quart "Why Our Families Can't Afford America"Document6 pagesSqueezed by Alissa Quart "Why Our Families Can't Afford America"Zahra AfikahNo ratings yet
- Proposal Majlis Berbuka PuasaDocument4 pagesProposal Majlis Berbuka PuasaheryizwanNo ratings yet
- MSE of Uncooperative PTDocument16 pagesMSE of Uncooperative PTGurvinder KalraNo ratings yet
- Nebosh Igc 2Document27 pagesNebosh Igc 2narendra16118890% (40)
- Project Report On RTS Juice PlantDocument7 pagesProject Report On RTS Juice PlantEIRI Board of Consultants and PublishersNo ratings yet
- O & M of Sub StationDocument94 pagesO & M of Sub StationAlbert Sekar100% (2)
- Types and Symptoms of Common Psychiatric DisordersDocument6 pagesTypes and Symptoms of Common Psychiatric DisordersRanusha AnushaNo ratings yet
- CHAPTER 4 - NotesDocument5 pagesCHAPTER 4 - NotesAquamsha FahimNo ratings yet
- Mood Disorders and SchizophreniaDocument6 pagesMood Disorders and SchizophreniaAdela ChristinaNo ratings yet
- New Disorder - 1Document148 pagesNew Disorder - 1max lifeNo ratings yet
- Mental Disorders: Key FactsDocument9 pagesMental Disorders: Key Factssoshi2691loveNo ratings yet
- General Definition, Causes, and Types of Mental IllnessDocument6 pagesGeneral Definition, Causes, and Types of Mental Illnesszahra03762No ratings yet
- 5 - Childhood Psychiatric Disorder (2017!06!02 23-15-39 UTC)Document60 pages5 - Childhood Psychiatric Disorder (2017!06!02 23-15-39 UTC)drillercz12zNo ratings yet
- Chapter 14 Psychological Disorders.Document9 pagesChapter 14 Psychological Disorders.BorisVanIndigoNo ratings yet
- Mood Disorders OutlineDocument19 pagesMood Disorders OutlineAki HimeNo ratings yet
- Psy 214 Lwcture 7Document27 pagesPsy 214 Lwcture 7Hope MashakeniNo ratings yet
- Unit 1: Psychotherapy: But The Current Definition of Psychotherapy Is Board - I.EDocument59 pagesUnit 1: Psychotherapy: But The Current Definition of Psychotherapy Is Board - I.EabrihamNo ratings yet
- Models of Abnormality in PsychopathologyDocument18 pagesModels of Abnormality in PsychopathologyGift MwapeNo ratings yet
- PSPA3714 Chapter 7 2021Document55 pagesPSPA3714 Chapter 7 2021Kamogelo MakhuraNo ratings yet
- Myths and Facts About Mental Health 022007Document2 pagesMyths and Facts About Mental Health 022007Jemimah AlobaNo ratings yet
- Definition of Terms PDFDocument7 pagesDefinition of Terms PDFkireeeNo ratings yet
- Somatoform DisordersDocument10 pagesSomatoform Disorderssuresh patilNo ratings yet
- Mh-Somatic Symptom Disorders - 2Document9 pagesMh-Somatic Symptom Disorders - 2martinNo ratings yet
- Glossary of Frequently Used Mental Health TermsDocument6 pagesGlossary of Frequently Used Mental Health TermsWarren MillerNo ratings yet
- Psychology Notes Chpt. 13Document5 pagesPsychology Notes Chpt. 13ChloeNo ratings yet
- Behavioural Problem Teennager: Family Medicine SystemDocument23 pagesBehavioural Problem Teennager: Family Medicine SystemSelvi Puspa SariNo ratings yet
- (Parenting) Mental Disorders in ChildrenDocument6 pages(Parenting) Mental Disorders in ChildrenBeatrice StefanNo ratings yet
- DSM 1-5Document46 pagesDSM 1-5Dheeraj Kumar ChhillarNo ratings yet
- PsychosomaticsDocument56 pagesPsychosomaticsrajneesh_shastri10No ratings yet
- Information Factsheet What Is Psychosis?: 2. False BeliefsDocument2 pagesInformation Factsheet What Is Psychosis?: 2. False BeliefsGrace LNo ratings yet
- 02 - Community Mental HealthDocument41 pages02 - Community Mental HealthNinad KupwadeNo ratings yet
- Affective Disorders: Dr. Zeina Adnan Family Medicine SpecialistDocument31 pagesAffective Disorders: Dr. Zeina Adnan Family Medicine SpecialistLamyaa Ali HasanNo ratings yet
- Kring Abnormal Psychology Chapter 5 Mood Disorders NotesDocument14 pagesKring Abnormal Psychology Chapter 5 Mood Disorders NotesAnn Ross FernandezNo ratings yet
- Disorders RushedDocument40 pagesDisorders Rushedapi-391411195No ratings yet
- Abpsych ReviewerDocument17 pagesAbpsych ReviewerAGNER JASMIN ROSE L.No ratings yet
- ADHDDocument21 pagesADHDYuniita VerayantiiNo ratings yet
- 1 - Signs and Symptoms of Mental Illness-PartDocument49 pages1 - Signs and Symptoms of Mental Illness-PartAljoker FarragNo ratings yet
- Schizophrenia LectureDocument20 pagesSchizophrenia LectureKate Lea100% (1)
- Mood Disorders - DepressionDocument58 pagesMood Disorders - Depressionmaha abdallahNo ratings yet
- Signs & Symptoms of An Eating DisorderDocument2 pagesSigns & Symptoms of An Eating DisorderWrendell BrecioNo ratings yet
- Columbia Suicide Severity Rating Scale Screen VersionDocument2 pagesColumbia Suicide Severity Rating Scale Screen VersionPaul SmithNo ratings yet
- Bipolar DisorderDocument1 pageBipolar DisorderNur BalqisNo ratings yet
- Mental Status Exam Template 03Document1 pageMental Status Exam Template 03رجمه ديوان100% (1)
- Function-Memory, Smell And: Persecutory / Paranoid Delusions - Involve TheDocument4 pagesFunction-Memory, Smell And: Persecutory / Paranoid Delusions - Involve TheMark Christian CaasiNo ratings yet
- Typical Signs and Symptoms of Mental Illness 1Document3 pagesTypical Signs and Symptoms of Mental Illness 1Sunny MaeNo ratings yet
- Psych Ch. 7 Notes (Tutor)Document5 pagesPsych Ch. 7 Notes (Tutor)Haylle ThomasNo ratings yet
- PSYCH 9 Reviewer - Chapter 7 Mood Disorders and SuicideDocument5 pagesPSYCH 9 Reviewer - Chapter 7 Mood Disorders and SuicideJoelle Marie GarciaNo ratings yet
- Paradigms of DisordersDocument6 pagesParadigms of DisordersElena-Andreea MutNo ratings yet
- Psych 109 - REVIEWERDocument21 pagesPsych 109 - REVIEWERChanGie Rhyl UbayNo ratings yet
- Paranoid Schizophrenia: OlehDocument52 pagesParanoid Schizophrenia: Olehbunga julia100% (1)
- Copy-Classification of Psychiatric DisordersDocument56 pagesCopy-Classification of Psychiatric Disordersshadrach bineyNo ratings yet
- Mental Status ExamDocument32 pagesMental Status ExamAmit Sen100% (1)
- Dementia Proforma Symptoms Checklist in History For Cognitive DeclineDocument16 pagesDementia Proforma Symptoms Checklist in History For Cognitive DeclineAnand Prakash SinghNo ratings yet
- Vascular DementiaDocument5 pagesVascular DementiaAna Ramos LopezNo ratings yet
- Anxiety Dis. OCD and OtherDocument6 pagesAnxiety Dis. OCD and OtherIsabel CastilloNo ratings yet
- Neural Base EmotionDocument3 pagesNeural Base EmotionClyde Joshua ManatasNo ratings yet
- Typical Signs and Symptoms of Psychiatric Illness DefinedDocument5 pagesTypical Signs and Symptoms of Psychiatric Illness Definedsivab2001ot100% (1)
- Drugs:: Side Effects of Psychotropic MedicationsDocument32 pagesDrugs:: Side Effects of Psychotropic MedicationsMARIE ROSE L. FUNTANARNo ratings yet
- Psych GENDER IDENTITY DISORDERS TRANSDocument8 pagesPsych GENDER IDENTITY DISORDERS TRANSIsabel CastilloNo ratings yet
- Schizo ToolDocument3 pagesSchizo Toolsherell220No ratings yet
- GlossaryDocument8 pagesGlossarysnejinka1979No ratings yet
- Schizophrenia and Other Psychotic Disorders: Southern Philippines Medical CenterDocument44 pagesSchizophrenia and Other Psychotic Disorders: Southern Philippines Medical CenterMaureen JadeNo ratings yet
- Schizophrenia and PsychoticDocument71 pagesSchizophrenia and Psychoticpunzell eonnieNo ratings yet
- Cog Psych ReviewerDocument12 pagesCog Psych ReviewerErika BalaniNo ratings yet
- Autoconceito ShavelsonDocument15 pagesAutoconceito ShavelsonJuliana SchwarzNo ratings yet
- Guide To Laboratory Establishment For Plant Nutrient AnalysisDocument1 pageGuide To Laboratory Establishment For Plant Nutrient AnalysisOsama MadanatNo ratings yet
- Sentinel Collim Rev1.2 CompressedDocument2 pagesSentinel Collim Rev1.2 CompressedBauyrzhanNo ratings yet
- Capinew Account June13Document7 pagesCapinew Account June13ashwinNo ratings yet
- Department of Education: Learning Activity SheetDocument7 pagesDepartment of Education: Learning Activity SheetKaren May UrlandaNo ratings yet
- T N M M T N M M: HE EW Essies Anual HE EW Essies AnualDocument8 pagesT N M M T N M M: HE EW Essies Anual HE EW Essies AnualMunna100% (1)
- Planning and Facilities: Building StorageDocument31 pagesPlanning and Facilities: Building Storagequsai migdadiNo ratings yet
- PhilRice - Fertilizer CalculationDocument21 pagesPhilRice - Fertilizer CalculationMichelle Ann SoledadNo ratings yet
- ECA DatabaseDocument22 pagesECA DatabaseRidhwan JamaludinNo ratings yet
- Emilio Aguinaldo College: School of NursingDocument2 pagesEmilio Aguinaldo College: School of NursingAwani ONo ratings yet
- Why Aws Is Even Better With CloudcheckrDocument7 pagesWhy Aws Is Even Better With CloudcheckrPardha SaradhiNo ratings yet
- Muscular Triangles of The NeckDocument3 pagesMuscular Triangles of The NeckSam TagardaNo ratings yet
- Problem Sets For Solutions AnalysisDocument2 pagesProblem Sets For Solutions AnalysisKamil Guillergan100% (1)
- Normal Wash, Pigment Wash, Caustic WashDocument9 pagesNormal Wash, Pigment Wash, Caustic WashTauhidurRChowdhuryNo ratings yet
- Wired For: Hit Play For SexDocument7 pagesWired For: Hit Play For SexPio Jian LumongsodNo ratings yet
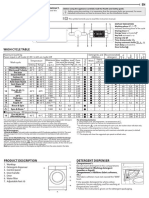
- Whirlpool BIWDWG861484uk enDocument4 pagesWhirlpool BIWDWG861484uk ennadaljoachim77No ratings yet
- Trane Xb13 Packaged Air Conditioner: Your Profit-AbilityDocument2 pagesTrane Xb13 Packaged Air Conditioner: Your Profit-AbilityJesus CantuNo ratings yet
- BRAC Annual Report 2017 PDFDocument116 pagesBRAC Annual Report 2017 PDFShoaib AhmedNo ratings yet
- American FoodDocument10 pagesAmerican FoodEvan BanksNo ratings yet
- Drug Ana Surgery WardDocument11 pagesDrug Ana Surgery WardJames QuilingNo ratings yet
- Ebook Chemistry For Today General Organic and Biochemistry PDF Full Chapter PDFDocument67 pagesEbook Chemistry For Today General Organic and Biochemistry PDF Full Chapter PDFrobert.davidson233100% (31)
- DPP 02 NTSE BY @class - 10 - MaterialsDocument1 pageDPP 02 NTSE BY @class - 10 - MaterialsShashwat MishraNo ratings yet
- Acupressure Points GuidelinesDocument6 pagesAcupressure Points Guidelinesshahisk100% (1)